Scapula Fractures: An Advanced Guide to Epidemiology, Anatomy, & Biomechanics
Key Takeaway
Scapula fractures are uncommon, high-energy injuries often indicating severe associated trauma due to the bone's protected position. Orthopedic management requires understanding detailed surgical anatomy, critical neurovascular structures, and complex biomechanics. Classification systems like AO/OTA and Ideberg are crucial for accurate diagnosis and guiding treatment decisions, ensuring comprehensive patient care.
You are presented with a 35-year-old male involved in a high-speed motorcycle accident. He has an isolated, significantly displaced scapula body and neck fracture. Radiographs show a "floating shoulder" pattern. Describe your approach to the clinical assessment and the role of imaging in your decision-making process.
Candidate: I would start with an ATLS-based assessment to rule out associated thoracic injuries like pneumothorax. For the shoulder, I would order AP, Y-view, and axillary radiographs, followed by a CT scan to look at the fracture pattern and glenoid involvement. I would assess his neurovascular status, specifically checking the brachial plexus and axillary nerve, and then decide if the displacement requires ORIF.
Candidates often jump straight to surgical approaches. They fail to mention the 80-90% association rate with life-threatening chest trauma, neglect to define the "Superior Shoulder Suspensory Complex" (SSSC) concept, or fail to prioritize the systemic "seatbelt sign" trauma assessment.
A high-scoring answer addresses the systemic nature of the injury first. 1. Systemic Priority: Rule out thoracic injuries (pneumothorax/hemothorax) given the high-energy nature. 2. Imaging: Plain films are insufficient; emphasize the 3D CT scan to evaluate the glenoid fossa and SSSC integrity. 3. Surgical Planning: Frame the "floating shoulder" as a disruption of the SSSC—the structural ring composed of the glenoid, coracoid, AC joint, acromion, and distal clavicle. 4. Neurovascular: Specifically mention the high risk of brachial plexus and axillary nerve injury.
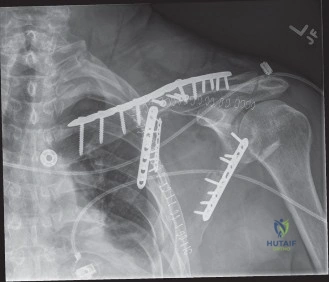
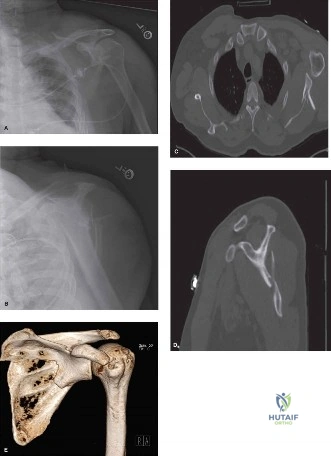
You have decided to proceed with surgery for this patient. This is the pre-operative imaging of the patient. Please interpret these findings and discuss your surgical approach.
Candidate: The CT shows a complex scapular body and neck fracture. I would use a Judet posterior approach to access the glenoid and neck, fix it with locking plates, and be careful not to damage the suprascapular nerve.
Failing to mention the specific internervous plane or ignoring the specific neurovascular structures at risk (suprascapular and axillary nerves). A weak answer also fails to describe the logic behind the plate construct (e.g., creating an "L" or lateral border plate to restore glenoid version).
Demonstrate anatomical mastery: 1. Approach: Choose the Judet approach. Identify the internervous plane between the deltoid (axillary nerve) and infraspinatus (suprascapular nerve). 2. Technique: Mention subperiosteal elevation and the risk to the suprascapular nerve at the spinoglenoid notch. 3. Fixation: Use 3.5mm locking plates along the lateral border of the scapula, potentially combined with spine plating to create a stable, orthogonal construct. 4. Goals: Highlight the importance of restoring the "version" of the glenoid to prevent long-term rotator cuff impingement.
Post-operatively, you review the fixation. What complications would you warn the patient about, and how do you manage them if they occur?
Candidate: I would warn about infection, nerve injury, and shoulder stiffness. If they get an infection, I'd give antibiotics. If they get stiff, I'd tell them to do more physiotherapy.
Vague management plans. "More physiotherapy" is not a management plan for severe post-traumatic stiffness. Failing to mention the specific risk of suprascapular nerve palsy (10-30%) or the impact of hardware prominence on the thin soft tissue coverage of the scapular spine.
Structure the answer by priority: 1. Nerve Palsy: Acknowledge that suprascapular nerve palsy is common (10-30%) and often neuropraxia; monitor with EMG. 2. Stiffness: Distinguish between minor stiffness (early aggressive PT/mobilization) and severe contracture (requiring MUA or arthrolysis). 3. Hardware: Warn about prominence over the spine, often requiring secondary metalwork removal. 4. Infection: Address the need for formal surgical debridement and culture-specific antibiotics for deep infection, rather than just oral antibiotics.
