Optimizing ORIF for Distal Humerus: Prevent Class II HO
Key Takeaway
Your ultimate guide to Optimizing ORIF for Distal Humerus: Prevent Class II HO starts here. Distal humerus fractures result from high-energy trauma in young patients or osteopenia in older adults, often comminuted. Radiographs and CT with 3D reconstruction are crucial for diagnosis and understanding fracture patterns. Internal fixation is the primary treatment, using stable constructs like precontoured plates and locked screws for optimal outcomes, even in complex cases like a severe class ii ho fracture.
Comprehensive Introduction and Patho-Epidemiology
Distal humerus fractures represent a formidable challenge to the orthopedic surgeon, demanding a profound understanding of elbow biomechanics, meticulous surgical technique, and rigorous postoperative management. Epidemiologically, these fractures demonstrate a classic bimodal distribution. The first peak occurs in younger patients, typically males, who sustain high-energy trauma such as motor vehicle collisions, falls from significant heights, or industrial accidents. In this demographic, the soft tissue envelope is often severely compromised, and the fracture pattern is characterized by profound comminution and displacement. The second peak involves older patients, predominantly females, who suffer low-energy falls onto an outstretched hand or directly onto the flexed elbow. In these individuals, underlying osteopenia or frank osteoporosis significantly complicates the ability to achieve rigid internal fixation, often dictating alternative management strategies such as total elbow arthroplasty (TEA).
Comminution is the dominant and most vexing feature of supracondylar and intercondylar fractures (AO/OTA type 13-C). The inherent complexity of the skeletal geometry of the distal humerus—characterized by the diverging medial and lateral columns supporting the articular spool of the trochlea and capitellum—creates a precarious mechanical environment. Historically, severe comminution in this region earned the moniker "bag of bones," and non-operative management was frequently employed, often resulting in profound stiffness and functional impairment. Modern osteosynthesis, however, demands anatomic restoration of the articular surface and rigid stabilization of the columns to the humeral shaft. The overarching goal of the initial evaluation is to meticulously decode the fracture pattern, ascertain the integrity of the soft tissue envelope (especially in open fractures), and identify any concomitant musculoskeletal or neurovascular injuries, particularly involving the ulnar nerve or brachial artery.
A critical, yet often underappreciated, objective in the management of these complex fractures is the prevention of Heterotopic Ossification (HO), specifically Hastings and Graham Class II HO. Class II HO is defined as ectopic bone formation that significantly limits the elbow's arc of motion without progressing to complete ankylosis (Class III). The distal humerus and the surrounding brachialis and triceps musculature are uniquely predisposed to this exuberant osteogenic response following trauma. Optimizing Open Reduction and Internal Fixation (ORIF) is the primary surgical defense against Class II HO. By achieving absolute mechanical stability, the surgeon permits immediate, active, unprotected range of motion (ROM). Early motion prevents the organization of fracture hematoma into a rigid fibrous and eventually osseous matrix, thereby mitigating capsular contracture and ectopic bone deposition.
Furthermore, the initial clinical assessment must delve into the patient's functional demands and pre-existing elbow pathology. Determining the existence of previous symptomatic elbow conditions, such as rheumatoid arthritis, post-traumatic osteoarthritis, or prior ligamentous instability, is paramount. These factors profoundly influence the surgical algorithm, potentially shifting the paradigm from ORIF to TEA in the elderly or rheumatoid patient. The surgeon must also evaluate the proximal radius and ulna, as concomitant injuries (e.g., terrible triad patterns, Monteggia variants) will exponentially increase the complexity of the reconstruction and the risk of postoperative instability and stiffness.

Detailed Surgical Anatomy and Biomechanics
The distal humerus is best conceptualized as a highly specialized architectural triangle or "tie-arch." The medial and lateral columns form the robust pillars of this arch, diverging from the tubular humeral shaft to support the articular segment. The articular segment itself, comprising the trochlea medially and the capitellum laterally, functions as the keystone of the arch. The capitellum is a hemispherical structure projecting anteriorly, articulating with the radial head, while the trochlea is a complex spool-shaped structure covered by hyaline cartilage over a 300-degree arc. This extensive cartilaginous coverage leaves a paucity of non-articular bone available for hardware placement, rendering the fixation of intercondylar fractures exceptionally challenging.
Mechanically, the distal humerus is subjected to tremendous torsional and bending forces during normal activities of daily living. The articulation is anteriorly translated relative to the humeral shaft, with the articular surface tilted approximately 30 degrees anteriorly. Furthermore, it exhibits a natural valgus angulation of 4 to 8 degrees. Failure to restore this precise spatial orientation during ORIF results in altered kinematics, restricted range of motion, and accelerated articular wear. Specifically, inadequate restoration of the anterior tilt will severely limit terminal elbow flexion, while malreduction of the columns can lead to varus or valgus deformity, compromising both cosmetic appearance and functional strength.
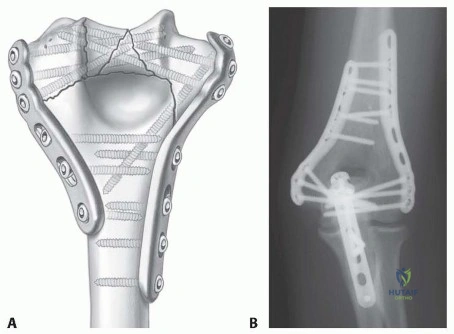
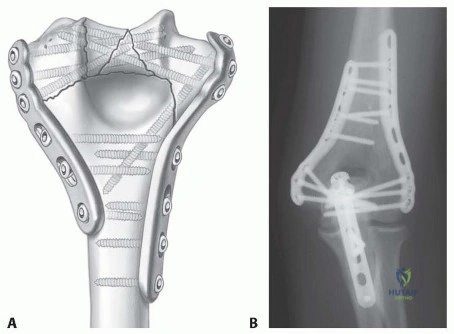
The biomechanical superiority of parallel plating over orthogonal (90-90) plating has been extensively validated in contemporary orthopedic literature, particularly in the setting of osteopenic bone or severe comminution. As elucidated by O'Driscoll, the parallel plate configuration acts as a rigid frame, maximizing the biomechanical stiffness of the construct. By placing plates on the medial and lateral ridges of the columns, the surgeon can pass multiple, long, interdigitating screws through the articular fragments. This creates a structurally sound "dome" of fixation that resists the varus, valgus, and torsional moments applied across the elbow joint during early active rehabilitation.
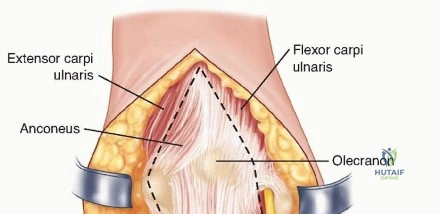
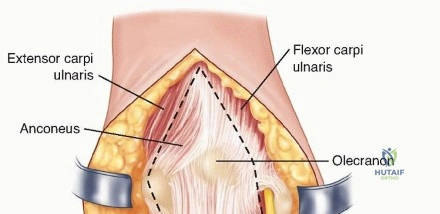
Understanding the surrounding soft tissue anatomy is equally critical to executing a safe and effective ORIF. The ulnar nerve is intimately associated with the posterior aspect of the medial epicondyle, traversing through the cubital tunnel. Its proximity makes it highly vulnerable to iatrogenic injury during medial column exposure and plate application. Posteriorly, the triceps brachii inserts broadly onto the olecranon, and its management dictates the surgical approach. The anconeus muscle, originating from the lateral epicondyle and inserting onto the proximal ulna, provides dynamic stability to the lateral elbow and must be carefully managed or repaired if detached. Additionally, the "bare area" of the greater sigmoid notch of the ulna—a transverse groove devoid of articular cartilage—serves as the precise anatomic landmark for executing a safe olecranon osteotomy.
Exhaustive Indications and Contraindications
Open reduction and internal fixation remains the undisputed gold standard for the vast majority of displaced distal humerus fractures. The primary indication for ORIF is any displaced supracondylar or intercondylar fracture in a physiologically young or active patient where the bone stock is sufficient to hold hardware. The overarching goal is to achieve a construct stable enough to allow immediate, unprotected active motion without fear of catastrophic hardware failure or fracture displacement. Even in cases of extreme comminution (AO/OTA 13-C3), modern pre-contoured locking plate technology allows skilled surgeons to reconstruct the articular spool and securely fasten it to the metaphyseal diaphysis.
However, the indications for ORIF are not absolute, and a paradigm shift has occurred regarding the management of these fractures in the elderly, osteoporotic population. Total elbow arthroplasty (TEA) is now strongly considered—and often preferred—in elderly patients (typically over 65-70 years of age) presenting with severe comminution, profound osteopenia, or pre-existing symptomatic elbow pathology such as rheumatoid arthritis. In these scenarios, the likelihood of achieving stable internal fixation is low, and the risk of nonunion, hardware pullout, and subsequent reoperation is unacceptably high. TEA offers the distinct advantage of immediate stability and early mobilization, bypassing the need for fracture union, albeit with lifelong lifting restrictions.
Absolute contraindications to ORIF include active local or systemic infection, critically compromised soft tissue envelopes that preclude safe surgical incisions (e.g., severe burn eschars or active blistering), and patients who are medically unstable for anesthesia. Relative contraindications include severe cognitive impairment or non-compliance, as the success of ORIF is heavily dependent on the patient's ability to adhere to a strict, phased postoperative rehabilitation protocol. If a patient cannot participate in early active motion, the risk of severe stiffness and Class II HO increases exponentially, potentially rendering the surgical intervention futile.
| Modality | Primary Indications | Relative/Absolute Contraindications |
|---|---|---|
| ORIF | Physiologically young/active patients; Good bone stock; Displaced intra-articular fractures (13-B, 13-C); Extra-articular fractures (13-A) failing closed management. | Extreme osteopenia in the elderly; Pre-existing severe osteoarthritis/rheumatoid arthritis; Active infection; Medically unfit for prolonged surgery. |
| Total Elbow Arthroplasty (TEA) | Elderly (>65-70 yrs) with severe comminution (13-C3); Profound osteoporosis; Pre-existing inflammatory arthropathy; Salvage for failed ORIF. | Young, active patients; High physical demand/heavy laborers; Active infection; Deficient triceps mechanism (relative). |
| Non-Operative (Splint/Cast) | Non-displaced fractures; Patients with absolute medical contraindications to surgery; Bedbound patients with minimal functional demands. | Displaced intra-articular fractures; Open fractures; Concomitant neurovascular compromise. |
Pre-Operative Planning, Templating, and Patient Positioning
Thorough preoperative planning is the cornerstone of successful distal humerus ORIF. The initial imaging sequence must include high-quality anteroposterior (AP) and lateral radiographs of the elbow. These films should be meticulously scrutinized to identify the primary fracture lines, the size and location of the articular fragments, and the degree of metaphyseal comminution. It is imperative to evaluate the joint above and below, specifically looking for associated injuries in the proximal radius and ulna. However, a complete and accurate understanding of the fracture pattern is notoriously difficult to obtain based solely on simple radiographs. The complex, overlapping geometry of the distal humerus, combined with multi-fragmentary comminution, often obscures the true nature of the articular disruption.
Consequently, Computed Tomography (CT) with two-dimensional multiplanar reformats and three-dimensional (3D) surface rendering has become the standard of care for complex distal humerus fractures. 3D CT reconstructions are invaluable; they allow the surgeon to mentally "disassemble" and "reassemble" the fracture prior to making an incision. The CT scan identifies specific osteochondral fragments, such as a coronal shear fragment of the capitellum or a separate trochlear fragment, which might require specialized fixation techniques like headless compression screws. If a CT scan is unavailable, or if the patient is taken emergently to the operating room, traction radiographs obtained under anesthesia just prior to prepping and draping can be highly illuminating, pulling the fragments out of their telescoped positions.

Preoperative templating involves selecting the appropriate hardware systems. Modern fixation relies heavily on pre-contoured, periarticular locking plates designed specifically for the medial and lateral columns. The surgeon should ensure the availability of various plate lengths, as well as 2.7 mm and 3.5 mm locking and non-locking screws. Furthermore, headless compression screws and fine threaded K-wires must be available for the provisional and definitive fixation of small articular fragments. The surgical team should also be prepared with a sterile tourniquet and appropriate bone grafting materials (autograft or allograft) in anticipation of metaphyseal bone voids.
Patient positioning is a critical logistical step that dictates surgical exposure and ease of fluoroscopic imaging. The two primary positions utilized are the lateral decubitus position and the prone position. In the lateral decubitus position, the patient is supported with a beanbag, and the injured arm is draped over a radiolucent post or bolster, allowing the elbow to flex to 120 degrees. This position provides excellent access to the posterior elbow and facilitates easy C-arm positioning. Alternatively, the prone position allows the arm to rest on a radiolucent arm board, which some surgeons prefer for its stability and the ergonomic ease of accessing the posterior structures. Regardless of the position chosen, all bony prominences must be meticulously padded to prevent perioperative neuropraxias, and a sterile tourniquet should be applied high on the brachium.
Step-by-Step Surgical Approach and Fixation Technique
Olecranon Osteotomy
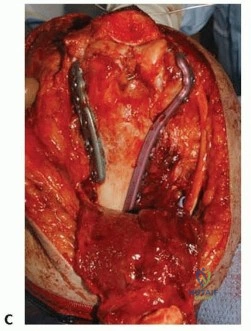
Adequate exposure is the absolute prerequisite for achieving anatomic reduction and rigid fixation of the complex distal humerus. The olecranon osteotomy remains the preferred and most extensile surgical approach for the vast majority of intra-articular distal humerus fractures (AO/OTA 13-C). It provides unparalleled, en face visualization of the articular spool, allowing the surgeon to directly manipulate the trochlea and capitellum. The procedure begins with a posterior midline incision curving around the olecranon. The ulnar nerve is identified, meticulously neurolysed, and protected; whether it is routinely transposed subcutaneously or left in situ remains a topic of spirited debate, though protection throughout the case is universally mandated.
A chevron osteotomy is the preferred configuration, as its V-shape provides inherent rotational stability upon closure. The apex of the chevron is directed distally and is precisely centered over the "bare area" of the greater sigmoid notch—a transverse ridge where articular cartilage is naturally absent. Before initiating the cut, the proximal ulna is pre-drilled and tapped to facilitate anatomic repair later. The osteotomy is initiated with a thin microsagittal saw. Crucially, the saw is only used to cut the dorsal 75% of the bone. The use of a thick saw blade through the entire bone removes excessive stock, making it difficult to achieve interfragmentary compression and increasing the risk of nonunion.

The final 25% of the osteotomy, specifically the subchondral bone and articular surface, is completed by levering a broad osteotome. This technique fractures the remaining bone, creating irregular, interdigitating surfaces that perfectly key into one another during reduction, thereby preserving the articular cartilage and enhancing construct stability. Once the osteotomy is complete, the proximal olecranon fragment, along with the attached triceps tendon, is reflected proximally, granting massive exposure to the distal humerus. The anconeus can be divided in line with the lateral limb of the osteotomy or preserved by dissecting it free and reflecting it with the proximal fragment.
At the conclusion of the humeral fixation, the olecranon osteotomy must be rigidly repaired. Biomechanical studies support various methods, but the combination of a 7.3-mm cancellous screw and a figure-of-eight tension band wire is highly effective. Alternatively, parallel K-wires with a tension band, or a dedicated proximal ulna contoured plate, can be utilized. Plate fixation is increasingly favored in patients with osteopenia or when the osteotomy is comminuted, though it carries a slightly higher risk of symptomatic hardware requiring later removal.

Triceps-Sparing and Reflecting Approaches
For fractures that do not require the absolute maximum exposure provided by an olecranon osteotomy, or in cases where intraoperative conversion to a total elbow arthroplasty is a distinct possibility (e.g., elderly patients with osteopenia), triceps-reflecting approaches are highly advantageous. These approaches preserve the integrity of the proximal ulna, avoiding the complications inherent to osteotomies, such as nonunion or hardware prominence. Furthermore, an intact proximal ulna serves as an invaluable, perfect anatomic template against which the reconstructed distal humeral articular surface can be molded and judged.
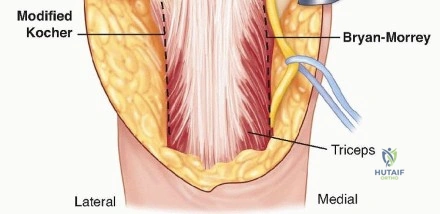
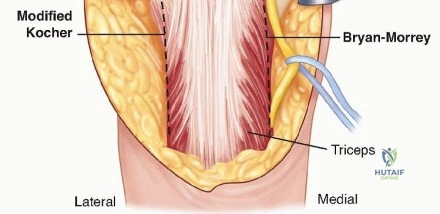
The Bryan-Morrey triceps-sparing approach involves elevating the triceps from the medial intermuscular septum and the posterior aspect of the humeral shaft. The forearm fascia and periosteum are incised just lateral to the flexor carpi ulnaris, and the entire extensor mechanism (triceps, anconeus, and forearm fascia) is reflected subperiosteally in continuity from medial to lateral. Conversely, the Mayo-modified extensile Kocher approach elevates the triceps from the lateral intermuscular septum, reflecting the mechanism from lateral to medial. In both techniques, meticulous care must be taken to preserve the anterior bundle of the medial collateral ligament and the lateral ulnar collateral ligament to prevent catastrophic postoperative instability.
The Bilaterotricipital approach is reserved for simpler fracture patterns (AO/OTA A, C1, C2) or extra-articular distal humerus fractures. In this technique, the surgeon works on both sides of the intact triceps muscle through medial and lateral windows. The triceps is elevated from the medial and lateral intermuscular septae, but its central insertion on the olecranon remains completely undisturbed. This approach significantly decreases surgical time and eliminates complications related to extensor mechanism repair, allowing for aggressive, immediate postoperative rehabilitation. However, its primary disadvantage is the severely limited visualization of the central articular surface, making it inappropriate for complex, multi-fragmentary intra-articular fractures.

Internal Fixation Principles and Execution
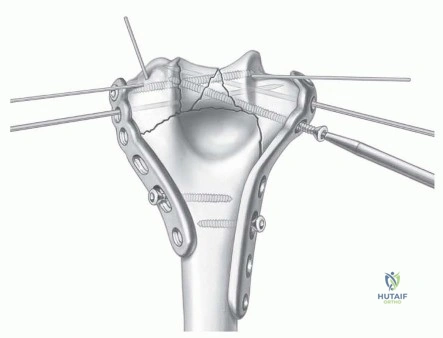
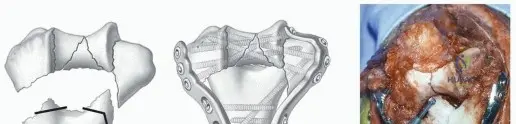
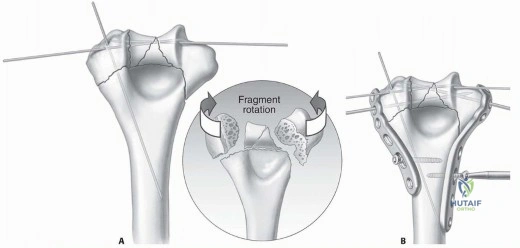
The technical execution of internal fixation for the distal humerus is governed by a strict set of biomechanical principles designed to create an architectural structure mimicking a rigid arch or dome. The primary objective is to place screws in the distal articular fragments such that every screw passes through a plate, and each screw engages a fragment on the opposite side that is also fixed to a plate. The surgeon must strive to place as many screws as possible into the distal fragments, ensuring each screw is as long as possible and engages multiple articular pieces. Crucially, these screws should interdigitate within the distal segment, rigidly linking the medial and lateral columns together.
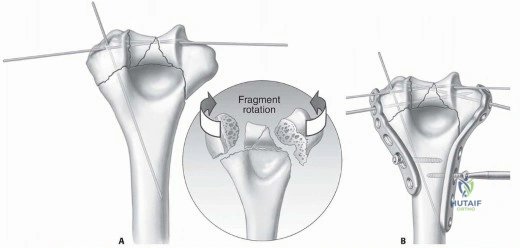
The reconstruction begins with the provisional assembly of the articular surface. The trochlea and capitellum fragments are anatomically reduced, often using the intact proximal ulna and radial head as a template. Rotational alignment is critical and must be verified fluoroscopically. Smooth K-wires (typically 1.5 mm or 2.0 mm) are used to provisionally hold the articular block together. These wires must be placed strategically so they do not interfere with subsequent plate application. Small, fine-threaded wires or headless compression screws may be buried within the articular cartilage for definitive fixation of smaller osteochondral shear fragments.
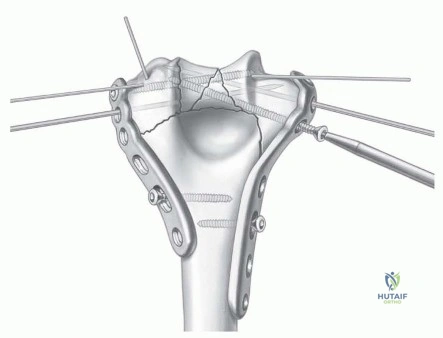
Once the articular block is reconstructed, it must be secured to the humeral diaphysis. Medial and lateral pre-contoured locking plates are applied. Two 2.0-mm smooth wires introduced at the medial and lateral epicondyles can serve as provisional guides, allowing the distal holes of the plates to slide over them. One cortical screw is loosely introduced into a slotted hole on the proximal aspect of each plate to hold them against the humeral shaft, allowing for fine-tuning of plate position. A large bone clamp is then applied to compress the articular fracture lines (unless severe comminution precludes compression), and multiple long, interdigitating locking screws are placed through the plates into the distal segment.
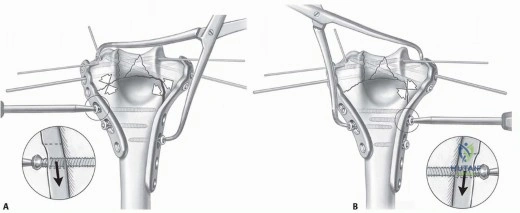
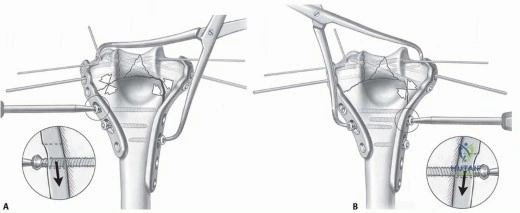
The final, critical step is achieving supracondylar compression. The plates must be applied such that true interfragmentary compression is achieved at the metaphyseal level for both columns. This is accomplished by backing out the proximal screw on one side and applying a large bone clamp distally on that plate and proximally on the opposite side's bone. This maneuver dynamically compresses the reconstructed articular block against the humeral shaft. Compression is then locked in by placing a proximal screw in compression mode. The resulting construct must be strong and stiff enough to resist bending and torsional forces, allowing the patient to begin immediate, unprotected active range of motion.