

Introduction and Epidemiology
Distal humerus fractures represent a complex and challenging subset of orthopedic trauma, demanding a profound understanding of elbow biomechanics, intricate regional anatomy, and advanced osteosynthesis techniques. These injuries are relatively uncommon, comprising approximately 2% of all fractures and roughly one-third of all humerus fractures. The overall incidence of distal humerus fractures in adults is estimated at 5.7 per 100,000 person-years.
Epidemiologically, distal humerus fractures exhibit a classic bimodal age distribution. Peak incidences occur between the ages of 12 and 19 years in young men, typically resulting from high-energy trauma such as motor vehicle collisions or severe sporting accidents. Conversely, the second peak occurs in women aged 80 years and older. In this elderly demographic, greater than 60% of distal humerus fractures occur from low-energy mechanisms, predominantly simple falls from a standing height onto an outstretched hand or a direct blow to the flexed elbow. The osteoporotic nature of the bone in this cohort severely complicates achieving stable internal fixation.
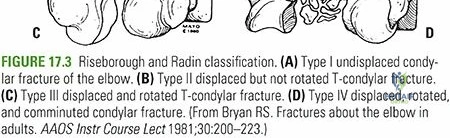
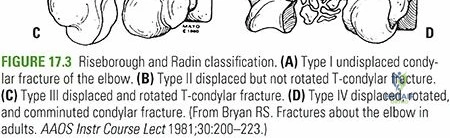
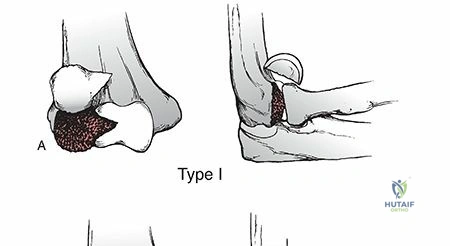
Regarding fracture morphology, extra-articular fractures (AO/OTA Type 13A) account for approximately 40% of these injuries, while bicondylar intra-articular fractures (AO/OTA Type 13C) account for 37%, representing the most common fracture patterns encountered in adult clinical practice. In the pediatric population, the epidemiology shifts dramatically; extension-type supracondylar fractures of the distal humerus account for greater than 80% of all supracondylar fractures in children, necessitating entirely different management algorithms based on physeal anatomy and remodeling potential.
Mechanism of Injury and Clinical Evaluation
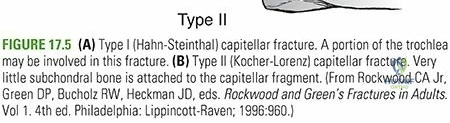
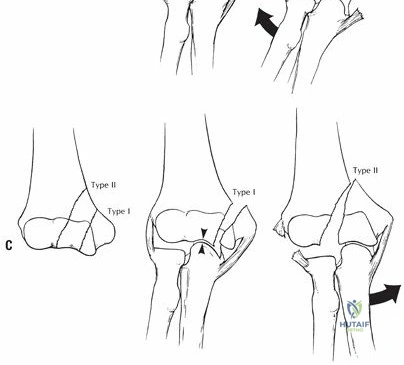
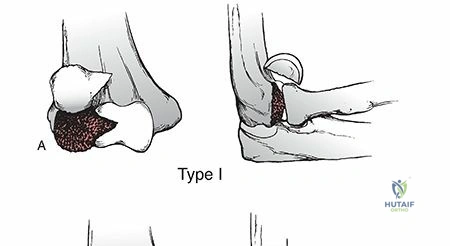
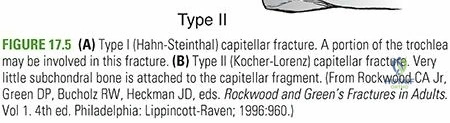
The mechanism of injury dictates the energy imparted to the soft tissue envelope and the resultant fracture comminution. Most low-energy distal humeral fractures in middle-aged and elderly women result from an axial load applied to the outstretched hand or a direct strike to the olecranon. High-energy trauma in younger individuals often produces severe articular comminution, coronal shear fractures of the capitellum and trochlea, and significant soft tissue compromise.
Clinical evaluation must be meticulous. Signs and symptoms vary directly with the degree of swelling and displacement. Considerable soft tissue edema and hemarthrosis frequently occur, rendering standard bony landmarks difficult to palpate. In a normal elbow, the relationship of the olecranon, medial epicondyle, and lateral epicondyle forms an equilateral triangle when the elbow is flexed to 90 degrees; disruption of this triangle indicates articular displacement or elbow dislocation.
While crepitus with range of motion and gross instability may be present and are highly suggestive of fracture, no attempt should be made to elicit these signs. Aggressive manipulation can easily convert a closed injury into an open one or precipitate iatrogenic neurovascular compromise. A careful, documented neurovascular evaluation is essential. The sharp, fractured end of the proximal humeral shaft fragment—particularly in extension-type injuries—may impale, stretch, or contuse the brachial artery, median nerve, or radial nerve.
Surgical Anatomy and Biomechanics
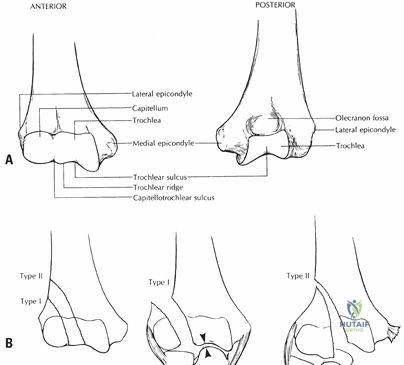
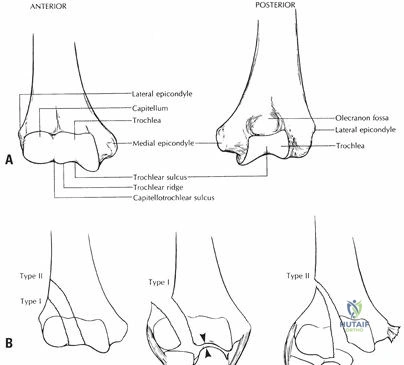
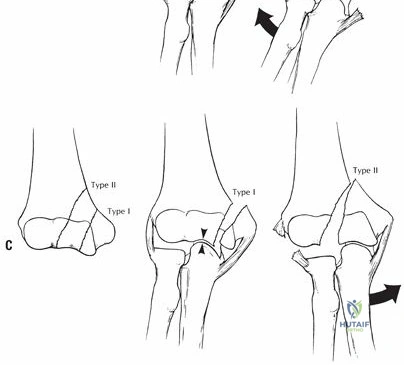
A rigorous conceptualization of distal humerus anatomy is paramount for successful surgical reconstruction. The distal humerus must be conceptualized as two distinct medial and lateral columns, each of which is roughly triangular in shape. Each column is composed of an epicondyle (the nonarticulating terminal of the supracondylar ridge) and a condyle (the articulating unit of the distal humerus). These columns converge proximally into the humeral diaphysis, forming an architectural arch with the articular block acting as the keystone tie-beam.

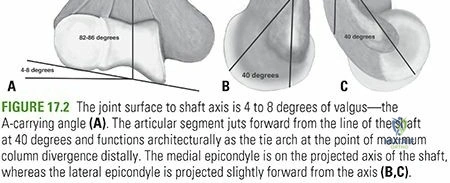
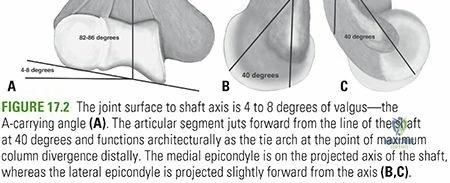
The osseous anatomy of the distal humerus is highly specialized to permit the complex kinematics of the elbow joint. The articulating surface of the capitellum and trochlea projects distally and anteriorly at a 40 to 45 degree angle relative to the longitudinal axis of the humeral shaft. This anterior projection is critical for clearing the coronoid process during terminal elbow flexion.

The center of the arc of rotation of each condyle’s articular surface lies on the exact same horizontal axis. Consequently, any malalignment of the relationships of the condyles to each other alters their arc of rotation, inexorably limiting both flexion and extension and predisposing the joint to early post-traumatic arthrosis.

Angular Relationships and Medullary Anatomy
The trochlear axis, when compared with the longitudinal axis of the humerus, rests in 4 to 8 degrees of valgus. This contributes to the normal carrying angle of the upper extremity. Furthermore, the trochlear axis is 3 to 8 degrees internally rotated. Failure to restore this internal rotation during osteosynthesis can lead to varus malalignment and altered tracking of the ulnohumeral articulation.

From a fixation standpoint, it is critical to recognize that the intramedullary canal of the humerus ends 2 to 3 cm above the olecranon fossa. The bone immediately proximal to the articular surface—comprising the coronoid fossa anteriorly and the olecranon fossa posteriorly—is exceedingly thin. This "waist" of the distal humerus provides virtually no purchase for standard cortical screws, dictating that fixation plates must bypass this region or utilize screws specifically trajectory-planned to capture the dense bone of the medial and lateral columns.
Indications and Contraindications
The management of distal humerus fractures has evolved significantly, with open reduction and internal fixation (ORIF) remaining the gold standard for the vast majority of displaced fractures in physiologically appropriate patients. However, total elbow arthroplasty (TEA) has emerged as a highly effective primary treatment for specific indications, particularly in the elderly osteoporotic patient with severe intra-articular comminution.
| Management Strategy | Primary Indications | Contraindications |
|---|---|---|
| Non-Operative | Truly non-displaced fractures; severely medically compromised patients unfit for anesthesia; non-ambulatory patients with minimal baseline upper extremity functional demands. | Open fractures; vascular compromise; floating elbow; displaced intra-articular fractures in active patients. |
| ORIF | Displaced intra-articular fractures (AO/OTA 13C); displaced supracondylar fractures (13A); open fractures; vascular injuries requiring repair; polytrauma. | Severe osteopenia where stable fixation is impossible; profound soft tissue infection; non-reconstructable articular comminution in the elderly. |
| Total Elbow Arthroplasty | Elderly patients (>65 years) with severe osteopenia and non-reconstructable intra-articular comminution; pre-existing inflammatory arthritis (e.g., Rheumatoid Arthritis). | Young, high-demand patients; laborers; active infection; profound triceps insufficiency; lack of adequate soft tissue coverage. |

Pre Operative Planning and Patient Positioning
Thorough preoperative planning is the cornerstone of successful distal humerus reconstruction. Standard anteroposterior (AP) and lateral radiographs of the elbow are mandatory, though frequently obscured by complex overlapping fracture lines and splint material. Traction radiographs under procedural sedation can be invaluable for delineating fracture fragments.
Currently, a fine-cut Computed Tomography (CT) scan with 3D reconstructions is considered the standard of care for all intra-articular distal humerus fractures. CT imaging allows the surgeon to accurately map coronal shear fragments (e.g., capitellar or trochlear fractures), identify marginal impaction, and template plate positioning.

Patient Positioning Considerations
The patient is typically positioned in either the lateral decubitus or prone position, depending on surgeon preference and concomitant injuries.
- Lateral Decubitus: The patient is placed in the lateral position with the operative arm draped over a well-padded post or an articulated arm holder. This allows excellent access to the posterior elbow and facilitates gravity-assisted reduction. It is highly favored for isolated elbow trauma.
- Prone Position: The patient lies prone with the arm resting on a radiolucent arm board. This provides excellent visualization and is particularly useful if concomitant posterior approaches to the shoulder or lower extremity procedures are required. However, airway management and ventilation require meticulous anesthesia coordination.
In both positions, a sterile tourniquet is applied high on the brachium. The C-arm fluoroscopy unit must be positioned to allow unobstructed AP and lateral views throughout the procedure without compromising the sterile field.

Detailed Surgical Approach and Technique
The surgical approach to the distal humerus must provide adequate exposure for anatomic articular reduction while minimizing morbidity to the extensor mechanism and critical neurovascular structures. The universal posterior incision is standard, typically curving slightly laterally around the tip of the olecranon to prevent painful scar formation over the bony prominence.

Management of the Ulnar Nerve
Regardless of the deep approach utilized, the ulnar nerve must be identified, neurolysed, and protected early in the procedure. The nerve is located in the cubital tunnel posterior to the medial epicondyle. The first motor branch to the flexor carpi ulnaris must be preserved. Whether to perform an in-situ decompression or a formal anterior transposition (subcutaneous or submuscular) remains debated. Transposition is generally indicated if the hardware impinges on the nerve's native bed, if there is pre-existing cubital tunnel syndrome, or if the nerve subluxates during flexion post-release.
Deep Surgical Approaches
Several options exist for addressing the extensor mechanism to access the joint:
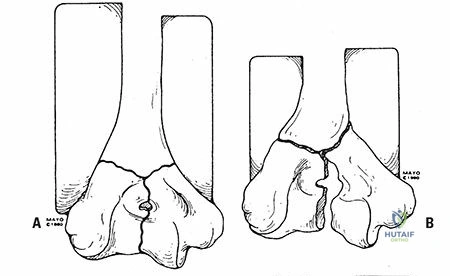
- Olecranon Osteotomy: The gold standard for complex AO/OTA 13C3 fractures. An apex-distal chevron osteotomy is performed through the bare area of the greater sigmoid notch. This provides unparalleled visualization of the articular surface. The osteotomy is later repaired using tension band wiring or a dedicated olecranon plate.
- Triceps-Sparing (Paratricipital / Alonso-Llames): Involves working through the medial and lateral windows on either side of the triceps. Ideal for extra-articular fractures (13A) or simple intra-articular splits (13C1) where extensive articular visualization is not required.
- Triceps-Reflecting (Bryan-Morrey): The triceps is elevated off the olecranon from medial to lateral in continuity with the anconeus and forearm fascia. Provides good exposure and avoids an osteotomy, but requires meticulous soft tissue repair and may limit early active extension.
- Triceps-Splitting (Campbell): A midline split through the triceps tendon. Rarely used for complex trauma due to limited articular visualization and potential for extensor mechanism scarring.
Reduction and Fixation Strategy
The surgical sequence follows a strict algorithmic approach: "Build the spool, then attach the spool to the shaft."
- Articular Reduction: The trochlea and capitellum are anatomically reduced and provisionally held with smooth K-wires. Definitive fixation of the articular block is achieved with headless compression screws or countersunk cortical screws placed from lateral to medial (or vice versa), ensuring they do not violate the olecranon or coronoid fossae.
- Column Fixation: Once the articular block is reconstituted, it is reduced to the humeral diaphysis. This requires dual plating. Biomechanical studies have extensively debated orthogonal (one medial, one posterolateral) versus parallel (one medial, one lateral) plating.
- Parallel Plating: Biomechanically superior for resisting axial loads and torsional forces, particularly in comminuted or osteoporotic bone. It relies on the architectural principle of creating a rigid arch.
- Orthogonal Plating: Often technically easier for specific fracture patterns and provides excellent stability for apex-posterior bending forces.
According to the principles popularized by O'Driscoll for parallel plating, the surgeon must aim to maximize screw length in the distal fragments, ensure screws interlock to create a fixed-angle construct, and apply the plates under compression to offload the hardware.
Complications and Management
Distal humerus fractures are fraught with potential complications, both from the initial trauma and the surgical intervention. The complex regional anatomy and the elbow's inherent propensity for capsular contracture make complication management a routine part of postoperative care.
| Complication | Incidence | Etiology and Management Strategy |
|---|---|---|
| Elbow Stiffness | >50% (Most Common) | Due to capsular fibrosis, intrinsic articular damage, or prolonged immobilization. Management: Aggressive early ROM, static progressive splinting. Open or arthroscopic capsular release is indicated if functional arc (< 100 degrees) is not achieved by 6 months. |
| Ulnar Neuropathy | 10% - 25% | Direct trauma, iatrogenic traction, or hardware impingement. Management: Careful intraoperative handling. Postoperative neuropathy is initially observed; if progressive or failing to improve, surgical exploration, neurolysis, and anterior transposition are indicated. |
| Nonunion | 2% - 10% | Inadequate fixation, severe comminution, or infection. Supracondylar level is most common. Management: Revision ORIF with dual plating, rigid compression, and autologous bone grafting. TEA is a salvage option in the elderly. |
| Heterotopic Ossification (HO) | 3% - 10% | High-energy trauma, delayed surgery, traumatic brain injury. Management: Prophylaxis with Indomethacin or single-dose radiation in high-risk patients. Excision is delayed until HO is radiographically mature (typically 6-12 months) and a normal alkaline phosphatase level is achieved. |
| Hardware Failure | < 5% | Failure to adhere to biomechanical principles (e.g., using single plate, inadequate distal screw purchase). Management: Revision osteosynthesis or conversion to TEA depending on patient age and bone stock. |
Infection, while less common than stiffness or neuropathy, is a devastating complication. Deep surgical site infections require aggressive serial debridement, hardware retention if stability is maintained and the fracture is healing, or hardware removal and placement of an antibiotic spacer if fixation is lost.
Post Operative Rehabilitation Protocols
The overriding philosophy of postoperative rehabilitation following distal humerus ORIF is the immediate institution of motion to prevent catastrophic stiffness. The elbow joint capsule is highly sensitive to trauma and immobilization, rapidly developing thick, unyielding scar tissue.
Phase 1: Immediate Postoperative (0-2 Weeks)
The arm is typically placed in a well-padded posterior splint in 60 to 90 degrees of flexion immediately post-op to allow soft tissue rest. However, this splint should ideally be removed within 3 to 7 days to commence active-assisted range of motion (AAROM) and active range of motion (AROM) exercises. Gravity-assisted extension and supine overhead flexion are emphasized. If an olecranon osteotomy or triceps-reflecting approach was utilized, active extension against resistance is strictly prohibited to protect the extensor mechanism repair.
Phase 2: Intermediate (2-6 Weeks)
Sutures are removed. The patient progresses with AROM and AAROM. Edema control is critical. Nighttime extension splinting may be initiated if the patient demonstrates an extension lag or early flexion contracture. The goal by the end of this phase is to achieve a functional arc of motion (30 to 130 degrees of flexion).
Phase 3: Late (6-12+ Weeks)
Radiographic evaluation should demonstrate early bridging callus or obliteration of fracture lines. Once clinical and radiographic union is progressing, progressive resistance exercises (PREs) and formal strengthening are introduced. If stiffness persists despite therapy, turnbuckle or static progressive splinting is utilized. Maximum medical improvement regarding range of motion may take up to 12 to 18 months.
Summary of Key Literature and Guidelines
The academic discourse surrounding distal humerus fractures is robust, with several pivotal studies guiding contemporary surgical algorithms.
The biomechanical superiority of parallel plating was definitively established by O'Driscoll et al., who demonstrated that dual parallel plates, linked via the articular fragments, construct an architectural arch that is significantly stiffer in axial compression and torsion compared to orthogonal constructs. This has shifted the paradigm, particularly for highly comminuted 13C3 fractures.
However, clinical outcome studies, such as the randomized controlled trial by Lee et al., have shown no statistically significant difference in functional outcomes or union rates between parallel and orthogonal plating systems when strict surgical principles are applied. The choice often
Clinical & Radiographic Imaging








Detailed Chapters & Topics
Dive deeper into specialized chapters regarding distal-humerus-fractures