Latarjet Glenoid Reconstruction: A Masterclass in Anterior Shoulder Instability with Bone Loss
Key Takeaway
This masterclass details the Latarjet procedure for anterior shoulder instability with glenoid bone loss. Fellows will learn comprehensive surgical anatomy, precise preoperative planning, and granular intraoperative execution from a master surgeon's perspective. We cover coracoid osteotomy, subscapularis splitting, glenoid preparation, and meticulous graft fixation, emphasizing neurovascular protection, critical pearls, and complication management for optimal patient outcomes.
Comprehensive Introduction and Patho-Epidemiology
Welcome, colleagues, fellows, and residents, to this definitive masterclass on the Latarjet procedure. Today, we are tackling one of the most challenging yet highly rewarding surgical interventions in our armamentarium: the open Latarjet glenoid reconstruction for recurrent anterior shoulder instability associated with significant glenoid bone loss. Originally described by Dr. Michel Latarjet in 1954, and subsequently modified by pioneers such as Patte and Walch, this technique has stood the test of time. It remains the gold standard for restoring stability in patients where arthroscopic soft-tissue stabilization is destined to fail. This procedure offers a robust, dynamic solution, particularly vital for high-demand contact athletes, military personnel, or patients presenting with substantial anteroinferior bony defects.
The epidemiology of anterior shoulder instability dictates a nuanced understanding of failure rates associated with isolated Bankart repairs. While arthroscopic capsulolabral repair is highly successful in the absence of bone loss, the presence of significant glenoid or bipolar bone loss fundamentally alters the biomechanical landscape. Studies have consistently demonstrated that arthroscopic stabilization in patients with greater than 15% to 20% glenoid bone loss yields unacceptably high recurrence rates, often exceeding 60% in young, competitive contact athletes. Recognizing this demographic is paramount; we are not merely treating a dislocating joint, but restoring the functional capacity of an individual whose lifestyle demands absolute shoulder stability under extreme physiological loads.
Understanding the pathogenesis of glenoid bone loss is critical for proper surgical indication. Anterior glenoid bone loss arises from either the acute, catastrophic impaction of the humeral head against the anterior glenoid rim during a high-energy dislocation (resulting in a bony Bankart fracture) or from the chronic, insidious erosion and abrasive wear caused by recurrent subluxations. This repetitive micro-trauma transforms the native "pear-shaped" glenoid into an "inverted pear," drastically reducing the surface area available for concavity compression. Furthermore, we must consider the concept of the "glenoid track." When a Hill-Sachs lesion engages the anterior glenoid rim during abduction and external rotation, the joint is biomechanically doomed to dislocate unless the anterior glenoid arc is restored.
The Latarjet procedure is far more than a simple bone block; it is an elegant, multi-faceted dynamic stabilization technique. By transferring the coracoid process along with its attached conjoint tendon to the anteroinferior glenoid neck, we fundamentally alter the local anatomy to prevent anterior humeral translation. As we delve into the intricacies of this procedure, from precise preoperative templating to the meticulous execution of the subscapularis split and graft fixation, you will appreciate why the Latarjet remains an indispensable tool for the complex shoulder surgeon.
Detailed Surgical Anatomy and Biomechanics
The Triple Blocking Effect
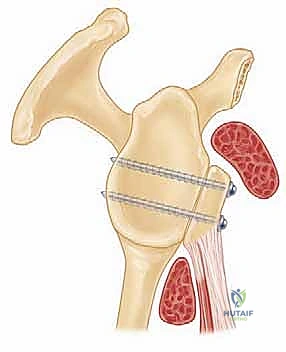
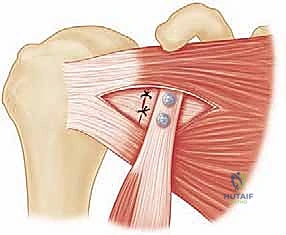
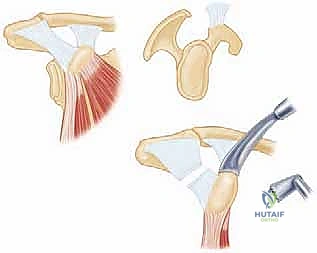
Before we make our deltopectoral incision, it is imperative to deeply comprehend the biomechanics that render the Latarjet procedure so extraordinarily effective. The French shoulder surgeon Denis Patte eloquently described this mechanism as the "triple blocking effect." This triad of stabilizing forces works synergistically to prevent anterior humeral head translation, even in the face of massive capsuloligamentous deficiency. The first component is the Anterior Bone Block Effect. By transferring the osteotomized coracoid process and securely fixing it flush to the anterior glenoid rim, we physically reconstruct the lost osseous architecture. This effectively restores the native pear shape of the glenoid, extending the articular arc and increasing the surface area required for effective concavity compression by the rotator cuff.
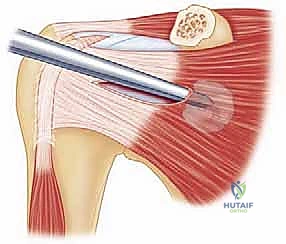
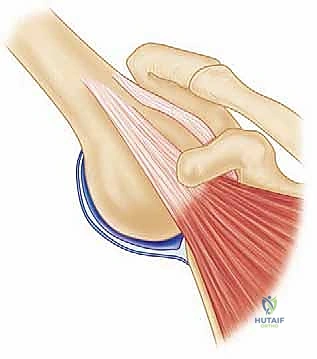
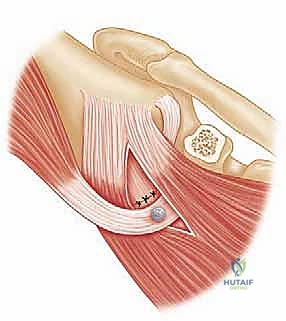
The second, and arguably the most uniquely powerful component, is the Conjoint Tendon Sling Effect. The conjoint tendon, comprising the short head of the biceps and the coracobrachialis, remains attached to the transferred coracoid graft. As this graft is repositioned to the anteroinferior glenoid, the tendon is routed through the split subscapularis muscle. When the patient's arm is placed in the vulnerable position of abduction and external rotation (the classic apprehension position), this tendon becomes taut. It acts as a dynamic, tensioned sling that forcefully compresses the inferior subscapularis muscle belly and the underlying anteroinferior capsule directly against the humeral head, physically barring it from anterior subluxation.
The third component is the Capsular Repair Effect. During the coracoid preparation, we deliberately preserve a robust stump of the coracoacromial (CA) ligament attached to the lateral aspect of the graft. After the bone block is rigidly fixed to the glenoid neck, the native anterior joint capsule—or the lateral leaf of the subscapularis if the capsule is deficient—is meticulously sutured to this CA ligament stump. This step effectively re-tensions the anterior capsular structures, obliterates any redundant anterior recess, and provides a reinforced static restraint that complements the dynamic sling and the bony buttress.
The synergy of these three mechanisms ensures that the Latarjet is not solely reliant on bony union for success. Even in the rare event of a fibrous nonunion of the bone graft, the dynamic sling and capsular repair often provide sufficient stability to prevent recurrent dislocation. This redundancy is what makes the procedure uniquely resilient and particularly suited for high-collision athletes.
Glenohumeral Articular Anatomy
A profound mastery of the regional osseous and soft-tissue anatomy is non-negotiable for the successful execution of the Latarjet procedure. The native glenoid fossa is typically pear-shaped, wider inferiorly than superiorly, with an average superoinferior height of 35 mm and an anteroposterior width of 25 mm in the lower half. The articular surface is slightly retroverted and relies heavily on the fibrous glenoid labrum to deepen the socket by approximately 50%, significantly enhancing the concavity compression mechanism. Anterior glenoid bone loss preferentially obliterates the wider, inferior portion of the glenoid, functionally converting it into an "inverted pear" and drastically reducing the joint's tolerance to anterior shear forces.
The inferior glenohumeral ligament (IGHL) complex is the primary static stabilizer against anterior translation when the arm is abducted and externally rotated. The anterior band of the IGHL typically originates from the anteroinferior glenoid labrum, between the 2 o’clock and 4 o’clock positions (in a right shoulder). In chronic instability, this ligamentous complex is often plastically deformed, avulsed (Bankart lesion), or medially displaced and scarred down the scapular neck (ALPSA lesion). Recognizing the state of the IGHL is crucial, as the Latarjet procedure will bypass the need for a direct anatomic labral repair, relying instead on the triple blocking effect to substitute for this deficient static restraint.
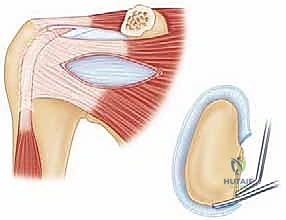
The articular cartilage of the glenoid must be meticulously respected during the procedure. When preparing the anterior glenoid neck to receive the coracoid graft, the decortication must be perfectly flush with, but not violate, the articular cartilage margin. If the graft is placed too laterally (proud), it will inevitably lead to rapid, catastrophic abrasive wear of the humeral head cartilage, resulting in severe secondary osteoarthritis. Conversely, if placed too medially, the bone block effect is negated, and the joint remains unstable.
Furthermore, the surgeon must appreciate the capsular reflections. The anterior capsule inserts onto the labrum and the glenoid neck. During the approach, a vertical capsulotomy is required to expose the joint. The quality of this capsular tissue dictates the final step of the triple block; robust capsular tissue allows for a strong repair to the CA ligament stump, while attenuated tissue may require incorporation of the subscapularis tendon for adequate anterior closure.
Coracoid Process and Musculotendinous Intervals
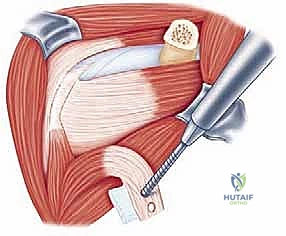
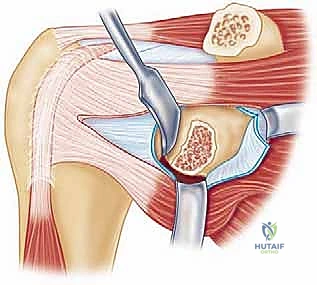
The coracoid process is a complex, multi-functional osseous prominence arising from the superior border of the anterior scapular neck. It projects anteriorly before hooking laterally and inferiorly. For the Latarjet procedure, we are primarily concerned with the horizontal distal segment. At its apex, the coracoid serves as the origin for the conjoint tendon. Medially, it receives the insertion of the pectoralis minor muscle, which must be carefully released to mobilize the graft. Laterally, it anchors the coracoacromial (CA) and coracohumeral ligaments.
The osteotomy site is critical. It must be performed at the "knee" of the coracoid—the anatomical transition point where the horizontal process meets the vertical base. This location is chosen to yield a graft of approximately 2.5 to 3.0 centimeters in length. Crucially, the osteotomy must remain distal to the insertions of the conoid and trapezoid ligaments (the coracoclavicular ligaments). Violating these ligaments during the osteotomy or subsequent dissection will result in iatrogenic acromioclavicular joint instability, a highly undesirable complication.
Surgical access is achieved via the deltopectoral interval, the workhorse approach to the anterior shoulder. This internervous plane lies between the deltoid (axillary nerve) and the pectoralis major (medial and lateral pectoral nerves). The cephalic vein, typically running within this groove, must be identified and meticulously protected. While it can be retracted medially or laterally, lateral retraction with the deltoid is generally preferred as it preserves the major venous tributaries draining the deltoid muscle, reducing postoperative edema.
Deep to the deltopectoral fascia lies the subscapularis muscle, the anterior dynamic stabilizer of the glenohumeral joint. Historically, the Latarjet utilized a vertical tenotomy of the subscapularis. However, modern techniques mandate a horizontal subscapularis split, parallel to its muscle fibers, typically at the junction of the middle and inferior thirds. This muscle-splitting approach is paramount; it preserves the integrity of the subscapularis tendon insertion, maintains its dynamic function, and allows the conjoint tendon to pass through the split, creating the essential dynamic sling effect without compromising internal rotation strength.
Neurovascular Structures at Risk
The Latarjet procedure demands meticulous dissection due to the intimate proximity of several critical neurovascular structures. The most vulnerable nerve during the initial phases of the operation is the Musculocutaneous Nerve. This nerve typically penetrates the conjoint tendon from its medial aspect, entering the deep surface of the coracobrachialis. Its entry point is highly variable, averaging 5 cm distal to the coracoid tip, but it can be as proximal as 1.5 cm. Aggressive distal retraction of the conjoint tendon, or blind sweeping maneuvers on its medial side, can cause traction neuropraxia or direct transection, resulting in profound biceps weakness and sensory loss over the lateral forearm.
The Axillary Nerve is the second major neurological structure at risk, particularly during the deeper stages of the exposure. It courses anterior to the subscapularis muscle, lying lateral to the axillary artery, before diving posteriorly into the quadrilateral space at the inferior margin of the subscapularis. During the subscapularis split and the placement of inferior glenoid retractors (such as a Fukuda or Hohmann retractor), the axillary nerve is highly susceptible to compression or traction. To mitigate this risk, retractors must always be placed strictly subperiosteally along the inferior scapular neck, ensuring the nerve remains protected within the soft tissue envelope.
Medial to the conjoint tendon lie the major vessels: the Axillary Artery and Vein, along with the cords of the brachial plexus. While these structures are generally protected by their medial position, catastrophic injury can occur if dissection strays too far medially or if a drill bit plunges excessively deep during glenoid preparation. The surgeon must maintain a strict lateral and anterior orientation, keeping the conjoint tendon as a protective barrier between the operative field and the axillary sheath.
Finally, the Suprascapular Nerve must be considered during the drilling and fixation of the coracoid graft to the glenoid. The nerve courses through the spinoglenoid notch on the posterior aspect of the scapular neck. If the drill trajectory is aimed too far medially or posteriorly, the drill bit or the subsequent screws can penetrate the posterior scapular cortex and injure the nerve, leading to devastating infraspinatus paralysis. A trajectory strictly parallel to the articular surface is mandatory to avoid this complication.
Exhaustive Indications and Contraindications
The decision to proceed with a Latarjet reconstruction over an arthroscopic soft-tissue repair requires a rigorous, evidence-based evaluation of the patient's clinical profile and pathoanatomy. The Instability Severity Index Score (ISIS), popularized by Boileau and Balg, remains a cornerstone in this decision-making process. Patients scoring over 6 points on the ISIS are statistically highly likely to fail isolated arthroscopic Bankart repair and are prime candidates for a Latarjet.
Primary indications include recurrent anterior glenohumeral instability in the presence of critical glenoid bone loss (generally defined as >15-20% of the inferior glenoid width). However, the Latarjet is also strongly indicated in patients with "subcritical" bone loss (10-15%) who possess high-risk profiles: competitive contact athletes (rugby, American football, martial arts), military special operators, and individuals engaged in heavy manual labor. Furthermore, the Latarjet is the salvage procedure of choice for patients presenting with failed prior arthroscopic or open soft-tissue stabilization procedures, regardless of the precise percentage of bone loss.
Contraindications must be strictly observed to prevent disastrous outcomes. Absolute contraindications include voluntary, habitual shoulder instability driven by psychological factors, as these patients will inevitably stress and fail any surgical construct. Multidirectional instability (MDI) characterized by profound global capsular hyperlaxity, in the absence of a distinct structural bony Bankart lesion or traumatic etiology, is generally a contraindication; these patients are better served by capsular plication and intensive rehabilitation.
Relative contraindications include advanced glenohumeral osteoarthritis, where a Latarjet may exacerbate joint stiffness and pain without addressing the primary degenerative pathology. Patients with uncontrolled seizure disorders pose a unique challenge; while a Latarjet is mechanically stronger than a Bankart repair, a massive grand mal seizure can still fracture the graft or pull out the hardware. In such cases, optimization of medical management is required prior to any surgical intervention. Advanced age is a relative contraindication, not strictly due to chronologic age, but because older patients generally have lower physical demands and may suffer from concomitant rotator cuff arthropathy, altering the surgical algorithm.
| Clinical Parameter | Indication for Latarjet | Contraindication for Latarjet |
|---|---|---|
| Glenoid Bone Loss | > 15-20% (Critical Bone Loss) | < 10% in a low-demand patient |
| Patient Profile | Contact athlete, heavy laborer, military | Sedentary lifestyle, low physical demand |
| Prior Surgery | Failed arthroscopic Bankart repair | First-time dislocation without bone loss |
| Instability Type | Traumatic, unidirectional anterior | Voluntary, habitual, or multidirectional (MDI) |
| Concomitant Pathology | Engaging Hill-Sachs lesion (Off-track) | Severe glenohumeral osteoarthritis |
| Neurological Status | Intact axillary and musculocutaneous nerves | Uncontrolled seizure disorder |
Pre-Operative Planning, Templating, and Patient Positioning
Clinical Evaluation and Diagnostic Imaging
A meticulous preoperative clinical evaluation sets the stage for surgical success. The history must detail the mechanism of the initial dislocation, the frequency of recurrences, the ease of reduction, and the specific arm positions that provoke apprehension. Physical examination should confirm anterior instability via the Anterior Apprehension and Relocation tests. Crucially, the surgeon must evaluate for signs of global hyperlaxity, assessing the sulcus sign, generalized joint hypermobility (Beighton score), and the Gagey hyperabduction test. An asymmetric difference in passive abduction of more than 20-30 degrees strongly implies severe inferior glenohumeral ligament incompetence. A rigorous neurovascular exam, specifically testing deltoid function (axillary nerve) and biceps strength/lateral forearm sensation (musculocutaneous nerve), must be documented preoperatively.
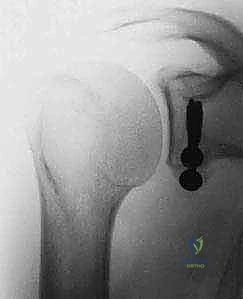
Diagnostic imaging is the cornerstone of surgical templating. Standard plain radiographs must include a true anteroposterior (Grashey) view, an axillary lateral, and a Stryker notch view to assess for Hill-Sachs lesions. The Bernageau profile view, though technically demanding for radiology technicians, is an excellent traditional method for visualizing anterior glenoid deficiency. However, advanced imaging is now considered mandatory for precise surgical planning.
A non-contrast Computed Tomography (CT) scan with 3D reconstructions and digital subtraction of the humeral head is the gold standard for quantifying glenoid bone loss. The en face 3D view of the glenoid allows the surgeon to clearly visualize the "cliff sign" and accurately measure the defect utilizing the best-fit circle method over the inferior glenoid. Furthermore, CT imaging allows for the calculation of the "glenoid track," integrating the size of the glenoid defect with the dimensions of the Hill-Sachs lesion to determine if the lesion is "on-track" or "engaging" (off-track). An off-track lesion is a definitive indication for a Latarjet procedure. Magnetic Resonance Imaging (MRI) or MR Arthrography is useful as an adjunct to evaluate the integrity of the rotator cuff, the long head of the biceps, and the presence of SLAP tears, though these soft-tissue pathologies rarely alter the decision to proceed with the bony reconstruction.


Anesthesia and Patient Positioning
Optimal patient positioning and anesthetic management are critical for facilitating exposure and minimizing complications. The procedure is performed under general endotracheal anesthesia. We strongly advocate for the concurrent use of a regional interscalene nerve block, administered preoperatively by the anesthesia team under ultrasound guidance. This provides profound intraoperative muscle relaxation, decreasing the need for paralytic agents, and ensures excellent postoperative analgesia, facilitating early mobilization.
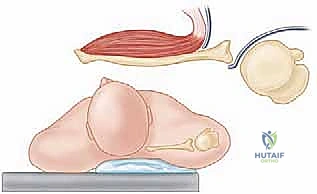
The patient is positioned in a modified beach-chair position. The back of the bed is elevated to approximately 45 to 60 degrees, and the patient's head is secured in a specialized headrest, ensuring the cervical spine remains in a neutral position without excessive lateral flexion or rotation. The operative shoulder must be positioned completely free of the lateral edge of the bed to allow for unrestricted arm extension, which is vital for delivering the glenoid later in the procedure.
A critical maneuver in positioning is the "scapular protraction reduction." A folded surgical towel or a commercially available scapular bump is placed firmly underneath the medial border of the ipsilateral scapula. This bump prevents the scapula from falling posteriorly into protraction. By stabilizing the scapula, we effectively push the glenohumeral joint anteriorly and medially, dramatically improving our surgical access to the anterior glenoid neck and making the subscapularis split significantly easier. The arm is prepped and draped free in a sterile fashion, utilizing a U-drape and an impervious stockinette, allowing the surgical assistant to manipulate the limb dynamically throughout the case.

Step-by-Step Surgical Approach and Fixation Technique
Deltopectoral Approach and Coracoid Preparation
The operation commences with a standard deltopectoral incision, typically 5 to 7 centimeters in length, originating just distal to the coracoid process and extending towards the deltoid tuberosity. Subcutaneous tissues are divided, and the deltopect
Clinical & Radiographic Imaging Archive