Knee Arthroscopy Masterclass: Comprehensive Intraoperative Techniques & Anatomy

Key Takeaway
This masterclass guides fellows through knee arthroscopy, covering comprehensive anatomy of the tibiofemoral and patellofemoral joints, menisci, and crucial ligaments. We detail preoperative planning, patient positioning, and meticulous portal placement. Learn step-by-step diagnostic arthroscopy, identifying pathologies in the suprapatellar pouch and assessing patellar tracking, all from a master surgeon's perspective.
Comprehensive Introduction and Patho-Epidemiology
Welcome, colleagues and fellows, to the definitive masterclass on knee arthroscopy. What was once considered a mere diagnostic adjunct in the mid-20th century has evolved into a foundational, highly sophisticated video-assisted surgical intervention. Knee arthroscopy is now the cornerstone of intra-articular disease management, demanding an amalgamation of profound anatomical knowledge, refined spatial awareness, and meticulous manual dexterity. The transition from open arthrotomy to minimally invasive arthroscopic techniques represents one of the most significant paradigm shifts in modern orthopedic surgery, drastically reducing surgical morbidity, accelerating functional recovery, and allowing for dynamic, magnified visualization of intra-articular pathology.
The patho-epidemiology of knee disorders necessitating arthroscopic intervention is vast and varied. Meniscal tears remain the most frequent indication, with an estimated incidence of 60 to 70 cases per 100,000 person-years. These injuries span a bimodal distribution: acute, traumatic tears predominantly affecting the young, active demographic, and degenerative tears afflicting the older population. Furthermore, anterior cruciate ligament (ACL) ruptures, affecting approximately 200,000 individuals annually in the United States alone, rely heavily on arthroscopic techniques for precise anatomical reconstruction. Chondral defects, synovial proliferative disorders, and the presence of intra-articular loose bodies further contribute to the high volume of these procedures performed globally.
Mastering this procedure requires moving beyond a simple mechanical understanding of instrumentation. The arthroscope is an extension of the surgeon's eye, and the instruments are extensions of the surgeon's hands. To navigate the complex, tri-compartmental architecture of the knee safely and effectively, one must possess an internalized, three-dimensional map of the joint's anatomy and biomechanics. Every incision, every instrument pass, and every therapeutic maneuver must be dictated by a profound respect for the physiological environment of the knee. Our goal is not merely to resect pathology, but to restore biomechanical harmony and preserve joint longevity.
Detailed Surgical Anatomy and Biomechanics
Let us begin by deconstructing the intricate architecture of the knee joint. The knee is a modified hinge joint, governed by a complex interplay of osseous geometry, ligamentous restraints, and meniscal load-sharing. A profound understanding of these elements is the absolute prerequisite for safe and efficacious arthroscopic surgery.
The Tibiofemoral Articulation
The tibiofemoral articulation is biomechanically divided into the medial and lateral compartments, each possessing distinct morphological and kinematic properties.
The medial tibial plateau is a critical load-bearing structure. In the sagittal plane, it exhibits a larger anteroposterior dimension compared to its lateral counterpart. It presents a concave articular surface designed to interface with the convex medial femoral condyle. However, a critical biomechanical imperative must be recognized: the curvature of the medial tibial plateau is significantly flatter than that of the medial femoral condyle, creating an inherent osseous incongruence. Without an intermediary load-distributing mechanism, this mismatch would result in focused, high-point contact stresses, rapidly precipitating articular cartilage degradation and early-onset osteoarthritis.
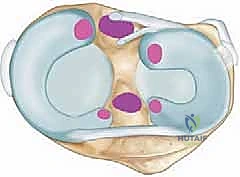
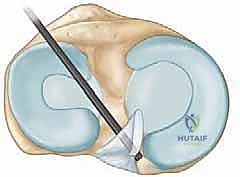
The medial meniscus serves as the primary evolutionary solution to this biomechanical challenge. It is a C-shaped fibrocartilaginous structure situated along the perimeter of the medial tibiofemoral articulation. In cross-section, it is wedge-shaped or triangular, with its thicker, vascularized region located peripherally (the "red-red" zone) and tapering to a thin, avascular inner edge (the "white-white" zone). This geometry significantly enhances joint congruence, converts axial compressive forces into circumferential hoop stresses, and effectively decreases point contact pressures. The medial meniscus is firmly anchored to the tibial plateau at its anterior and posterior horns via the meniscal roots. Furthermore, the deep medial collateral ligament (MCL) attaches firmly to the central body of the medial meniscus (the meniscofemoral and meniscotibial ligaments), providing crucial stability but also rendering it more susceptible to injury during valgus and torsional stress. Crucially for the arthroscopist, the undersurface of the medial meniscus is not adherent to the tibial plateau, allowing for the gentle elevation required to inspect for hidden undersurface tears.
Conversely, the lateral tibiofemoral compartment presents a different anatomical paradigm. The lateral meniscus is shaped more like an 'O' than a 'C' and covers a substantially larger portion—approximately 75%—of the lateral tibial articular surface. This extensive coverage is an absolute necessity due to the unique geometry of the lateral compartment: both the lateral femoral condyle and the lateral tibial plateau present convex surfaces. To achieve appropriate congruence and distribute forces across this convex-on-convex articulation, a larger, highly mobile meniscus is essential.
The mobility of the lateral meniscus is facilitated by its unique capsular attachments. The popliteus tendon courses intra-articularly but extra-synovially, providing stability to the posterior body of the lateral meniscus via three distinct popliteomeniscal fascicles: the anteroinferior, posterosuperior, and posteroinferior fascicles. Anterior and posterior to the popliteus hiatus, a recess of the joint capsule exists that does not insert onto the meniscal periphery. This anatomical arrangement grants the lateral meniscus significantly greater translation during knee flexion compared to its medial counterpart, influencing both its tear patterns and our approach to meniscal repair. Furthermore, originating from the posterior horn of the lateral meniscus are the meniscofemoral ligaments: the ligament of Wrisberg (passing posterior to the PCL) and the ligament of Humphrey (passing anterior to the PCL).
The Patellofemoral Joint
The patellofemoral compartment comprises the patella, the trochlear groove of the femur, the suprapatellar pouch, and the complex dynamic and static stabilizing retinacular structures.
The patella is the largest sesamoid bone in the human body, serving as a biomechanical fulcrum that increases the moment arm of the extensor mechanism. It features distinct medial, lateral, and often "odd" facets that articulate with the trochlea. The patella boasts the thickest articular cartilage in the body—up to 6 millimeters—a direct testament to its role in withstanding compressive forces that can exceed five to seven times body weight during deep flexion activities like stair climbing or squatting. Normal patellofemoral kinematics dictate that the patella begins to engage the superior trochlea at approximately 20 degrees of knee flexion and becomes fully constrained within the bony geometry by 45 degrees. During diagnostic arthroscopy, evaluating this engagement is critical; a lack of medial facet contact at early flexion angles is pathognomonic for patellar maltracking or lateral hyperpressure.
The suprapatellar pouch is a large, potential synovial space that extends proximally beneath the quadriceps tendon. During arthroscopy, fluid distension of this pouch provides an excellent initial viewing chamber. Within this region, the arthroscopist frequently encounters synovial plicae—embryonic remnants of synovial septation. The suprapatellar, medial, and infrapatellar (ligamentum mucosum) plicae are the most common. While often asymptomatic, a thickened, fibrotic medial patellar plica can bowstring across the medial femoral condyle during flexion, causing chondral abrasion and localized pain (plica syndrome). Additionally, the suprapatellar pouch is a notorious repository for intra-articular loose bodies, which can sequester within hidden recesses or "porta" created by these plicae.
The static stabilizers of this joint are the medial and lateral patellofemoral ligaments. The medial patellofemoral ligament (MPFL) is the primary restraint against lateral patellar translation, particularly in early flexion (0 to 30 degrees). Its disruption is the hallmark of acute lateral patellar dislocation. Conversely, a tight lateral retinaculum can tether the patella, leading to excessive lateral tilt and facet overload.
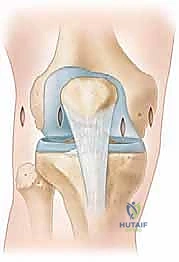
The Intercondylar Notch and Cruciate Ligaments
Situated centrally between the medial and lateral tibiofemoral articulations is the intercondylar notch, a critical non-articular vault housing the central pivot structures of the knee: the anterior and posterior cruciate ligaments. The morphology of the notch—specifically its width and shape (A-shaped vs. U-shaped)—is highly variable. A stenotic notch is a recognized anatomical risk factor for ACL injury and may necessitate a prophylactic notchplasty during ACL reconstruction to prevent graft impingement in extension.
The Anterior Cruciate Ligament (ACL) is the primary restraint to anterior tibial translation. It originates from the posteromedial aspect of the lateral femoral condyle (the lateral wall of the notch), typically described as the 10:30 position on a right knee (or 1:30 on a left knee) when viewed arthroscopically. It courses distally, anteriorly, and medially to insert on the footprint located anterior and between the tibial eminences. The tibial insertion is intimately related to the anterior horn of the lateral meniscus and sits approximately 7 mm anterior to the PCL fibers. The ACL is composed of two functional bundles: the anteromedial (AM) bundle, which is tight in flexion, and the posterolateral (PL) bundle, which is tight in extension and provides critical rotatory stability.
The Posterior Cruciate Ligament (PCL) is the primary restraint to posterior tibial translation and is significantly thicker and stronger than the ACL. It originates from the anterolateral aspect of the medial femoral condyle (the medial wall of the notch), with a broad, crescent-shaped footprint spanning from approximately 12 o’clock to 3:30 on a right knee. The PCL travels distally and posteriorly, crossing behind the ACL, to insert centrally on the posterior tibial sulcus, approximately 10 to 15 mm inferior to the articular joint line. During arthroscopic debridement or PCL reconstruction, extreme vigilance is required; the PCL's posterior insertion is perilously close to the posterior root of the medial meniscus and the extracapsular neurovascular bundle (specifically the popliteal artery).
In the anterior aspect of the joint, bridging the menisci, lies the transverse meniscal ligament. This structure originates from the anterior horn of the medial meniscus and inserts onto the anterior horn of the lateral meniscus. It is a critical landmark; inexperienced arthroscopists or radiologists may misinterpret the junction of this ligament with the menisci as an anterior horn tear on MRI or during direct visualization.
The Synovial Gutters and Posteromedial Compartments
The peripheral recesses of the knee capsule, known as the gutters, demand meticulous inspection during any comprehensive arthroscopy. The medial and lateral gutters are formed by the reflection of the synovium along the medial and lateral aspects of the femoral condyles. These dependent areas are classic hiding spots for chondral fragments, osteochondral loose bodies, and inflammatory debris.
Furthermore, the posteromedial and posterolateral compartments are distinct anatomical zones that are often under-evaluated. The posteromedial compartment houses the posterior horn of the medial meniscus, the meniscocapsular junction, and the ramp lesion area. Accessing these posterior compartments often requires passing the arthroscope through the intercondylar notch (the modified Gillquist maneuver) or establishing dedicated posteromedial or posterolateral accessory portals.
Exhaustive Indications and Contraindications
The decision to proceed with knee arthroscopy must be rooted in a rigorous clinical evaluation, correlating patient history and physical examination with advanced imaging findings. Arthroscopy is not a panacea for all knee pain; it is a targeted intervention for specific mechanical and structural pathologies.
| Category | Specific Pathologies / Considerations | Clinical Rationale |
|---|---|---|
| Primary Indications | Meniscal Tears (Traumatic/Degenerative) | Partial meniscectomy for unrepairable tears; Meniscal repair for peripheral, vascularized tears to restore hoop stresses. |
| Cruciate Ligament Ruptures | ACL/PCL reconstruction to restore translational and rotatory stability, preventing secondary meniscal/chondral damage. | |
| Chondral and Osteochondral Lesions | Debridement, microfracture, osteochondral autograft/allograft transfer (OATS), or matrix-induced autologous chondrocyte implantation (MACI). | |
| Loose Bodies / Synovial Chondromatosis | Extraction to prevent mechanical locking, catching, and third-body wear of the articular cartilage. | |
| Synovial Pathology | Synovectomy for pigmented villonodular synovitis (PVNS), rheumatoid arthritis, or excision of symptomatic, fibrotic plicae. | |
| Septic Arthritis | Emergent arthroscopic irrigation and extensive debridement to reduce bacterial load and preserve articular cartilage. | |
| Absolute Contraindications | Active Overlying Skin Infection | Cellulitis or superficial abscess at the planned portal sites risks introducing pathogens directly into the sterile intra-articular space. |
| Severe Medical Comorbidities | Unstable cardiopulmonary disease or severe coagulopathy that precludes safe administration of regional or general anesthesia. | |
| Relative Contraindications | Advanced Osteoarthritis (Bone-on-Bone) | Arthroscopic debridement for severe, end-stage DJD provides poor long-term outcomes and is generally discouraged unless addressing a specific, acute mechanical block (e.g., a displaced bucket-handle tear). |
| Arthrofibrosis / Severe ROM Deficit | Inability to flex the knee limits intra-articular access and visualization, increasing the risk of iatrogenic cartilage scuffing. |
Pre-Operative Planning, Templating, and Patient Positioning
Surgical excellence begins long before the first incision is made. Meticulous preoperative planning is paramount. Each patient presents a unique anatomical and pathological profile, demanding a highly tailored, patient-specific surgical strategy.
Clinical Evaluation and Imaging Review
As an academic surgeon, I cannot overstate this directive: always personally review the patient's history, physical examination findings, and all imaging studies prior to entering the operating theater. Relying solely on the radiologist's report is a dereliction of surgical duty. Analyze the MRI sequences yourself. Evaluate the meniscal morphology on sagittal and coronal views. Assess the cruciate ligaments on the T2-weighted sagittal sequences. Scrutinize the articular cartilage for focal defects or subchondral edema. This rigorous review is crucial for anticipating intraoperative challenges, confirming the diagnosis, and ensuring all necessary specialized equipment (e.g., meniscal repair devices, specific graft fixation systems) is available and sterile.
Examination Under Anesthesia
On the day of surgery, following the mandatory World Health Organization (WHO) surgical safety checklist and site marking, the patient undergoes induction of anesthesia. Once profound muscle relaxation is achieved, a comprehensive Examination Under Anesthesia (EUA) is strictly required. This is a critical step; awake patients often exhibit involuntary muscle guarding that masks true ligamentous laxity.
We systematically execute the following maneuvers:
* Lachman Test and Pivot Shift: To definitively assess ACL integrity and rotatory instability.
* Posterior Drawer and Sag Sign: To evaluate the PCL and posterior capsular structures.
* Varus and Valgus Stress Tests (at 0 and 30 degrees): To isolate and evaluate the lateral collateral ligament (LCL) and medial collateral ligament (MCL), respectively.
* Dial Test (at 30 and 90 degrees): To assess for posterolateral corner (PLC) injuries.
* Full Range of Motion Assessment: To document baseline flexion and extension, identifying any fixed contractures.
Always compare these findings to the contralateral, unaffected knee to establish the patient's physiologic baseline laxity. The EUA directly dictates the final intraoperative plan.
Patient Positioning and Operating Room Setup
Proper patient positioning is the foundation for optimal visualization and unhindered instrument maneuverability. The patient is positioned supine on the operating table. The operative knee must be positioned distally enough to allow the foot of the bed to be dropped, enabling full, unrestricted knee flexion (minimum 120 degrees) and extension.
The choice of leg support is dictated by surgeon preference, the specific procedure planned, and the patient's body habitus.
The Thigh Holder (Leg Holder): This is the most ubiquitous setup for standard arthroscopy and ACL reconstructions. A pneumatic tourniquet is placed high on the proximal thigh, and a circumferential thigh holder is applied just distal to the tourniquet. This securely fixes the femur, allowing the surgeon to apply valgus or varus stress by manipulating the lower leg, thereby opening the medial or lateral compartments. The contralateral "well-leg" is placed in a padded stirrup or abducted on a leg board to prevent deep vein thrombosis and avoid obstructing the surgeon's working space.

The Lateral Post: For patients with morbid obesity, extreme muscular hypertrophy, or in pediatric cases where a standard thigh holder may cause neurovascular compression or fail to provide adequate fixation, a lateral post is the preferred alternative. The post is rigidly fixed to the bed rail and positioned just proximal to the joint line on the lateral aspect of the thigh. The leg rests flat on the table, and the surgeon uses the post as a fulcrum to apply valgus stress to open the medial compartment. To open the lateral compartment, the leg is brought into a "figure-of-four" position.

Regardless of the chosen positioning apparatus, absolute vigilance regarding soft tissue padding is mandatory. All pressure points, particularly the peroneal nerve at the fibular head and the contralateral heel, must be meticulously padded to prevent devastating perioperative neuropathies or decubitus ulcers.
Step-by-Step Surgical Approach and Fixation Technique
The execution of knee arthroscopy requires a methodical, reproducible approach. Haphazard wandering within the joint leads to missed pathology and iatrogenic injury.
Standard Anterior Portal Placement
Portal placement is arguably the most critical step of the procedure. Poorly placed portals will fight the surgeon for the entire case, limiting reach, creating instrument convergence, and increasing the risk of cartilage scuffing.
The standard approach utilizes two primary anterior portals: the anterolateral (AL) and anteromedial (AM) portals.
* Anterolateral (AL) Portal: This is the primary viewing portal. It is established first. The landmark is the lateral border of the patellar tendon, approximately 1 cm superior to the lateral joint line (the palpable sulcus between the lateral femoral condyle and lateral tibial plateau). A No. 11 scalpel blade is used to make a vertical incision, minimizing the risk of transecting the infrapatellar branches of the saphenous nerve. A blunt trocar is then used to breach the capsule and enter the intercondylar notch, directing the instrument toward the suprapatellar pouch to avoid damaging the articular cartilage.
- Anteromedial (AM) Portal: This is the primary working portal. Its placement should be localized under direct intra-articular visualization using a spinal needle. The ideal location is just medial to the patellar tendon, approximately 1 cm above the medial joint line. The spinal needle trajectory must allow parallel access to the anterior horn of the medial meniscus without being obstructed by the medial femoral condyle. Once the optimal trajectory is confirmed, a vertical incision is made, and instruments are introduced.

Accessory Portals and Posterior Access
Depending on the complexity of the pathology, accessory portals may be required.
* Superomedial or Superolateral Portals: Often used for fluid outflow or for dedicated viewing of patellofemoral tracking dynamics.

* Posteromedial and Posterolateral Portals: Essential for addressing posterior horn meniscal root tears, ramp lesions, or extracting posterior loose bodies. The posteromedial portal is established utilizing a trans-illumination technique. The arthroscope is passed through the intercondylar notch (between the PCL and medial femoral condyle) into the posteromedial compartment. The light source trans-illuminates the skin posterior to the superficial MCL. A spinal needle localizes the portal, ensuring it is posterior to the MCL and anterior to the saphenous nerve and vein.

Systematic Diagnostic Tour
Once access is established, a rigorous, 14-point systematic diagnostic tour must be executed. I train my fellows to perform this sequence identically every single time to ensure no subtle pathology is overlooked.
- Suprapatellar Pouch: Inspect for synovitis, plicae, and loose bodies.
- Patellofemoral Joint: Evaluate the articular cartilage of the patellar facets and the trochlea. Assess patellar tracking dynamically by flexing and extending the knee.

- Medial Gutter: Sweep for loose bodies.
- Medial Compartment: Apply valgus stress and external rotation to open the compartment. Probe the medial meniscus meticulously, checking the anterior horn, body, posterior horn, and roots. Assess the articular cartilage of the medial femoral condyle and tibial plateau.

- Intercondylar Notch: Evaluate the ACL and PCL. Probe the ACL to confirm tension and structural integrity. Assess the synovial coverage and identify the transverse meniscal ligament.
- Lateral Compartment: Apply varus stress and internal rotation (or place the leg in a figure-of-four position). Probe the lateral meniscus, paying special attention to the popliteal hiatus and the posterior horn. Evaluate the lateral articular cartilage.
- Lateral Gutter: Sweep the lateral recess and evaluate the popliteus tendon insertion.
Therapeutic Interventions and Instrumentation
Following the diagnostic sweep, therapeutic intervention commences. For meniscal pathology, the modern paradigm dictates preservation whenever biologically feasible. If a tear is peripheral, longitudinal, and within the vascularized "red-red" zone, meniscal repair (using all-inside suture anchors, inside-out suture techniques, or outside-in techniques) is mandatory.
When meniscectomy is unavoidable (e.g., complex, degenerative, avascular white-zone tears), the principle of economy of resection applies. Using arthroscopic punches, biters, and motorized shavers, only the unstable, mobile fragments are resected. The goal is to contour a stable, smoothly transitioning peripheral rim, preserving as much functional meniscal tissue as possible to maintain joint mechanics. Motorized shavers and radiofrequency ablation wands are utilized for chondroplasty, carefully debriding fibrillated cartilage to stable, vertical borders without violating the subchondral bone plate.
Complications, Incidence Rates, and Salvage Management
While knee arthroscopy is generally considered a safe, minimally invasive procedure, it is not devoid of risks. A profound understanding of potential complications allows for rapid identification and appropriate salvage management.
| Complication | Estimated Incidence | Pathophysiology & Risk Factors | Prevention & Salvage Management |
|---|---|---|---|
| Iatrogenic Cartilage Injury | 1% - 3% | Scuffing of the femoral condyles or tibial plateau during portal entry or instrument manipulation. Common in tight knees or with poor portal placement. | Prevention: Precise portal placement; use blunt trocars for entry; avoid levering instruments against cartilage. Management: Document injury; perform gentle chondroplasty if flaps are created. |
| Neurovascular Injury | < 0.5% | Injury to the saphenous nerve (medial portals), common peroneal nerve (lateral post pressure), or popliteal artery (posterior capsule penetration). | Prevention: Vertical skin incisions; meticulous padding; extreme caution during posterior horn/PCL work. Management: Immediate vascular surgery consultation for suspected arterial injury; nerve injuries often require observation or delayed exploration. |
| Deep Vein Thrombosis (DVT) | 0.5% - 1% | Venous stasis from tourniquet use, positioning, and postoperative immobility. | Prevention: Minimize tourniquet time; early mobilization; mechanical prophylaxis (SCDs). Chemical prophylaxis in high-risk patients. Management: Doppler ultrasound confirmation; therapeutic anticoagulation. |
| Septic Arthritis | 0.1% - 0.4% | Introduction of skin flora (e.g., Staphylococcus aureus) into the joint space. | Prevention: Strict sterile technique; preoperative prophylactic antibiotics; optimal OR airflow. Management: Emergent arthroscopic irrigation |
