

Comprehensive Introduction and Patho-Epidemiology
Welcome, colleagues and fellows. Step in close, let us scrub in and prepare to navigate one of the most challenging yet profoundly rewarding procedures in reconstructive orthopedics: knee arthrodesis. This intervention is rarely an everyday elective case; rather, it is a powerful, durable salvage option, often deployed as a last resort for patients facing severe, limb-threatening challenges. The most common indications include chronically infected total knee arthroplasties (TKAs) with massive bone loss, devastating high-energy periarticular trauma that has obliterated the joint architecture, and radical oncologic resections. Our ultimate surgical objective is to create a stable, painless, and highly functional extremity, allowing for independent ambulation where all other joint-preserving or replacing options have failed or are contraindicated.
Historically, the alternative to a failed, multiply revised, or chronically infected knee has been an above-the-knee amputation (AKA). While AKA remains a viable option in specific scenarios, knee arthrodesis offers a remarkably durable solution that frequently lasts a patient's entire lifetime. From a biomechanical and physiological standpoint, the energy expenditure required for ambulation with a successfully fused knee is significantly less than that required for walking with an AKA prosthesis. This is a crucial, often life-altering consideration, particularly for our elderly patients burdened with cardiopulmonary comorbidities, for whom the increased metabolic demand of an AKA might render them permanently non-ambulatory or wheelchair-bound.
In the younger, high-demand, post-traumatic demographic, a solid knee fusion offers a robust and resilient solution. It enables participation in physically demanding occupations and activities that neither a prosthetic limb nor a highly constrained revision TKA could reliably accommodate without the risk of catastrophic failure. The natural history of severe traumatic and infectious processes around the knee is exceptionally dire without definitive intervention; patients are typically left with an unstable, flail limb, chronic pain, and an inability to bear weight. By executing a meticulous arthrodesis, we intervene to halt this downward spiral, providing axial stability, eradicating infection, and restoring functional independence.
Detailed Surgical Anatomy and Biomechanics
Our standard approach for knee arthrodesis is an extensile anterior midline incision, often utilizing previous surgical scars to minimize skin bridge necrosis. Understanding the intricate and often distorted anatomy is paramount, especially given that the soft tissue envelope and osseous structures are frequently compromised from multiple previous surgeries, chronic infection, or massive trauma.
Osteology and Extensor Mechanism Integrity
The anterior knee often presents a severely compromised soft tissue envelope. In cases of multiply revised or infected TKA, the extensor mechanism—comprising the quadriceps tendon, patella, and patellar tendon—may be attenuated, chronically retracted, or entirely absent due to prior radical débridement. This deficiency can lead to a significant anterior soft tissue defect, leaving the underlying bone subcutaneous and lacking robust, well-vascularized muscle coverage. Consequently, wound healing is a primary concern, and the surgeon must meticulously preserve any remaining vascular supply to the anterior skin flaps. The distal femur and proximal tibia are our primary osteological focus; our goal is to achieve broad, healthy, bleeding cancellous bone contact between these two surfaces to optimize the biological environment for fusion.
If an intramedullary (IM) nailing technique is selected, understanding the alignment and entry points is critical. For long, spanning IM nails, the piriformis fossa or greater trochanter serves as the critical entry point in the ipsilateral femur, while the tibial entry point must be carefully calculated to ensure proper mechanical alignment. The surgeon must account for the natural anatomical valgus of the femur (typically 5 to 7 degrees) and the mechanical axis. A perfectly straight IM nail driven through both the femur and tibia will result in 0 degrees of anatomic valgus, which is mechanically acceptable but requires careful preoperative calculation to avoid medializing the mechanical axis too severely.
Neurovascular Topography of the Popliteal Fossa
The most critical anatomical region requiring absolute vigilance is directly posterior to the knee joint: the popliteal fossa. Here lie the vital neurovascular structures that dictate the survival and function of the distal extremity. The popliteal artery is the deepest structure, lying directly against the posterior capsule of the joint, making it exceptionally vulnerable during capsular release or bone resection. Superficial to the artery is the popliteal vein, often the most prominent vascular structure encountered if posterior dissection is inadvertently deep.
Furthermore, the sciatic nerve bifurcates superior to the popliteal fossa into the tibial nerve and the common peroneal nerve. The tibial nerve runs medially and superficially to the popliteal vessels, while the common peroneal nerve courses laterally, superficial to the lateral head of the gastrocnemius, before wrapping around the fibular neck. This lateral nerve is particularly vulnerable to traction injury, direct compression from retractors, or transection during lateral capsular release or fibular head resection.
SURGICAL WARNING: Popliteal Neurovascular Bundle
Extreme caution is required when elevating the posterior capsule off the distal femur and proximal tibia. This maneuver brings the surgeon into direct proximity with the popliteal artery, vein, and tibial nerve. In cases of significant bone loss, chronic infection, or severe scarring, these structures can be densely adherent or anatomically displaced. Always work meticulously, maintaining clear visualization, and utilize blunt dissection or periosteal elevators to stay strictly subperiosteal, avoiding catastrophic vascular or nerve injury.

Exhaustive Indications and Contraindications
While highly effective as a salvage procedure, knee fusion is not universally applicable and requires careful patient selection. Fusing the knee inevitably eliminates the flexion-extension arc, shifting compensatory motion and mechanical stress to the adjacent joints—specifically the ipsilateral hip, the ipsilateral ankle, and the lumbar spine.
Patient Selection Criteria
The ideal candidate for a knee arthrodesis is a patient with a unilateral, unsalvageable knee joint who possesses good compensatory mobility in their adjacent joints and sufficient cardiovascular reserve to participate in postoperative rehabilitation. Patients with a highly virulent, multi-drug resistant periprosthetic joint infection (PJI) that has failed two-stage exchange arthroplasty are classic candidates. Similarly, young patients with massive periarticular bone loss from trauma or tumor resection, for whom a mega-prosthesis would likely fail prematurely, are excellent candidates for the durability of a fusion.
Conversely, significant pre-existing arthritis or restricted range of motion in the ipsilateral hip or ankle are relative contraindications. Over time, the altered gait mechanics of a fused knee will invariably exacerbate these conditions. Furthermore, severe lumbar spine pathology is a major concern; the loss of knee flexion requires the patient to utilize compensatory pelvic hike and spinal circumduction to clear the foot during the swing phase of gait. This increased spinal motion can rapidly accelerate degenerative disc disease and exacerbate chronic back pain.
| Category | Specific Conditions | Clinical Rationale |
|---|---|---|
| Primary Indications | Failed infected TKA (recalcitrant PJI) | Eradicates infection while providing a stable, weight-bearing limb. |
| Massive periarticular trauma | Stabilizes flail limbs where articular reconstruction is impossible. | |
| Post-tumor resection | Provides durable reconstruction when mega-prostheses are contraindicated. | |
| Paralytic limb with instability | Restores axial stability for weight-bearing in polio or severe neuropathy. | |
| Relative Contraindications | Ipsilateral severe hip arthritis | Fusion shifts stress, rapidly accelerating hip degeneration and pain. |
| Severe lumbar spine pathology | Compensatory circumduction gait exacerbates spinal stenosis and disc disease. | |
| Contralateral limb amputation | Bilateral stiff limbs severely limit independent mobility and transfers. | |
| Absolute Contraindications | Severe peripheral vascular disease | Inadequate perfusion precludes bone healing and soft tissue recovery. |
| Active, untreated systemic sepsis | Source control must be achieved prior to definitive reconstructive efforts. | |
| Non-ambulatory patient baseline | If the patient was not walking prior, fusion exposes them to surgical risk without functional gain. |
Pre-Operative Planning, Templating, and Patient Positioning
Meticulous preoperative planning is the absolute cornerstone of a successful knee arthrodesis. It allows the surgical team to anticipate anatomical challenges, select the most appropriate fixation technique, and prepare for potential intraoperative complications, particularly regarding bone loss and soft tissue coverage.
Clinical and Systemic Evaluation
The evaluation begins with an exhaustive review of the patient's surgical and medical history. The surgeon must document all prior interventions around the knee, including the exact nature of previous implants, the presence of retained cement or hardware, and the history of any local or free flap surgeries. Comorbidities such as peripheral vascular disease, poorly controlled diabetes, chronic malnutrition, and smoking status must be critically assessed and optimized, as these factors profoundly compromise osteogenesis and soft tissue healing.
A rigorous physical examination is mandatory. The integrity and range of motion of the ipsilateral hip and ankle must be documented. Any existing equinus contracture of the ankle will severely impede ambulation post-fusion and should be addressed concomitantly with an Achilles tendon lengthening or a gastrocnemius recession. Vascular assessment is non-negotiable; if dorsalis pedis and posterior tibialis pulses are diminished or absent, a formal vascular evaluation with Ankle-Brachial Indices (ABI) or CT angiography is required before proceeding. Finally, the soft tissue envelope must be inspected for adherent scars, previous skin grafts, and overall pliability, which will dictate the surgical approach and closure strategy.
Advanced Imaging and Defect Assessment
The most critical imaging studies are high-quality, long-standing anteroposterior (AP) erect lower limb radiographs and long lateral view radiographs. These films provide the foundational data for templating.

Limb-Length Discrepancy (LLD) must be accurately assessed to predict the final discrepancy after bone resection and fusion. To ensure radiographic accuracy, the patient's pelvis must be leveled using calibrated blocks under the short leg before the radiograph is taken. This prevents the patient from compensating with an equinus posture of the short limb or knee flexion of the long limb, which would skew the measurements. The radiograph should ideally be obtained from 10 feet away using a 51-inch cassette to minimize magnification errors.


Alignment and bone defect size are also evaluated on these films. The surgeon must calculate the exact size of the segmental defect that will remain after débridement of infected or devitalized bone. This measurement dictates the surgical strategy. Magnetic Resonance Imaging (MRI) can occasionally be helpful for evaluating the proximal extent of intramedullary osteomyelitis, but it must be interpreted with extreme caution, as reactive bone marrow edema can easily mimic active infection, potentially leading to unnecessarily aggressive bone resection.
Templating and Hardware Selection
Based on the size of the anticipated bone defect and the patient's physiological status, a definitive fixation strategy is selected. Acute shortening is often preferred for small defects, but defects exceeding 5 to 6 cm, if acutely compressed, can lead to severe vascular kinking and subsequent limb ischemia.
| Size of Segmental Bone Gap | Recommended Treatment Strategy |
|---|---|
| < 3 cm | Acute shortening and compression with Intramedullary (IM) Nail or Dual Plating. |
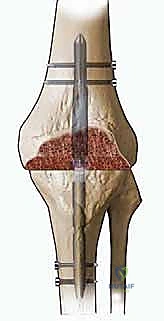
| 3 to 6 cm | Acute shortening (with careful vascular monitoring) OR Modular IM Nail with structural allograft/autograft. |
| > 6 cm | Bone transport (Ilizarov/Taylor Spatial Frame) OR massive structural allograft with long IM nail OR custom mega-prosthesis (if infection is completely eradicated). |
Step-by-Step Surgical Approach and Fixation Technique
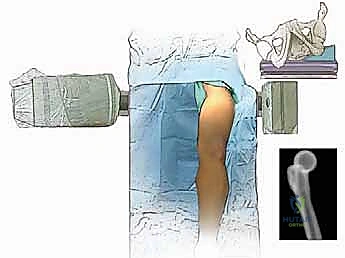
The patient is typically positioned supine on a radiolucent table to allow for unhindered fluoroscopic imaging from the hip to the ankle. A sterile tourniquet may be applied high on the thigh, though its use is often precluded by the need for proximal extension of the incision or the presence of vascular disease.
Soft Tissue Dissection and Joint Exposure
The surgical approach is generally an anterior midline incision, incorporating and excising prior surgical scars whenever possible to prevent the creation of narrow, ischemic skin bridges. Full-thickness fasciocutaneous flaps are elevated medially and laterally to expose the extensor mechanism. In the setting of a failed TKA, the joint capsule is incised, and a meticulous, radical synovectomy and débridement are performed. All retained foreign material, including polyethylene debris, polymethylmethacrylate (PMMA) cement, and the metallic implants themselves, must be completely extracted.

The removal of well-fixed cement mantles from the femoral and tibial canals is often the most time-consuming and hazardous portion of the procedure, requiring specialized extraction tools, flexible osteotomes, and occasionally, cortical windows. Once the hardware is removed, the bone ends are aggressively débrided back to healthy, bleeding cancellous bone. The posterior capsule is carefully elevated off the distal femur and proximal tibia using blunt periosteal elevators, strictly adhering to the bone to protect the popliteal neurovascular bundle.
Bone Preparation and Defect Management
To maximize the surface area for osseous integration, the bone ends are prepared with flat, parallel cuts using an oscillating saw. The femoral cut is typically made perpendicular to the anatomical axis in the coronal plane, and the tibial cut is made perpendicular to the mechanical axis of the tibia. Some surgeons prefer to fashion the cuts to allow for 5 to 7 degrees of valgus and 5 to 10 degrees of flexion to facilitate a more natural swing phase during gait, though a perfectly straight, 0-degree fusion is mechanically sound and often easier to achieve with a long IM nail.

If a massive bone defect is present, the surgeon must execute the pre-planned defect management strategy. If acute shortening is utilized, the bone ends are brought into direct apposition. The distal pulses must be immediately checked; if vascular compromise is suspected due to vessel kinking, the shortening must be reversed, and an alternative strategy, such as bone transport with an external fixator or the interposition of a structural graft, must be employed.

Intramedullary Nailing and Alternative Fixation Methods
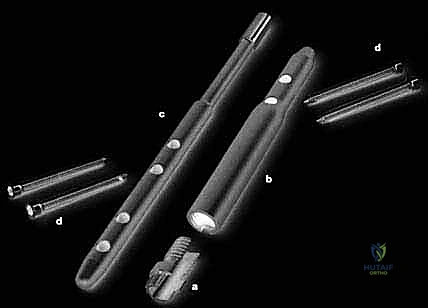
Intramedullary nailing is widely considered the gold standard for knee arthrodesis due to its superior biomechanical stability, load-sharing properties, and high fusion rates. A long, spanning arthrodesis nail is introduced antegrade through the piriformis fossa or greater trochanter of the femur. The femoral and tibial canals are sequentially reamed to accommodate the largest possible nail diameter, ensuring a tight isthmic fit.

The nail is driven across the prepared docking site into the tibia. Compression across the arthrodesis site is absolutely critical for primary bone healing. This can be achieved through internal compression mechanisms built into modern modular nails or by utilizing external compression devices prior to final distal interlocking.


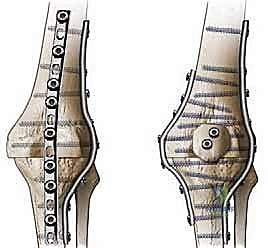
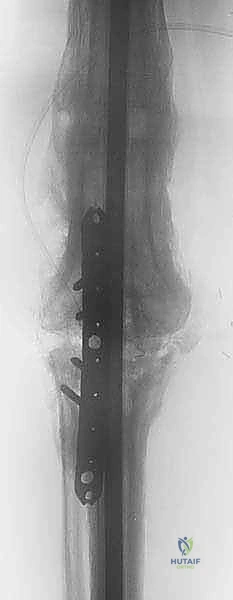
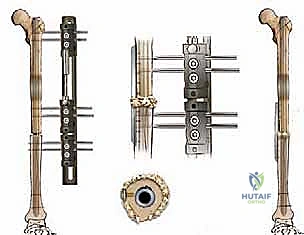
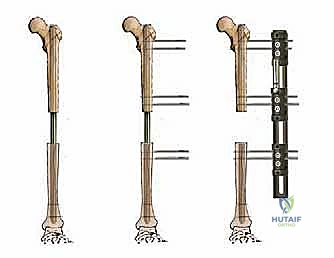
In cases where IM nailing is precluded—such as in the presence of an ipsilateral total hip arthroplasty, total ankle arthroplasty, or severe canal deformity—dual orthogonal plating (typically an anterior and a medial/lateral plate) or circular external fixation (Ilizarov method) are viable, albeit technically demanding, alternatives. External fixation is particularly advantageous in the setting of active, poorly controlled infection, as it avoids placing massive permanent hardware into a contaminated bed and allows for simultaneous bone transport to address large defects.
Complications, Incidence Rates, and Salvage Management
Despite meticulous technique, knee arthrodesis is fraught with potential complications, reflecting the severely compromised baseline status of these patients. The surgeon must be prepared to identify and manage these issues promptly to prevent catastrophic failure or eventual amputation.
Intraoperative and Early Postoperative Complications
Intraoperative complications include iatrogenic fractures during hardware removal or canal reaming, and catastrophic vascular injury during posterior dissection or acute limb shortening. Postoperatively, the most pressing concern is wound necrosis and deep infection. The anterior soft tissue envelope is notoriously tenuous; marginal necrosis can rapidly progress to deep hardware exposure. Prophylactic plastic surgery consultation for local rotational flaps (e.g., medial gastrocnemius flap) or free tissue transfer should be considered if closure under tension is anticipated.
Deep vein thrombosis (DVT) and pulmonary embolism (PE) are significant risks given the extensive medullary reaming and prolonged immobilization. Aggressive chemical and mechanical prophylaxis is mandatory unless strictly contraindicated.
Late Complications and Nonunion
Nonunion is the most common late complication, with reported rates ranging from 10% to 20% depending on the fixation method and patient comorbidities. Aseptic nonunion typically presents with persistent pain and hardware failure (e.g., broken interlocking screws or nail breakage). Treatment usually requires revision fixation, enhancement of stability, and the addition of autologous bone graft or orthobiologics.


Septic nonunion or recurrence of the original PJI is a devastating outcome. It necessitates complete hardware removal, aggressive radical débridement, placement of antibiotic spacers, and eventual conversion to an external fixator or, frequently, progression to an above-knee amputation if the host is exhausted.

| Complication | Estimated Incidence | Prevention and Salvage Management |
|---|---|---|
| Nonunion | 10% - 20% | Maximize bone contact, achieve rigid compression. Salvage with revision fixation and bone grafting. |
| Recurrent Infection | 5% - 15% | Thorough two-stage approach for PJI. Salvage requires hardware removal, Ex-Fix, or AKA. |
| Hardware Failure | 5% - 10% | Use largest possible IM nail; ensure solid docking. Salvage with larger nail or dual plating. |
| Vascular Injury / Ischemia | < 2% | Avoid >5cm acute shortening; meticulous posterior dissection. Salvage with immediate vascular repair. |
| Periprosthetic Fracture | 2% - 5% | Careful reaming, avoid stress risers at nail tips. Salvage with spanning plates or longer nails. |
Phased Post-Operative Rehabilitation Protocols
The rehabilitation following a knee arthrodesis requires a delicate balance between protecting the osseous docking site to ensure fusion and mobilizing the patient to prevent systemic complications and adjacent joint stiffness.
Immediate Postoperative Phase and Weight-Bearing
In the immediate postoperative period, the limb is typically elevated to minimize edema, and closed suction drains are monitored and removed once output decreases. The weight-bearing status is entirely dictated by the stability of the intraoperative fixation and the quality of the host bone. If a robust, large-diameter IM nail achieves excellent cortical purchase and solid compression across the arthrodesis site, patients may be allowed to bear weight as tolerated (WBAT) immediately with a walker or crutches. This axial loading can actually promote micromotion and stimulate secondary bone healing.
Conversely, if fixation is achieved via dual plating in osteoporotic bone, or if a structural allograft is utilized without an IM nail, weight-bearing is strictly restricted (non-weight bearing or toe-touch weight bearing) for 6 to 12 weeks until radiographic evidence of bridging callus is observed. Physical therapy focuses heavily on upper extremity strengthening, core stability, and maintaining full range of motion in the ipsilateral hip and ankle.
Long-Term Adaptation and Functional Outcomes
As the fusion solidifies, the focus shifts to gait training. A fused knee fundamentally alters the biomechanics of walking. Because the knee cannot flex during the swing phase, the limb effectively becomes "longer" during this phase, requiring the patient to utilize compensatory mechanisms to clear the foot from the ground. Patients will naturally develop a circumduction gait (swinging the leg outward) or a vaulting gait (rising on the toes of the contralateral foot).
To optimize gait and minimize energy expenditure, addressing any residual limb-length discrepancy is critical. Most arthrodesis procedures result in 2 to 4 cm of shortening. This mild shortening is actually functionally advantageous, as it assists with foot clearance during the swing phase of the stiff limb. However, discrepancies greater than 1.5 to 2 cm typically require a permanent shoe lift on the operative side to level the pelvis and prevent progressive lower back pain and contralateral hip strain. With proper physical therapy and orthotic management, patients can achieve a highly functional, independent, and pain-free ambulatory status.
Summary of Landmark Literature and Clinical Guidelines
The orthopedic literature heavily supports intramedullary nailing as the premier technique for knee arthrodesis, particularly following failed TKA.
Evidence-Based Outcomes and Future Directions
Landmark studies comparing fixation methods consistently demonstrate that IM nailing yields the highest fusion rates (frequently exceeding 90%) and the lowest rates of hardware failure compared to external fixation or dual plating. External fixation, while invaluable for active infection and bone transport, is associated with high rates of pin tract infections, patient non-compliance, and inferior biomechanical stability against bending forces.
Furthermore, physiological studies analyzing energy expenditure (such as those by Waters et al.) have conclusively proven that walking with a successful knee arthrodesis requires approximately 20% to 30% less oxygen consumption and metabolic energy compared to walking with an above-knee amputation prosthesis. This data is paramount when counseling elderly or medically frail patients, as it underscores arthrodesis not merely as a limb-sparing procedure, but as a life-enhancing, function-preserving masterclass in reconstructive surgery. Future advancements in modular nail designs, bioactive coatings to prevent bacterial colonization, and customized 3D-printed structural augments will continue to refine our ability to salvage these extraordinarily complex limbs.
Detailed Chapters & Topics
Dive deeper into specialized chapters regarding knee-arthrodesis