Knee Osteochondral Lesions: An Intraoperative Masterclass in OCD & AVN Management

Key Takeaway
Welcome to the OR, fellows. Today, we're tackling knee osteochondral lesions, specifically Osteochondritis Dissecans (OCD) and Avascular Necrosis (AVN). This masterclass will guide you through precise surgical anatomy, meticulous preoperative planning, and granular intraoperative execution, from initial arthroscopy to advanced fixation and drilling techniques. We'll cover critical pearls, pitfalls, and comprehensive postoperative management to ensure optimal patient outcomes for these challenging conditions.
Comprehensive Introduction and Patho-Epidemiology
Welcome, colleagues and fellows, to the operating theater and this definitive masterclass on a fascinating, ubiquitous, and often formidable area of knee pathology: osteochondral lesions. Specifically, we will be undertaking a rigorous examination of Osteochondritis Dissecans (OCD) and Avascular Necrosis (AVN) of the knee. These conditions, while distinctly divergent in their etiology, demographic presentation, and natural history, share a devastating common endpoint. If left unaddressed or mismanaged, both precipitate catastrophic damage to the articular cartilage and the critical underlying subchondral bone architecture. This structural failure inevitably leads to intractable pain, severe mechanical dysfunction, and accelerated, irreversible degenerative joint disease. Our objective in this comprehensive chapter is to dissect the nuances of advanced diagnosis, elaborate on meticulous surgical planning, and define the precise intraoperative execution required to manage these complex cases successfully.
To establish a foundation for advanced surgical decision-making, we must first rigorously clarify the definitions and pathophysiological distinctions of these entities. The nomenclature in osteochondral pathology is frequently applied with insufficient precision, leading to diagnostic ambiguity and suboptimal treatment algorithms. Spontaneous Osteonecrosis of the Knee (SONK), now more accurately termed subchondral insufficiency fracture of the knee (SIFK), typically involves a focal stress fracture of the subchondral bone plate, frequently culminating in secondary mechanical collapse. It is highly correlated with altered joint biomechanics, often observed in patients following meniscectomy or those suffering from meniscal root tears leading to extrusion. Clinically, SONK is a disease of the older demographic (typically over 55 years of age), presents with acute unilateral pain, and almost exclusively involves a single condyle—predominantly the weight-bearing surface of the medial femoral condyle.
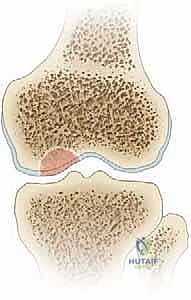
In stark contrast, Osteochondritis Dissecans (OCD) is characterized by a focal segment of subchondral bone undergoing avascular changes, leading to structural destabilization. Crucially, this "wafer" of avascular bone, intimately bound to its overlying articular cartilage, may progressively separate from the underlying healthy osseous bed. The underlying host bed in OCD remains biologically normal and highly vascularized, though it becomes physically separated from the lesion by a distinct, fibrous, and sclerotic rim that inhibits spontaneous healing. Avascular Necrosis (AVN), or secondary osteonecrosis, diverges further by involving a significantly larger, typically wedge-shaped segment of bone that has suffered a catastrophic loss of its vascular supply, often secondary to systemic factors (e.g., corticosteroid use, alcohol abuse, coagulopathies). If this profound ischemic necrosis propagates to the subchondral plate, it precipitates macroscopic subchondral fracture and widespread articular surface collapse. Unlike OCD, the avascular osteochondral surface in AVN frequently fragments and separates from an inherently avascular and biologically compromised bed. Furthermore, AVN is not confined to the epiphysis; it routinely extends into the metaphysis and diaphysis, and presents bilaterally and multifocally in over 80% of cases.


Finally, we must distinguish between pure chondral lesions and true osteochondral lesions. Chondral lesions are strictly confined to the articular cartilage layer, failing to penetrate the tidemark or the subchondral bone plate. Consequently, the damage is isolated to the chondrocytes and their extracellular matrix, eliciting virtually no inflammatory or reparative healing response from the underlying marrow elements due to the avascular nature of cartilage. Conversely, osteochondral lesions, by definition, violate the subchondral bone. Because they penetrate into the vascularized marrow space, they trigger a robust inflammatory healing cascade. It is this very access to the marrow elements that we attempt to exploit surgically in marrow stimulation techniques, though the resulting repair tissue is typically biomechanically inferior fibrocartilage rather than native hyaline cartilage.
Detailed Surgical Anatomy and Biomechanics
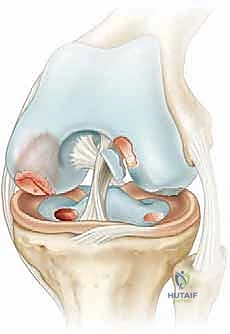
Mastery of the precise topographical anatomy and vascular architecture of the knee, with particular emphasis on the distal femoral condyles, is an absolute prerequisite for the successful operative management of both OCD and AVN. The distal femur is characterized by its complex bi-condylar geometry, designed to accommodate the intricate rolling and gliding kinematics of the tibiofemoral articulation. The articular cartilage thickness varies significantly across the condyles, generally being thicker on the weight-bearing surfaces and the patellofemoral groove. The subchondral bone plate, immediately deep to the calcified cartilage layer, serves as a critical shock absorber and structural foundation. Disruptions in this plate, whether from the localized ischemia of OCD or the massive infarction of AVN, fundamentally alter load transmission, leading to pathological stress concentrations on the overlying cartilage.
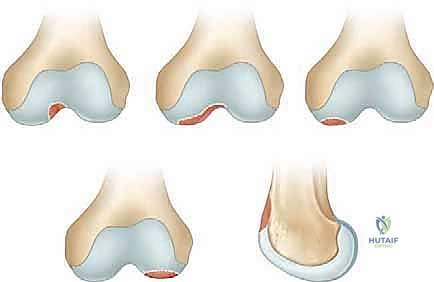
The anatomical distribution of Osteochondritis Dissecans lesions within the knee is remarkably specific and dictates our surgical approach. The Medial Femoral Condyle (MFC) is the overwhelmingly predominant site, accounting for 80% to 85% of all documented cases. The "classic" OCD lesion localizes to the lateral aspect of the MFC, adjacent to the intercondylar notch, representing approximately 70% of MFC presentations. This area is subjected to unique shear forces, particularly from the tibial spine during internal tibial rotation. An "extended classical" variant accounts for 5%, involving a broader swath of the condyle. "Inferocentral" lesions, encompassing 10% of MFC cases, are situated more directly on the central weight-bearing axis and carry a higher risk of rapid progression to osteoarthritis if untreated. The Lateral Femoral Condyle (LFC) harbors 10% to 15% of lesions, almost exclusively in the inferocentral, weight-bearing region. Lesions of the trochlea (<1%) and the patella (5% to 10%, typically inferomedial) are significantly less common but present unique challenges regarding fixation trajectories and patellofemoral kinematics.
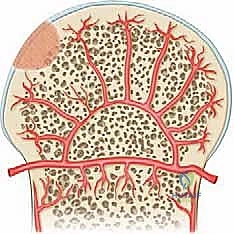
The vascular anatomy of the distal femoral epiphysis is paramount to understanding the etiology of OCD. The epiphyseal artery supplies the epiphysis and secondary centers of ossification via a delicate network of small end-arteries. The prevailing pathophysiological theory posits that repetitive microtrauma—often associated with rigorous athletic activity in a growing child—or a discrete traumatic event can compromise these vulnerable end-arteries. This localized vascular disruption results in transient ischemia to a highly specific, circumscribed segment of subchondral bone, initiating the OCD cascade. In contrast, the anatomy of Avascular Necrosis (AVN) is characterized by a much broader territory of infarction. AVN involves a massive wedge-shaped segment of subchondral bone, frequently with profound extension deep into the epiphysis and proximally into the metaphysis or even the diaphysis. It can affect the femur, the tibia, or both simultaneously.
When executing surgical interventions around the condyles, the orthopedic surgeon must maintain an acute awareness of critical regional neurovascular and tendinous structures. On the medial aspect, the saphenous nerve and the great saphenous vein course superficially; medial portals and arthrotomy incisions must be meticulously planned to avoid iatrogenic injury to these structures, as well as the deep medial collateral ligament (MCL) and the pes anserinus insertion. Laterally, while the common peroneal nerve is generally protected posterior to the fibular head, extreme caution is mandated during extensive lateral approaches or when utilizing deep, posterolateral drill trajectories, particularly if the pathology extends toward the proximal tibia. Posteriorly, the popliteal artery, popliteal vein, and tibial nerve lie in close proximity to the posterior capsule. Transarticular drilling of posterior condylar lesions, or the establishment of posteromedial/posterolateral arthroscopic portals, requires rigorous depth control, precise angulation, and often the use of a posterior safety stop to preclude catastrophic vascular injury.
Exhaustive Indications and Contraindications
The decision-making algorithm for surgical intervention in osteochondral lesions of the knee is complex, heavily reliant on the patient's skeletal maturity, the specific pathology (OCD vs. AVN vs. SONK), the stability of the lesion, and the presence of clinical symptoms. Skeletal maturity is arguably the most critical inflection point in the management of OCD. Juvenile Osteochondritis Dissecans (JOCD), occurring in patients with open physes, possesses a robust intrinsic healing potential. Consequently, asymptomatic or stable JOCD lesions are initially managed with a strict regimen of non-operative therapy, including activity modification, protected weight-bearing, and immobilization. Conversely, Adult Osteochondritis Dissecans (AOCD), defined by closed physes, exhibits a dismal rate of spontaneous healing. Therefore, the threshold for surgical intervention in AOCD is significantly lower, and non-operative management is rarely successful for anything beyond incidental, asymptomatic, and radiographically stable findings.
Surgical intervention is definitively indicated when non-operative management of a stable JOCD lesion fails after a rigorous 3 to 6-month trial, evidenced by persistent pain, mechanical symptoms, or lack of radiographic progression toward healing. Furthermore, immediate surgical management is mandated for any lesion—regardless of skeletal maturity—that demonstrates signs of instability. Clinical indicators of instability include mechanical catching, locking, or recurrent effusions. Radiographic and MRI hallmarks of instability include a high T2 signal line (fluid) interposing between the lesion and the host bone, multiple cysts at the interface, a breach in the overlying articular cartilage, or frank displacement of the osteochondral fragment. In the setting of AVN, indications for surgery depend heavily on the stage of the disease. Early, pre-collapse AVN (Ficat Stage I/II) may be amenable to core decompression to reduce intraosseous pressure and stimulate revascularization. Once subchondral collapse has occurred (Ficat Stage III/IV), joint preservation techniques become significantly more complex, often necessitating massive osteochondral allografts or, ultimately, arthroplasty.

Contraindications to joint-preserving surgical intervention must be carefully respected to avoid catastrophic failure. Absolute contraindications include active local or systemic infection, severe uncorrectable coagulopathy, and a medically unstable patient unable to tolerate anesthesia. Relative contraindications are highly context-dependent. In the setting of advanced, generalized osteoarthritis with widespread tricompartmental cartilage loss, focal cartilage restoration procedures (like OATS or MACI) are destined to fail and are contraindicated; such patients are better served by arthroplasty. Similarly, uncorrected mechanical malalignment (e.g., severe varus or valgus deformity) that places excessive sheer and compressive loads on the planned repair site is a strong relative contraindication. Any planned cartilage restoration must be preceded by or performed concurrently with a corrective osteotomy (e.g., High Tibial Osteotomy or Distal Femoral Osteotomy) to normalize the mechanical axis.
Table: Indications and Contraindications for Operative Management
| Parameter | Indications for Joint Preservation Surgery | Contraindications for Joint Preservation Surgery |
|---|---|---|
| Patient Factors | Symptomatic AOCD; Failed conservative JOCD | Advanced chronological/physiological age |
| Lesion Status | Unstable, detached, or displaced fragment | Active joint infection or systemic sepsis |
| Symptoms | Mechanical locking, catching, recurrent effusions | Asymptomatic, stable JOCD (initial management) |
| Joint Health | Focal defect with otherwise healthy surrounding cartilage | Widespread, advanced tricompartmental osteoarthritis |
| Biomechanics | Normal mechanical axis, or concurrently correctable | Uncorrected, severe mechanical malalignment |
| AVN Specifics | Pre-collapse (core decompression); Focal post-collapse | Massive, diffuse, multi-compartmental collapse |
Pre-Operative Planning, Templating, and Patient Positioning
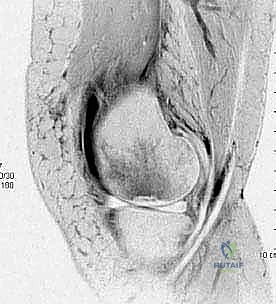
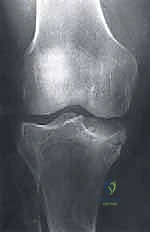
Exhaustive preoperative planning is the absolute cornerstone of a successful intraoperative execution and optimal postoperative outcome. This process begins with a meticulous radiographic evaluation. Standard plain radiographs must include a weight-bearing Anteroposterior (AP) view to assess overall alignment and joint space narrowing, and a true Lateral view to determine the anterior-posterior precise location of the lesion on the condyle. However, the most critical plain radiograph for OCD is the Tunnel View (Intercondylar Notch View), typically taken at 45 degrees of flexion. Because the classic OCD lesion is located on the posterolateral aspect of the medial femoral condyle, it frequently remains hidden behind the tibial plateau on a standard extension AP radiograph. The tunnel view profiles the posterior condyles, explicitly revealing the classic lesion. A Sunrise (patellar) view is essential to rule out patellofemoral involvement. Furthermore, given the high incidence of bilaterality (15-30% in OCD, >80% in AVN), obtaining comparison views of the contralateral knee is mandatory.



Advanced imaging, specifically Magnetic Resonance Imaging (MRI), is indispensable for staging the lesion, assessing stability, and guiding the surgical approach. A comprehensive MRI protocol should include T1-weighted, T2-weighted, and proton density fat-suppressed sequences in all three orthogonal planes. MRI allows for the precise measurement of the lesion's dimensions (critical for graft templating), evaluation of the overlying articular cartilage integrity, and assessment of the subchondral bone viability. The hallmark of an unstable lesion on MRI is a rim of high T2 signal intensity completely surrounding the osteochondral fragment, indicating synovial fluid interposition and failure of osseous integration. Additionally, the presence of subchondral cysts deep to the lesion suggests chronic instability and requires specific intraoperative management, typically involving curettage and bone grafting.



Once the lesion is fully characterized, surgical templating is performed. For salvageable lesions requiring internal fixation, the trajectory of the screws or bioabsorbable darts must be planned to ensure they are perpendicular to the lesion interface, maximizing compression while avoiding penetration into the intercondylar notch or posterior neurovascular structures. If the fragment is deemed unsalvageable, the defect size dictates the cartilage restoration strategy. Small defects (<2-3 cm²) may be amenable to marrow stimulation (microfracture) or Osteochondral Autograft Transfer (OATS). Larger defects (>3 cm²) necessitate advanced techniques such as Osteochondral Allograft (OCA) transplantation or Matrix-Induced Autologous Chondrocyte Implantation (MACI). Patient positioning is typically supine on a standard operating table. A well-padded high-thigh tourniquet is applied but inflated only if visualization becomes compromised. The leg is placed in a surgical leg holder or positioned over a post to allow for full, unencumbered flexion (up to 120 degrees) and extension, which is vital for accessing different regions of the femoral condyles arthroscopically. Fluoroscopy should be positioned on the contralateral side, draped sterilely, and readily available to verify drill trajectories and hardware placement during fixation.
Step-by-Step Surgical Approach and Fixation Technique
The surgical intervention invariably commences with a comprehensive diagnostic arthroscopy. Standard anterolateral and anteromedial portals are established, and a systematic evaluation of all joint compartments is performed to identify any concomitant pathology, such as meniscal tears or loose bodies. The osteochondral lesion is then meticulously visualized and probed. The arthroscopic probe is the surgeon's most vital diagnostic tool at this stage; it is used to assess the integrity of the overlying cartilage, palpate for softening (ballottement), and determine the macroscopic stability of the fragment. Based on these intraoperative findings, the lesion is graded, often utilizing the International Cartilage Repair Society (ICRS) classification system. An intact, stable lesion with intact cartilage (ICRS Grade I or II) in a symptomatic patient requires a different approach than a partially detached (Grade III) or completely detached (Grade IV) lesion.
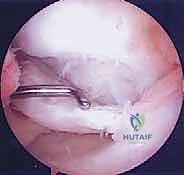

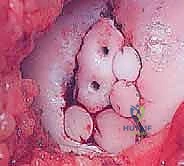
For intact, stable lesions that have failed conservative management (particularly in JOCD), the goal is to stimulate revascularization and healing without violating the articular surface. This is achieved through extra-articular (retroarticular) or transarticular drilling. Retroarticular drilling is technically demanding, requiring fluoroscopic guidance and an ACL tibial guide to direct a K-wire from the extra-articular metaphyseal cortex, through the epiphysis, and into the sclerotic base of the lesion, stopping precisely short of the subchondral plate. This preserves the pristine articular cartilage. Transarticular drilling is more straightforward, involving direct drilling through the articular cartilage into the subchondral bone using a 0.045-inch or 0.062-inch K-wire. Multiple perforations are created to breach the sclerotic rim and allow marrow elements (mesenchymal stem cells, growth factors) to access the avascular fragment.


When dealing with a salvageable but unstable or partially detached fragment, primary internal fixation is the gold standard. The surgical bed must first be meticulously prepared. The fragment is hinged open like a trapdoor (if partially attached) or temporarily removed. The underlying sclerotic host bed is aggressively debrided with a curette or a motorized burr until healthy, punctate bleeding bone is encountered. If a significant cystic void exists beneath the fragment, it must be packed with autologous cancellous bone graft (often harvested from the proximal tibia or distal femur) to provide structural support and osteoinductive stimulus. The fragment is then anatomically reduced. Fixation is achieved using variable-pitch headless compression screws, bioabsorbable compression darts, or even autologous osteochondral pegs. The hardware must be countersunk 1-2 mm below the articular surface to prevent devastating "kissing lesions" on the opposing tibial plateau.


In scenarios where the osteochondral fragment is fragmented, frankly necrotic, or structurally insufficient for stable fixation, it must be excised, leaving a full-thickness osteochondral defect
Clinical & Radiographic Imaging Archive





