Mastering Hemivertebra Unilateral Bar Diagnosis: 12 Cases

Key Takeaway
In this comprehensive guide, we discuss everything you need to know about Mastering Hemivertebra Unilateral Bar Diagnosis: 12 Cases. Scoliosis in children, especially juvenile onset, often results from congenital anomalies such as a hemivertebra unilateral bar. This defect involves incomplete vertebral formation and an unsegmented bone bar on the opposite side, causing progressive spinal curvature. Comprehensive MRI of the entire spine is crucial for diagnosing this structural anomaly and evaluating for other potential intraspinal issues.
You are presented with a 3-year-old female in the clinic. The parents are concerned about a rapidly progressive spinal deformity. On examination, there is a rigid thoracic prominence and a truncal shift. You suspect a congenital spinal deformity. Describe your initial assessment strategy and identify the most critical "must-exclude" clinical association.
Candidate: I would take a thorough history focusing on birth and developmental milestones. On physical exam, I would check the spine for rigidity, Adams forward bend for rotation, and a full neurological exam. I would order standing full-length spine radiographs. The most important thing to rule out is VACTERL syndrome.
Candidates often forget to emphasize the importance of looking for cutaneous markers of dysraphism (hairy patches, lipomas) or fail to mention the systemic screening (echocardiogram/renal ultrasound) required for VACTERL, focusing only on the spine.
A structured approach: 1. Clinical: Inspect for cutaneous stigmata of dysraphism, perform a meticulous neurological exam (baseline), and assess for associated limb/chest wall anomalies. 2. Radiographic: Full-length AP/Lateral standing films + supine bending films to assess curve flexibility. 3. Systemic: Explicitly exclude VACTERL association (Vertebral, Anal, Cardiac, Tracheo-esophageal, Renal, Limb) via echocardiogram and renal ultrasound. 4. Pathology: Highlight that in a 3-year-old, this is likely a progressive congenital anomaly requiring early diagnosis due to high risk of thoracic insufficiency.
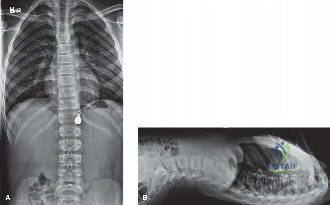
The radiographs confirm a T8 hemivertebra on the right with a contralateral unsegmented bar from T7 to T9. Look at these images. What is the pathomechanical risk of this specific configuration, and how does it influence your surgical decision-making?
Candidate: This is a mixed congenital deformity—the most aggressive type. The hemivertebra drives growth on the convex side, while the bar prevents growth on the concave side, causing severe, rapid progression. Because it is rigid and progressive, I would recommend early surgery to excise the hemivertebra and osteotomize the bar to prevent thoracic insufficiency syndrome.
Suggesting bracing as an initial management strategy. Bracing is contraindicated in fixed congenital structural deformities because it cannot override the biological tether of an unsegmented bar.
Identify this as Winter Type III deformity. Explain the "active growth engine" (hemivertebra) vs. "passive tether" (bar) mechanism. State that progression is inevitable (5–10°/year). Management is early posterior-only hemivertebrectomy and bar osteotomy. Emphasize that preoperative MRI is mandatory to rule out intraspinal anomalies (e.g., tethered cord/syringomyelia) which must be managed before or during deformity correction.
You have decided to proceed with a posterior-only hemivertebrectomy. During the procedure, your neuromonitoring team alerts you to a significant drop in MEPs. What are your immediate steps to address this?
Candidate: I would stop the correction immediately, check the blood pressure, and inspect the wound to see if there is any hardware pressing on the cord. I would also ask the anesthetist to check the patient's oxygenation.
Failing to follow a systematic protocol (The "Wake-up test" or "MAP elevation" sequence). Simply "looking" without a controlled, step-wise algorithm can lead to panic or further damage.
Follow the "Neuromonitoring Troubleshooting Protocol": 1. Cease: Immediately halt the correction maneuver (release tension/distraction). 2. Physiology: Increase Mean Arterial Pressure (MAP > 85 mmHg) to optimize spinal cord perfusion. 3. Assessment: Check for technical causes (hardware impingement, epidural hematoma, or bone fragments). 4. Communication: Ensure the anesthetist optimizes oxygenation and temperature. 5. If signals do not recover, consider a formal "Stagnara wake-up test" if the clinical scenario permits, or reassess the amount of correction intended.
