
A 63-year-old male presents after a diving accident into shallow water. He complains of neck pain, burning dysesthesias in his hands, and significant weakness in his upper extremities, while his lower extremities remain relatively strong. Describe your initial assessment and the likely pathophysiological mechanism of this presentation.

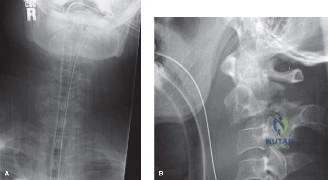
Candidate: The patient likely has Central Cord Syndrome. The mechanism is a hyperextension injury in a patient with pre-existing cervical spondylosis. The spinal cord is compressed by anterior osteophytes and a bulging ligamentum flavum posteriorly, creating a "pincer" effect. I would prioritize ATLS protocols, stabilize the spine, and perform a formal neurologic assessment.
Failing to mention hemodynamic stabilization (MAP targets) or misidentifying the syndrome as a complete spinal cord injury. Candidates often focus purely on the MRI findings without acknowledging the "pincer" mechanism or the importance of cervical spondylosis in the patient's demographic.
Identify this as Central Cord Syndrome. Explain the pathoanatomy: hyperextension causes a mechanical pincer effect via anterior osteophytes and posterior ligamentum flavum infolding. Crucially, explain the neuroanatomy: the corticospinal tract is somatotopically organized with cervical (upper extremity) fibers positioned medially, rendering them most susceptible to central intramedullary injury. Mention the need to avoid spinal shock/hypotension by maintaining a MAP >85 mmHg.
The MRI shows T2 hyperintensity in the cord. How do you distinguish between edema and hematomyelia, and why does this distinction matter for prognosis?
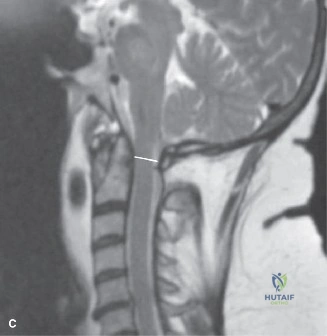
Candidate: T2 hyperintensity suggests edema, which is reversible. Hematomyelia would appear as a hypointense core on T2 or "blooming" artifact on gradient-echo (GRE) sequences. Hematomyelia indicates hemorrhage and tissue necrosis, which is a poor prognostic indicator for neurological recovery.
Assuming that any signal change on MRI implies a need for immediate emergency surgery without differentiating between parenchymal edema and frank hemorrhage.
State clearly that T2 signal intensity alone is non-specific. Use GRE or T2*-weighted sequences to detect "blooming" indicative of intramedullary hemorrhage (hematomyelia). Explicitly state that hemorrhage correlates with axonal disruption and permanent deficit, whereas pure edema (without hemorrhage) often correlates with a better chance of neurological recovery, aiding in informed prognostic discussions with the family.
You have decided to proceed with surgery. Why is a posterior decompression with instrumentation preferred over a laminoplasty in this specific patient?

Candidate: Laminoplasty relies on the spinal cord "drifting" posteriorly. Because this patient has a loss of cervical lordosis, the cord may not drift adequately. Posterior laminectomy and instrumented fusion provides stability and prevents post-laminectomy kyphosis.
Suggesting that laminoplasty is contraindicated in all cervical trauma cases, or failing to identify the biomechanical role of cervical lordosis in cord drift.
Explain that laminoplasty is dependent on the cord's ability to migrate posteriorly away from anterior pathology. In a neutral or kyphotic spine, the cord remains tethered against the anterior osteophytes despite posterior expansion. Therefore, an instrumented fusion is required to provide correction of the alignment and internal stability, which is superior to the motion-sparing benefits of laminoplasty in the context of significant deformity/kyphosis.
Detailed Chapters & Topics
Dive deeper into specialized chapters regarding spine-cases-2