Orthopedic Spine Review | Dr Hutaif Spine Surgery Revie -...

Key Takeaway
Looking for accurate information on ORTHOPEDIC MCQS ONLINE 015Spine? Spinal epidural abscesses require careful management. Risk factors for nonsurgical treatment failure include IV drug abuse, diabetes, age over 65, CRP levels exceeding 115, WBC levels above 12.5, and _Staphylococcus aureus_ infection. Surgical intervention becomes necessary if a patient's neurologic status worsens. For further research, refer to pmid view abstract links provided in studies.
Orthopedic Spine Review | Dr Hutaif Spine Surgery Revie -...
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
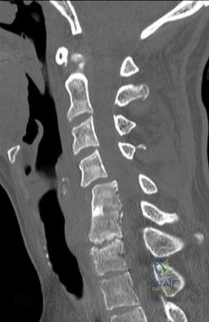
An 82-year-old male with severe chronic obstructive pulmonary disease and heart failure presents after a mechanical fall from a standing height. He reports significant neck pain. Neurologic examination is unremarkable.
Imaging demonstrates a displaced Type II odontoid fracture. What is the most appropriate management for this patient?
Explanation
Question 2
A 65-year-old male presents with progressive clumsiness in his hands, difficulty buttoning his shirt, and a wide-based gait. Physical exam reveals a positive Hoffmann's sign bilaterally.
MRI of the cervical spine demonstrates multilevel degenerative spondylosis with cord compression. Which of the following MRI findings is considered the strongest independent predictor of a poor neurologic recovery following surgical decompression?

Explanation
Question 3
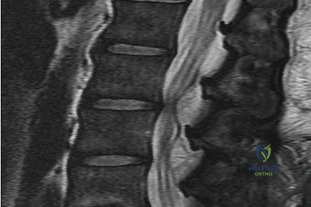
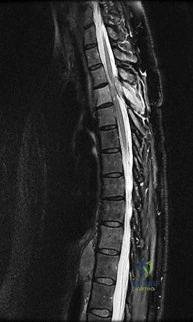
A 55-year-old diabetic male presents with severe mid-thoracic back pain, subjective fevers, and progressive bilateral leg weakness over the past 24 hours. His CRP is 120 mg/L.
An urgent MRI demonstrates a ventral spinal epidural abscess at T8-T10. Which of the following constitutes an absolute indication for urgent surgical decompression?

Explanation
Question 4
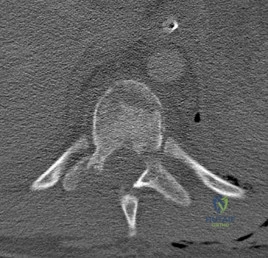
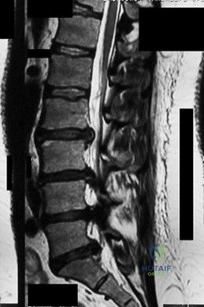
A 35-year-old male construction worker falls 10 feet from scaffolding. He complains of moderate low back pain but has full strength and normal sensation in his lower extremities.
CT imaging shows an L1 burst fracture with 40% loss of anterior vertebral body height and 50% retropulsion into the spinal canal. MRI confirms that the posterior ligamentous complex (PLC) is intact. Based on the Thoracolumbar Injury Classification and Severity (TLICS) score, what is the appropriate score and recommended management?
Explanation
Question 5
A 12-year-old premenarchal female is evaluated for a right thoracic prominence. Standing radiographs reveal a main thoracic curve of 32 degrees.
Her Risser stage is 0. Based on the Bracing in Adolescent Idiopathic Scoliosis Trial (BRAIST), which of the following factors has the most significant dose-dependent correlation with the success of bracing in preventing curve progression to surgical thresholds?

Explanation
Question 6
A 16-year-old elite male gymnast complains of chronic low back pain that is distinctly worse with spinal extension. He has failed 6 months of rest, physical therapy, and bracing.
Radiographs demonstrate a Grade II L5-S1 isthmic spondylolisthesis. He remains symptomatic. What is the most appropriate surgical intervention?

Explanation
Question 7
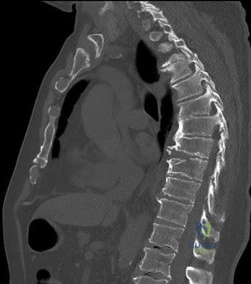
A 60-year-old female with a history of metastatic breast carcinoma presents with intractable mechanical mid-thoracic back pain.
Imaging demonstrates a large lytic lesion involving the T8 vertebral body and bilateral pedicles. There is no epidural tumor extension, and she is neurologically intact. Her Spinal Instability Neoplastic Score (SINS) is calculated to be 11. According to the NOMS framework, what is the next best step in management?

Explanation
Question 8
A 25-year-old female is involved in a motor vehicle collision while wearing only a lap belt. She presents with severe lower back pain and abdominal ecchymosis.
Radiographs and CT reveal a pure bony flexion-distraction injury (Chance fracture) extending through the spinous process, pedicles, and vertebral body of L2. She is neurologically intact. What is an acceptable nonoperative treatment modality?
Explanation
Question 9
A 70-year-old male with pre-existing cervical spondylosis falls forward, striking his chin. He presents to the ER with marked weakness in his hands and upper extremities, but relatively preserved strength in his lower extremities.
What is the primary pathophysiologic mechanism responsible for this specific neurologic deficit?
Explanation
Question 10
A 45-year-old male presents with severe shooting pain down his right anterior thigh and prominent weakness in knee extension. The right patellar reflex is absent.
MRI demonstrates a far-lateral (extraforaminal) disc herniation at the L4-L5 level. Which nerve root is most likely compressed?

Explanation
Question 11
A 6-year-old boy is brought to the trauma bay after a high-speed motor vehicle collision. He exhibits significant upper and lower extremity weakness and diffuse hyperreflexia.
Comprehensive plain radiographs and a non-contrast CT scan of the cervical spine demonstrate no fractures or subluxations. What is the most appropriate next step in his diagnostic workup?

Explanation
Question 12
A 65-year-old female presents with progressive stooped posture, early satiety, and severe low back pain. Radiographs reveal degenerative adult spinal deformity.
Which of the following spinopelvic parameters is most strongly correlated with poorer health-related quality of life (HRQOL) outcomes if it exceeds normative thresholds?
Explanation
Question 13
A 16-year-old male is brought to the clinic by his mother, who is concerned about his "round back." He complains of dull mid-back pain after standing for long periods. Standing lateral radiographs reveal a thoracic kyphosis of 65 degrees.
According to the Sorensen criteria, what specific radiographic finding is required to confirm the diagnosis of classic Scheuermann's disease?
Explanation
Question 14
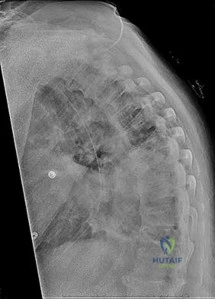
A 45-year-old male with a 20-year history of ankylosing spondylitis presents to the emergency department after a low-energy trip and fall at home. He complains of new-onset, severe lower cervical neck pain. Neurologic examination is unremarkable.
Standard AP, lateral, and odontoid plain radiographs are interpreted as normal. What is the most appropriate next step in management?

Explanation
Question 15
A 60-year-old female undergoes a C3-C6 posterior laminectomy and fusion for severe cervical spondylotic myelopathy.
On postoperative day two, she develops new-onset weakness in her right deltoid and biceps (Grade 2/5 strength) but has no new lower extremity symptoms or sensory loss. She has no distinct focal neck pain. What is the most likely etiology of this new deficit?

Explanation
Question 16
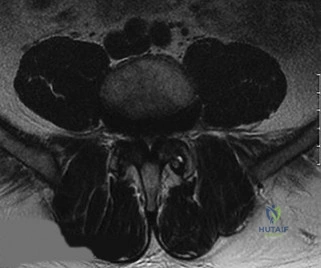
A 40-year-old male presents to the emergency room with acute, severe lower back pain, bilateral sciatica, and perianal numbness. He reports an inability to voluntarily void for the past 14 hours, and an ultrasound reveals a post-void residual volume of 650 mL.
MRI demonstrates a massive L4-L5 disc herniation filling the spinal canal. To maximize the probability of urologic and neurologic recovery, surgical decompression should ideally be performed within what maximum timeframe from the onset of symptoms?
Explanation
Question 17
A 30-year-old male is involved in a high-speed motor vehicle collision.
Radiographs show a traumatic spondylolisthesis of the axis (Hangman's fracture). According to the Levine-Edwards classification, the fracture exhibits severe angulation and minimal translation, and the C2-C3 disc space is widened posteriorly (Type IIA). What is the primary mechanism of injury for this specific fracture pattern?
Explanation
Question 18
A 22-year-old collegiate wrestler presents to the emergency room with severe neck pain and a radicular pain shooting down his right arm after being taken down on his head.
Lateral cervical radiographs reveal approximately 25% anterior subluxation of the C5 vertebral body over C6. What is the classic mechanism of injury for a unilateral facet dislocation?

Explanation
Question 19
During a posterior instrumented fusion of the lumbar spine, the surgeon is preparing to place a pedicle screw at the L4 level.
Which of the following describes the most accurate anatomic landmarks for establishing the starting point for a standard lumbar pedicle screw?

Explanation
Question 20
A 72-year-old male presents with bilateral leg pain, heaviness, and cramping that predictably worsens after walking two blocks.
He states that leaning forward on a shopping cart completely relieves his pain, but standing completely upright without moving fails to relieve the symptoms. His pedal pulses are 2+ bilaterally. What is the most likely diagnosis?
Explanation
Question 21
A 7-year-old boy presents with painful torticollis 10 days after undergoing a routine tonsillectomy. On examination, his head is tilted to the right and his chin is rotated to the left. Neurologic examination is intact. What is the most appropriate initial management?
Explanation
Question 22
A 75-year-old male sustains a Type II odontoid fracture after a ground-level fall. Which of the following radiographic factors is MOST strongly associated with non-union if treated non-operatively in a halo vest?
Explanation
Question 23
In a patient with advanced rheumatoid arthritis presenting for cervical spine evaluation, which of the following radiographic parameters is the most reliable predictor of impending neurologic deficit and indicates an urgent need for surgical stabilization?
Explanation
Question 24
A 65-year-old male with a known history of ankylosing spondylitis presents to the emergency department after a low-speed motor vehicle collision. A CT scan demonstrates a fracture through the C6-C7 disc space extending into the posterior elements.
What is the most appropriate surgical treatment?
Explanation
Question 25
A 35-year-old male is involved in a motor vehicle collision. Examination reveals normal motor and sensory function throughout his upper and lower extremities. CT imaging shows an L1 burst fracture with 15 degrees of local kyphosis and 30% canal compromise. MRI confirms an intact posterior ligamentous complex. According to the Thoracolumbar Injury Classification and Severity (TLICS) score, what is the indicated treatment?
Explanation
Question 26
A 55-year-old male presents with slowly progressive bowel and bladder dysfunction. MRI reveals a large, lobulated presacral mass. CT-guided core needle biopsy shows large cells with abundant, vacuolated cytoplasm (physaliferous cells) in a myxoid background. What is the most appropriate surgical management?
Explanation
Question 27
In adult spinal deformity surgery, the concept of spinopelvic harmony is critical to achieving successful outcomes and minimizing adjacent segment disease.
According to standard matching parameters, a patient's lumbar lordosis (LL) should ideally be restored to within how many degrees of their pelvic incidence (PI)?
Explanation
Question 28
A 12-year-old girl with cerebral palsy (GMFCS level V) has a rapidly progressing neuromuscular scoliosis measuring 85 degrees, with severe associated pelvic obliquity. She is non-ambulatory and has difficulty sitting in her wheelchair. Which surgical strategy is most critical for addressing her pelvic obliquity and restoring sitting balance?
Explanation
Question 29
A 60-year-old male with poorly controlled diabetes mellitus presents with severe back pain, fever, and progressive bilateral lower extremity weakness over the past 24 hours. An urgent MRI confirms an anterior epidural abscess at L2-L3.
Blood cultures are drawn. What is the next best step in management?
Explanation
Question 30
In a patient with cervical Ossification of the Posterior Longitudinal Ligament (OPLL), what does a "negative K-line" on a lateral radiograph imply regarding surgical planning?
Explanation
Question 31
A 14-year-old female with Adolescent Idiopathic Scoliosis is being evaluated for surgery.
Radiographs demonstrate a main thoracic curve of 55 degrees and a lumbar curve of 35 degrees. On lateral bending films, the main thoracic curve corrects to 30 degrees, while the lumbar curve corrects to 15 degrees. According to the Lenke classification, what type of curve is this?
Explanation
Question 32
A 65-year-old male with neurogenic claudication is undergoing a decompressive laminectomy for central and lateral recess stenosis. During the approach, which specific anatomic structure must be undercut or partially resected to effectively decompress the traversing nerve root in the lateral recess?
Explanation
Question 33
A 30-year-old male sustains a C2 fracture in a motor vehicle collision. Radiographs demonstrate a fracture through the pars interarticularis of C2 with severe angular deformity but minimal translation. This is consistent with a Levine-Edwards Type IIA Hangman's fracture. What is the mechanism of injury, and what is the appropriate initial management?
Explanation
Question 34
A 25-year-old male involved in a high-speed MVC wearing a lap belt presents with severe abdominal bruising. A spine CT reveals a transverse fracture line propagating through the spinous process, pedicles, and vertebral body of L2.
Which of the following injuries has the strongest association with this specific fracture pattern?
Explanation
Question 35
A 40-year-old female sustains a U-shaped sacral fracture with spinopelvic dissociation after a fall from a height. According to the Denis classification of sacral fractures, which zone is primarily involved in determining the highest risk of neurologic injury, and what is the approximate historical rate of neurologic injury associated with this zone?
Explanation
Question 36
A 28-year-old male presents with a spinal cord injury following a knife wound to the right side of his mid-thoracic back. Neurological examination reveals complete loss of motor function and proprioception in his right lower extremity, and a loss of pain and temperature sensation in his left lower extremity. Which spinal cord syndrome describes this pattern?
Explanation
Question 37
On a sagittal MRI of the lumbar spine, a vertebral body endplate adjacent to a degenerated disc shows hypointense signal on T1-weighted images and hyperintense signal on T2-weighted images. This finding corresponds to which Modic type, and what does it pathologically represent?
Explanation
Question 38
A 16-year-old male presents with a stiff, painful thoracic hyperkyphosis that does not correct upon hyperextension. Standing lateral radiographs reveal anterior wedging of 4 consecutive thoracic vertebrae by 6 degrees each, along with irregular endplates and prominent Schmorl's nodes. Which condition is the most likely diagnosis?
Explanation
Question 39
A 75-year-old female with severe osteoporosis complains of unremitting back pain 6 months after a minor fall. Her pain worsens significantly when standing and improves when supine. A lateral radiograph demonstrates an intravertebral vacuum cleft sign within a severely compressed T12 vertebral body. What is the eponymous name of this condition?
Explanation
Question 40
A 62-year-old male undergoes a C3-C6 posterior laminectomy and fusion for multilevel cervical spondylotic myelopathy. On post-operative day 2, he develops profound weakness of the right deltoid and biceps (MRC grade 2/5) without new sensory deficits or lower extremity weakness.
What is the most widely accepted primary pathomechanical explanation for this complication?
Explanation
Question 41
In the surgical planning and evaluation of a patient undergoing correction for adult spinal deformity, what is the widely accepted target goal for the relationship between lumbar lordosis (LL) and pelvic incidence (PI) to achieve optimal sagittal balance?
Explanation
Question 42
A 68-year-old male presents to the emergency department after falling forward and striking his chin, sustaining a hyperextension injury to his cervical spine. On examination, he exhibits bilateral upper extremity weakness (motor grade 2/5) but is able to move his lower extremities against resistance (motor grade 4/5). He also has patchy sensory deficits. Which spinal cord syndrome is most likely, and what is its typical prognosis for future ambulation?
Explanation
Question 43
The modified Tokuhashi scoring system is a widely utilized tool to predict life expectancy in patients with metastatic spine disease and to guide surgical decision-making. Which of the following parameters is specifically evaluated in this scoring system?
Explanation
Question 44
A 15-year-old male presents with a progressive rounding of his back. Lateral radiographs are taken to evaluate for Scheuermann's kyphosis. According to the classic Sorensen criteria, which of the following radiographic findings confirms the diagnosis?
Explanation
Question 45
A 55-year-old female undergoes a complex 10-hour posterior spinal fusion for degenerative scoliosis. During the surgery, there is significant estimated blood loss requiring massive transfusion, and prolonged hypotensive anesthesia is maintained. Upon waking in the recovery room, she complains of bilateral, painless vision loss. What is the most common cause of postoperative vision loss (POVL) in this specific clinical scenario?
Explanation
Question 46
Ossification of the posterior longitudinal ligament (OPLL) is a frequent cause of myelopathy. Which of the following describes the most common anatomical location and the most characteristic patient demographic for this condition?
Explanation
Question 47
A 30-year-old male is evaluated in the trauma bay following a high-speed rollover motor vehicle collision. AP and lateral cervical radiographs reveal a unilateral facet dislocation at C5-C6 on the right side. What is the primary mechanism of injury, and what is the typical radiographic appearance on the AP view?
Explanation
Question 48
Recombinant human bone morphogenetic protein-2 (rhBMP-2) possesses potent osteoinductive properties and is used off-label in various spinal fusion procedures. If utilized in anterior cervical spine surgery (e.g., ACDF), what is a well-documented, potentially life-threatening complication that prompted an FDA warning?
Explanation
Question 49
According to the Fielding and Hawkins classification for atlantoaxial rotatory subluxation (AARS) in pediatric patients, what radiographic parameter defines a Type II injury?
Explanation
Question 50
A 14-year-old female gymnast presents with insidious onset lower back pain. Imaging confirms an L5-S1 spondylolisthesis secondary to bilateral stress fractures of the pars interarticularis. According to the Wiltse classification of spondylolisthesis, which type does this represent?
Explanation
Question 51
Pyogenic spondylodiscitis is a serious spinal infection that most frequently affects the lumbar spine in adult patients. What is the most common route of pathogen dissemination leading to this condition?
Explanation
Question 52
A 40-year-old male presents with severe mechanical back pain. Standing lateral radiographs reveal an isthmic spondylolisthesis at L5-S1. The L5 vertebral body has slipped anteriorly by 60% of the width of the S1 endplate. According to the Meyerding classification, what grade is this slip?
Explanation
Question 53
A 45-year-old male presents with severe radiating leg pain. MRI of the lumbar spine reveals a far lateral (extraforaminal) disc herniation at the L4-L5 level. Which nerve root is predominantly compressed by a herniation in this specific location?
Explanation
Question 54
A 65-year-old male with long-standing, advanced ankylosing spondylitis presents to the emergency department after a low-energy mechanical fall. He complains of severe neck pain but has a normal neurological examination. Radiographs and CT reveal a highly unstable, extension-type fracture through the C5-C6 disc space extending into the posterior elements. What is the most appropriate definitive management?
Explanation
Question 55
Degenerative spondylolisthesis most commonly occurs at the L4-L5 level in older adults, particularly females. Which anatomical feature is most strongly associated with the predisposition for developing degenerative spondylolisthesis at this specific level?
Explanation
Question 56
A 40-year-old trauma patient requires the application of a halo-vest for a cervical spine injury. To minimize the risk of iatrogenic injury to the supraorbital and supratrochlear nerves, what is the optimal anatomical placement for the anterior halo pins?
Explanation
Question 57
A 3-year-old child is diagnosed with congenital scoliosis. Radiographs demonstrate a unilateral unsegmented bar with a contralateral hemivertebra at the same level. What is the expected natural history of this specific congenital spinal anomaly?
Explanation
Question 58
Fractures of the odontoid process (dens) are classified into three types by Anderson and D'Alonzo. Type II fractures are notorious for having a high rate of nonunion. What is the primary anatomical reason for this high nonunion rate?
Explanation
Question 59
A 25-year-old male is involved in a high-speed motor vehicle collision while wearing only a lap belt. He sustains a classic Chance fracture of the L2 vertebra. Based on the Denis three-column classification of the spine, which columns are involved in the pathomechanics of a classic Chance fracture?
Explanation
Question 60
In the evaluation of adult spinal deformity, achieving neutral global sagittal balance is a key surgical objective. What is the generally accepted threshold for a normal Sagittal Vertical Axis (SVA), measured as the distance from the C7 plumb line to the posterior superior corner of S1?
Explanation
Question 61
A 24-year-old male arrives at the trauma bay following a high-speed motor vehicle collision. Neurologic examination reveals no voluntary motor function or sensation below the T4 dermatome. His rectal tone is flaccid, and the bulbocavernosus reflex is absent. Which of the following statements regarding his neurologic prognosis is most accurate?
Explanation
Question 62
A 45-year-old female presents with sharp, radiating right arm pain. Examination demonstrates significant weakness in right wrist extension, numbness over the dorsal aspect of the thumb and index finger, and a diminished brachioradialis reflex. An MRI of the cervical spine is most likely to show a posterolateral disc herniation at which of the following levels?
Explanation
Question 63
A 35-year-old male presents after a rollover motor vehicle crash. Imaging demonstrates a bilateral pars interarticularis fracture of C2 with severe angulation and 1 mm of anterior translation (Levine-Edwards Type IIA Hangman's fracture). What maneuver is strictly contraindicated in the management of this specific fracture pattern?
Explanation
Question 64
A 62-year-old male with a 20-year history of ankylosing spondylitis presents to the emergency department complaining of new-onset, severe neck pain after a minor fall from a chair. He has no neurologic deficits. Plain radiographs of the cervical spine demonstrate extensive syndesmophytes but no obvious fracture. What is the most appropriate next step in management?
Explanation
Question 65
A 40-year-old construction worker falls from a ladder and sustains an L1 burst fracture. He is neurologically intact. An MRI of the lumbar spine confirms complete disruption of the posterior ligamentous complex (PLC). According to the Thoracolumbar Injury Classification and Severity (TLICS) score, what is the most appropriate treatment recommendation?
Explanation
Question 66
In the preoperative planning for a 65-year-old female undergoing surgical correction for adult degenerative scoliosis, the surgeon calculates a pelvic incidence (PI) of 55 degrees. According to the SRS-Schwab classification, what is the ideal radiographic target for her postoperative lumbar lordosis (LL)?
Explanation
Question 67
A 68-year-old male undergoes a C3-C7 posterior cervical laminectomy and instrumented fusion for severe cervical spondylotic myelopathy. On postoperative day two, he develops isolated 2/5 weakness in right shoulder abduction and elbow flexion, with no sensory deficits or long tract signs. An MRI shows adequate decompression with no hematoma. What is the most appropriate initial management?
Explanation
Question 68
A 55-year-old male with a history of renal cell carcinoma presents with progressive lower extremity weakness and a solitary, highly destructive lytic lesion at T8 causing spinal cord compression. He is planned for an urgent anterior corpectomy and stabilization. Which of the following preoperative interventions is highly recommended to reduce perioperative morbidity?
Explanation
Question 69
A 22-year-old male is evaluated after a diving accident. An open-mouth odontoid radiograph demonstrates a C1 ring fracture (Jefferson fracture). Which of the following radiographic measurements on the open-mouth view strongly suggests an incompetent transverse atlantal ligament (TAL)?
Explanation
Question 70
A 15-year-old female gymnast complains of chronic lower back pain and tightness in her hamstrings. Imaging reveals a Meyerding Grade II isthmic spondylolisthesis at L5-S1. Despite 6 months of dedicated physical therapy, bracing, and activity modification, her symptoms severely limit her daily activities. What is the most appropriate surgical intervention?
Explanation
Question 71
A 4-year-old boy is brought to the emergency department after falling from a trampoline. He is moving all extremities but guards his neck. A lateral cervical spine radiograph shows 3 mm of anterior displacement of C2 on C3. The Swischuk line (drawn from the anterior aspect of the C1 posterior arch to the C3 posterior arch) passes 1 mm anterior to the anterior aspect of the C2 spinous process. What is the most appropriate next step?
Explanation
Question 72
A 16-year-old male presents with cosmetic concerns regarding a "hunchback" posture. Radiographs reveal hyperkyphosis of the thoracic spine. To establish a formal radiographic diagnosis of Scheuermann's kyphosis (Sorensen criteria), what specific parameters must be met?
Explanation
Question 73
A spine surgeon is performing an anterior cervical discectomy and fusion (ACDF) at C6-C7. Depending on the side of the approach, there are differing risks regarding the recurrent laryngeal nerve (RLN). Which of the following statements regarding the RLN anatomy is true?
Explanation
Question 74
A 70-year-old male complains of bilateral leg and buttock pain that progressively worsens after walking two blocks. The pain is rapidly relieved when he sits or pushes a shopping cart. Pedal pulses are bounding. This classic presentation of neurogenic claudication is primarily caused by hypertrophy of which of the following structures?
Explanation
Question 75
An 80-year-old female sustains a Type II odontoid fracture after a ground-level fall. Her family prefers conservative management over surgery due to her severe cardiac comorbidities. Which of the following is the strongest risk factor for non-union of a Type II odontoid fracture treated with a rigid cervical collar?
Explanation
Question 76
A 72-year-old male with type 2 diabetes presents with progressive dysphagia. Lateral cervical spine radiographs demonstrate flowing, continuous ossification along the anterior aspect of five contiguous vertebral bodies, with preservation of the intervertebral disc spaces. His sacroiliac joints are radiographically normal. What is the most likely diagnosis?
Explanation
Question 77
A 35-year-old male falls from a ladder and sustains localized thoracolumbar pain. He is neurologically intact. CT and MRI confirm an L1 burst fracture with 15 degrees of kyphosis, 30% canal compromise, and an intact posterior ligamentous complex.
Based on the Thoracolumbar Injury Classification and Severity (TLICS) score, what is the most appropriate management?
Explanation
Question 78
A 68-year-old female with adult spinal deformity presents with progressive back pain and forward truncal lean. Her spinopelvic parameters reveal a Pelvic Incidence (PI) of 60 degrees. To achieve a harmonious sagittal profile postoperatively, what is the most appropriate target for her Lumbar Lordosis (LL)?
Explanation
Question 79
A 50-year-old male with severe, long-standing ankylosing spondylitis presents to the emergency department with new-onset neck pain after a low-speed motor vehicle collision. Neurological examination is normal. An initial cross-table lateral radiograph of the cervical spine is read as negative for acute fracture. What is the most appropriate next step in management?
Explanation
Question 80
A 55-year-old Asian male presents with progressive clumsiness in his hands and a wide-based gait. Imaging reveals ossification of the posterior longitudinal ligament (OPLL) from C3 to C6. The sagittal MRI shows that the OPLL mass crosses the K-line (K-line negative), and the cervical spine has 15 degrees of local kyphosis. Which surgical approach is most appropriate?
Explanation
Question 81
A 45-year-old male presents with acute, severe right leg radicular pain. MRI of the lumbar spine reveals a far lateral (extra-foraminal) disc herniation at the L4-L5 level on the right side. Which nerve root is most likely compressed, and what clinical finding is expected?
Explanation
Question 82
A 65-year-old male undergoes a C3-C6 posterior laminectomy and fusion for cervical spondylotic myelopathy. On postoperative day 2, he develops profound weakness of bilateral deltoid and biceps muscles without new sensory deficits. Lower extremity function remains intact. What is the most likely etiology of this complication?
Explanation
Question 83
A 24-year-old male is involved in a high-speed collision and sustains a Levine-Edwards Type IIa traumatic spondylolisthesis of the axis (Hangman's fracture). Radiographs show significant angular deformity with minimal translation. What is the most appropriate management?
Explanation
None
