Adjacent Segment Degeneration: Your Next Spine Case Solved

Key Takeaway
For anyone wondering about Adjacent Segment Degeneration: Your Next Spine Case Solved, Posterior ligamentous disruption is the strongest indicator of instability in thoracolumbar burst fractures, overriding traditional radiographic parameters. This often necessitates surgical intervention, which, in the long term, can contribute to adjacent segment degeneration. Noncontiguous spinal fractures are found in approximately 15% of such cases, emphasizing comprehensive evaluation for these complex injuries.
A 45-year-old male presents after a 20-foot fall. He has a T12-L1 step-off on palpation. You are presented with this CT scan. What are the key radiographic features, and what is your immediate concern regarding the neural elements?

Candidate: The CT shows a comminuted L1 burst fracture with retropulsion into the spinal canal. There is a vertical split through the lamina. My primary concern is neural compression, potentially involving the cauda equina, and the risk of a dural tear given the laminar fracture.
Failing to identify the vertical laminar split as a specific marker for dural entrapment. Candidates often focus only on the percentage of canal compromise without mentioning the morphology of the posterior element injury, which is a specific "red flag" for surgical planning.
Identify this as a Type A4 fracture. Crucially, note that the vertical laminar split suggests an 'opening' of the spinal canal during the burst, which is highly predictive of dural laceration and nerve root incarceration. State that while the patient is neurologically intact (ASIA E), the presence of these fractures mandates careful surgical approach to avoid iatrogenic nerve injury.
You mention the "50-50-25" rule in your assessment. Is this still the gold standard for defining instability in thoracolumbar burst fractures? What actually dictates stability in this patient?
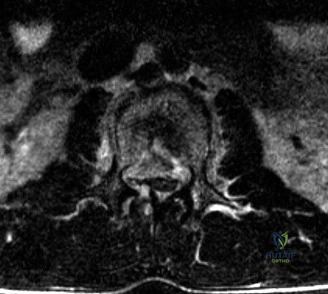
Candidate: No, the 50-50-25 rule is outdated. Stability is determined by the integrity of the Posterior Ligamentous Complex (PLC). In this patient, the MRI shows signal intensity changes in the interspinous ligaments and facet joints, confirming PLC failure, which defines this as unstable.
Relying on the 50% canal compromise or degree of kyphosis as the absolute indication for surgery. Candidates who lack the nuance of the PLC's role fail to demonstrate modern spine trauma knowledge.
Systematically dismiss the 50-50-25 rule as antiquated dogma. Define the PLC (ligamentum flavum, interspinous/supraspinous ligaments, and facet capsules) as the crucial "posterior tension band." Cite the TLICS scoring system, noting that the PLC status adds 3 points, pushing this case into the operative category regardless of the radiographic bony measurements.
The patient requires surgery. You are concerned about long-term outcomes, specifically "Adjacent Segment Degeneration." How does your surgical technique during this index stabilization influence the risk of this occurring?
Candidate: I need to avoid "flatback" deformity. I will contour the rods to restore the patient's native lumbar lordosis and sagittal balance. If I fix the spine in a kyphotic state, the adjacent levels will be forced into hyperlordosis to compensate, leading to accelerated facet and disc degeneration.
Focusing only on "stabilizing the fracture" without mentioning the importance of sagittal alignment. Simply "fixing the screws" without contouring the rods is the most common cause of long-term patient dissatisfaction and revision surgery.
Link the index procedure directly to the biomechanical stress of the unfused segments. Use terms like "sagittal vertical axis (SVA)," "pelvic incidence," and "regional lordosis." Explain that meticulous restoration of these parameters during rod contouring is the primary prophylaxis against adjacent segment disease (ASD).
