Posterior Cervical Arthrodesis: Occiput–C2 and C1–C2 Masterclass
Key Takeaway
Join us in the OR for a masterclass on posterior occipitocervical and C1-C2 arthrodesis. We'll meticulously cover surgical anatomy, advanced preoperative planning, and granular, step-by-step intraoperative execution. Learn critical techniques for stabilization, bone grafting, and hardware application, while gaining insights into managing potential pitfalls and ensuring optimal patient outcomes in complex upper cervical spine instability.
Comprehensive Introduction and Patho-Epidemiology
Welcome, colleagues and fellows, to the operating theater and this definitive masterclass. Today, we are tackling one of the most crucial, unforgiving, and technically demanding arenas of spine surgery: posterior cervical arthrodesis, specifically focusing on the occiput-C2 and C1-C2 articulations. The craniocervical junction (CCJ) is a biomechanical paradox; it is an evolutionary marvel designed to provide immense, multi-axial mobility for the cranium while simultaneously housing and protecting the most critical neural structures in the human body—the brainstem, the spinomedullary junction, and the upper cervical spinal cord.
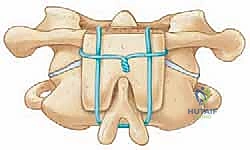
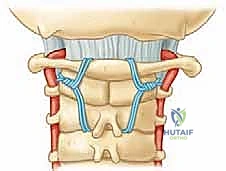
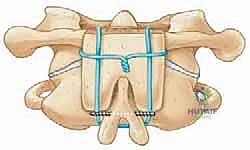
Our primary surgical goals in this region are tripartite: to rigidly stabilize the delicate osteoligamentous architecture, to meticulously decompress and protect the neural elements, and to achieve a robust, enduring arthrodesis. Historically, stabilization of the upper cervical spine relied on sublaminar wiring techniques (such as the Gallie, Brooks-Jenkins, and Dickman constructs) combined with structural bone grafting. While these techniques were foundational, they required prolonged postoperative halo immobilization and were fraught with higher rates of pseudoarthrosis, particularly in rotationally unstable patterns.
The advent of rigid screw-rod constructs—pioneered by Magerl’s transarticular screws and subsequently refined by the Goel-Harms technique of C1 lateral mass and C2 pedicle/pars fixation—has revolutionized our approach. These modern techniques offer superior immediate biomechanical stability, significantly higher fusion rates, and a drastic reduction in the need for rigid external orthoses. However, this biomechanical superiority comes at the cost of steep learning curves and the potential for catastrophic neurovascular complications if the complex regional anatomy is not flawlessly navigated.
Understanding the patho-epidemiology of CCJ disorders is essential for appropriate surgical decision-making. Instability in this region can be broadly categorized into traumatic, inflammatory, congenital, and neoplastic etiologies. Traumatic injuries, such as unstable Jefferson burst fractures, type II odontoid fractures with high risk of nonunion, and traumatic atlanto-occipital dislocations, frequently necessitate rigid internal fixation. Inflammatory arthritides, most notably Rheumatoid Arthritis (RA), have a profound predilection for the upper cervical spine, leading to atlantoaxial subluxation, basilar invagination (cranial settling), and subaxial subluxation. Congenital anomalies, including os odontoideum, Down syndrome (trisomy 21) with inherent ligamentous laxity, and Klippel-Feil syndrome, also present unique challenges that require bespoke surgical strategies.
Detailed Surgical Anatomy and Biomechanics
Before a scalpel ever touches the skin, a profound, three-dimensional understanding of the regional anatomy is paramount. This is not merely an academic exercise; it dictates every trajectory, every dissection plane, and every decision we make in the operating room. The margin for error at the craniocervical junction is measured in millimeters.
Osteology of the Craniocervical Junction
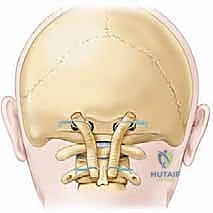
The occipitocervical articulation is a highly specialized functional unit formed by the occiput, the atlas (C1), and the axis (C2). This trifecta provides a vast degree of mobility, maintained by a robust network of ligamentous structures and uniquely shaped synovial joints. The occipital condyles articulate with the superior articular facets of C1, primarily facilitating flexion and extension (approximately 25 degrees) with a limited degree of lateral bending.
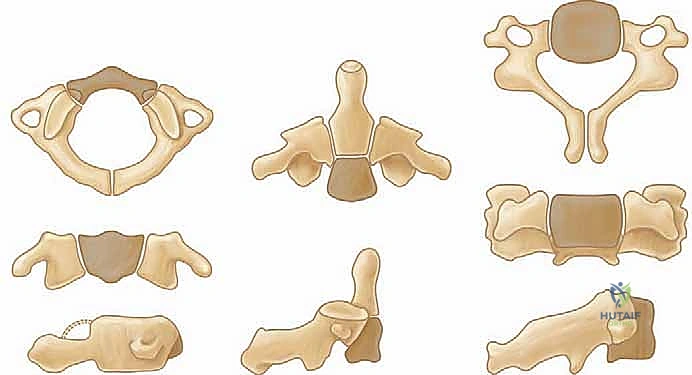
The atlas (C1) is unique; after skeletal maturity, it lacks a true vertebral body, presenting instead as a ring-shaped bone composed of anterior and posterior arches connected by bulky lateral masses. Its superior articular facets are concave and cup-shaped to receive the occipital condyles. The inferior articular facets are relatively flat and circular, articulating with C2. The dorsal facet of the anterior arch of C1 provides a synovial articulation for the dens of C2.
The axis (C2) is characterized by the prominent dens (odontoid process), which projects superiorly from its body, acting as a pivot point. The dens articulates with the anterior arch of C1, forming the median atlantoaxial joint. Critically, over 50% of the total axial rotation of the head and neck (approximately 40 degrees to each side) occurs at this C1-C2 articulation. The C2 pedicles and pars interarticularis are critical corridors for modern instrumentation, requiring precise anatomical knowledge of their morphometry and relationship to the vertebral artery.
Ligamentous Stabilizers of the Upper Cervical Spine
The stability of the upper cervical spine relies heavily on strong, intrinsic ligamentous structures. Excessive movement at these junctions, whether due to traumatic rupture, inflammatory pannus degradation, or congenital laxity, is the hallmark of craniocervical instability. The tectorial membrane is a direct cranial continuation of the posterior longitudinal ligament (PLL), providing substantial posterior support to the dens and the C1-C2 complex, limiting excessive flexion and vertical translation.
The cruciate ligament is arguably the most critical stabilizer. Its transverse band (the transverse atlantal ligament) acts as the primary restraint against atlantoaxial anteroposterior translation. It holds the dens firmly against the posterior border of the anterior arch of C1. Rupture or incompetence of the transverse ligament leads to anterior subluxation of C1 on C2, drastically reducing the space available for the spinal cord.
The alar and apical ligaments act as crucial secondary stabilizers. The alar ligaments extend obliquely from the superolateral aspects of the odontoid process to the medial aspects of the occipital condyles, acting to limit excessive axial rotation and lateral bending. The apical ligament is a thin band extending from the tip of the dens to the anterior margin of the foramen magnum, offering minor stabilizing support but serving as an important anatomical landmark.
Pediatric Developmental Considerations
It is a fundamental tenet of pediatric orthopedics that the pediatric upper cervical spine is not merely a miniature adult spine. Significant developmental differences exist that heavily influence both diagnosis and surgical management. The atlas (C1) develops from three primary ossification centers: an anterior centrum (which eventually forms the anterior arch) and two neural arches, typically visible by age one. The neurocentral synchondroses fuse with the anterior arch around 7 years of age. These synchondroses can easily be mistaken for fractures on pediatric radiographs, a critical diagnostic pitfall.
The axis (C2) has a highly complex embryological origin, derived from five primary ossification centers (two neural arches, two halves of the dens, and the vertebral body) and two secondary centers (the ossiculum terminale and the inferior ring apophysis). The two halves of the odontoid are usually fused at birth but can occasionally persist as a "dens bicornis."
The dentocentral synchondrosis, which separates the dens from the body of C2, is a critical radiographic landmark. It typically closes between ages 5 and 7 and appears as a radiolucent line resembling a "cork in a bottle" on open-mouth views until complete ossification. Misinterpreting this normal developmental anatomy as a basilar odontoid fracture is a common error. The tip of the dens appears around age 3 and fuses by age 12; failure of this fusion results in a persistent ossiculum terminale.
Critical Neurovascular Topography
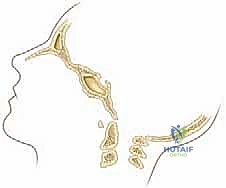
The neurovascular anatomy of the CCJ is notoriously complex and highly variable. The vertebral arteries (V3 segment) pass through the transverse foramina of C2, loop laterally to pass through the transverse foramina of C1, and then course medially along the superior surface of the C1 posterior arch (in the vertebral groove, or sulcus arteriae vertebralis) before piercing the posterior atlanto-occipital membrane and dura to enter the foramen magnum.
During C1 lateral mass screw placement, the vertebral artery is at extreme risk if the dissection is carried too far laterally along the posterior arch, or if the screw trajectory is excessively lateral or superior. For C2 pedicle and pars screws, care must be taken to stay within the bony confines, as the vertebral artery frequently creates a deep groove in the inferior aspect of the C2 superior articular facet. Preoperative CT angiography is absolutely invaluable for mapping their course and identifying anomalies such as a "high-riding" vertebral artery or a persistent first intersegmental artery.
The primary concern in upper cervical instability is mechanical compression of the spinal cord or brainstem. Our surgical approach must prioritize neural decompression and protection. Additionally, the greater occipital nerve (the dorsal ramus of the C2 spinal nerve) exits below the inferior nuchal line and ascends towards the scalp. It is frequently encountered during posterior exposures and C1-C2 joint preparation. Injury or entrapment of this nerve can lead to debilitating postoperative occipital neuralgia. Careful subperiosteal dissection and avoidance of excessive bipolar cautery in the lateral gutters are essential.

Exhaustive Indications and Contraindications
The decision to proceed with posterior cervical arthrodesis at the craniocervical junction must be based on a rigorous assessment of clinical symptoms, neurological status, and radiographic evidence of instability or compression.
Pathologies Necessitating Arthrodesis
Traumatic injuries are a frequent indication. While many upper cervical fractures can be managed non-operatively with rigid orthoses, specific patterns demand surgical stabilization. These include unstable Jefferson fractures with an associated rupture of the transverse ligament (indicated by >6.9 mm of lateral mass overhang on an open-mouth view), Type II odontoid fractures in the elderly or those with a high risk of nonunion (e.g., displacement >5 mm, posterior displacement, comminution), and atlanto-occipital dislocation, which is inherently highly unstable and carries a high mortality rate.
Inflammatory conditions, particularly Rheumatoid Arthritis, frequently lead to progressive, destructive instability. Atlantoaxial subluxation (AAS) is the most common manifestation, but basilar invagination (cranial settling)—where the odontoid process migrates superiorly through the foramen magnum to compress the brainstem—is the most lethal. Arthrodesis is indicated for intractable pain, progressive neurological deficit, or impending catastrophic instability. Congenital anomalies such as os odontoideum, marked by a separate ossicle cranial to the C2 body leading to gross C1-C2 instability, strongly warrant fusion if symptomatic or if the space available for the cord is critically compromised.
Contraindications to Posterior Approaches
While posterior arthrodesis is versatile, specific contraindications exist. Active posterior cervical infection precludes instrumentation. Irreducible anterior spinal cord compression (e.g., fixed basilar invagination or a large irreducible retrodental pannus) may require a staged anterior transoral or endoscopic endonasal odontoidectomy prior to posterior stabilization. Furthermore, severe osteoporosis or an aberrant vertebral artery trajectory (e.g., bilateral high-riding vertebral arteries precluding C2 pedicle or pars screw placement) requires significant modification of the surgical plan, potentially relying on alternative fixation points or sublaminar wiring techniques.
| Category | Indications for Occipitocervical/C1-C2 Arthrodesis | Contraindications (Absolute & Relative) |
|---|---|---|
| Trauma | Unstable Type II Odontoid fractures; Transverse ligament rupture; Atlanto-occipital dislocation; Unstable Jefferson fractures. | Active systemic or local infection (Absolute); Severe concomitant polytrauma precluding prone positioning (Relative). |
| Inflammatory | Rheumatoid Arthritis with basilar invagination, irreducible atlantoaxial subluxation, or progressive myelopathy. | Irreducible anterior cord compression requiring anterior release first (Relative). |
| Congenital | Symptomatic Os Odontoideum; Down Syndrome with severe ADI widening/neurologic deficit; Klippel-Feil instability. | Aberrant bilateral vertebral artery anatomy precluding safe screw placement (Relative - requires alternative fixation). |
| Neoplastic | Primary or metastatic tumors destroying the C1-C2 lateral masses or occipital condyles causing instability. | Terminal prognosis with <3 months expected survival (Relative). |
| Iatrogenic | Post-laminectomy instability; Failed prior upper cervical fusion (pseudoarthrosis). | Inadequate bone stock for any form of fixation (Absolute). |
Preoperative Planning, Templating, and Patient Positioning
Fellows, the success of these complex fusions hinges entirely on meticulous preoperative planning. The operating room is not the place for discovery. This is where we anticipate anatomical challenges, mitigate neurovascular risks, and define our precise surgical strategy.
Advanced Imaging and Craniometric Analysis
Standard radiographs remain the starting point. We mandate anteroposterior (AP), open-mouth odontoid, and lateral (neutral and dynamic flexion-extension) cervical spine views. On lateral flexion-extension views, we diagnose atlantoaxial instability by assessing the Atlantodental Interval (ADI). In adults, an ADI >3 mm is abnormal; in children, >4-5 mm indicates instability. More importantly, we measure the Space Available for the Spinal Cord (SAC), measured from the posterior border of the dens to the anterior border of the posterior tubercle of C1. A SAC of <14 mm is highly predictive of neurological compromise.


For complex instability, particularly basilar invagination, craniometry lines are essential.
* McRae's Line: Connects the anterior and posterior rims of the foramen magnum. The odontoid tip should be below this line.
* Chamberlain's Line: Drawn from the posterior margin of the hard palate to the posterior margin of the foramen magnum. The odontoid tip should be <6 mm above this line.
* McGregor's Line: Drawn from the hard palate to the most caudal point of the occiput. Odontoid projection >4.5 mm above this line indicates basilar impression.
* Wackenheim's Line: Drawn parallel to the posterior clivus; it should intersect or lie tangential to the posterior tip of the odontoid.
* Power Ratio: Used to assess atlanto-occipital dissociation. A ratio >1.0 indicates anterior translation of the occiput on the atlas.
High-resolution CT scanning with 3D reconstructions is mandatory. It provides invaluable information regarding bony anomalies, facet joint integrity, and the exact morphometry of the C2 pedicles and pars. We routinely utilize CT angiography to map the trajectory of the vertebral arteries, specifically looking for high-riding vessels that would preclude standard C2 pedicle screw placement. MRI is essential for identifying pathological changes in the dura mater, spinal cord signal changes (myelomalacia), and the extent of inflammatory pannus.
Neuromonitoring and Airway Management
Intraoperative neurologic monitoring is the standard of care. Somatosensory Evoked Potentials (SSEPs), Transcortical Motor Evoked Potentials (tcMEPs), and continuous electromyography (EMG) provide real-time feedback on spinal cord and nerve root function. Baseline signals must be obtained prior to positioning, as the act of proning an unstable patient can induce catastrophic cord compression.
Airway management requires close collaboration with anesthesiology. Flexible fiberoptic intubation with manual in-line axial stabilization is mandatory to minimize cervical motion. Avoid aggressive neck extension during intubation at all costs.
Prone Positioning and Reduction Techniques
Patient positioning is a highly choreographed critical step. The patient is carefully proned onto a radiolucent operating table (such as a Jackson table). We typically utilize a Mayfield cranial tong system to maintain rigid cranial control, though a horseshoe headrest can be used for less unstable cases. The head is positioned in a neutral or slightly extended posture (the "military tuck") to optimize the cervical lordosis and facilitate reduction of C1-C2 subluxations.
Ensure the abdomen hangs free to decrease intra-abdominal pressure, thereby reducing epidural venous engorgement and minimizing intraoperative bleeding. Reverse Trendelenburg positioning can further aid in venous drainage. Lateral fluoroscopy is brought in immediately after positioning to confirm alignment and ensure that no iatrogenic subluxation has occurred during the turn.


Step-by-Step Surgical Approach and Fixation Technique
The surgical execution demands meticulous hemostasis, precise anatomical dissection, and flawless instrumentation.
Surgical Exposure and Decompression
A standard midline posterior approach is utilized. The incision extends from the external occipital protuberance (inion) down to the spinous process of C3 or C4, depending on the planned construct. Deep dissection is carried out strictly in the avascular midline ligamentum nuchae. Subperiosteal dissection exposes the occiput, the posterior arch of C1, and the lamina and spinous process of C2.
Extreme caution is exercised when dissecting laterally along the superior margin of the C1 posterior arch to avoid injuring the vertebral artery residing in the vertebral groove. Dissection should not proceed further than 1.5 cm from the midline on the superior border of C1. The C1-C2 facet joints are exposed by defining the medial border of the lateral mass and sweeping the venous plexus (which can bleed profusely) laterally. Bipolar electrocautery and hemostatic agents (e.g., Gelfoam, Floseal) are essential here. The C2 nerve root (greater occipital nerve) is identified and mobilized inferiorly to allow access to the C1-C2 joint space.

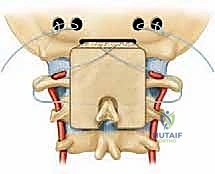
Instrumentation of the Atlas and Axis
For C1 lateral mass screws (Goel-Harms technique), the entry point is at the intersection of the posterior arch and the midpoint of the C1 lateral mass. The C2 nerve root is gently retracted caudally. A pilot hole is created with a high-speed burr or awl. The trajectory is approximately 10 to 15 degrees medial (convergent) and 15 degrees cephalad, aiming toward the anterior tubercle of C1. The hole is drilled, tapped, and a polyaxial screw (typically 3.5 mm diameter, 26-30 mm length) is inserted.
For C2 pedicle screws, the entry point is in the cranial and lateral quadrant of the C2 isthmus. The trajectory is approximately 20 to 25 degrees medial and 20 degrees cephalad, navigating strictly within the bony confines of the pedicle to avoid the laterally situated vertebral artery and the medially situated spinal cord. In cases where the vertebral artery is high-riding, C2 pars interarticularis screws or translaminar screws offer safe, biomechanically sound alternatives.
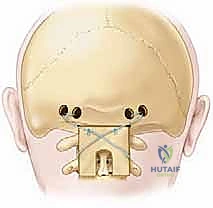
Occipitocervical Fixation Strategies
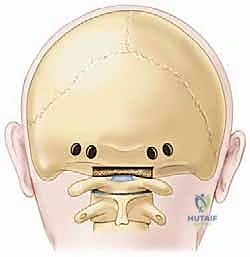
When the pathology demands extension to the occiput, an occipital plate or independent occipital screws are utilized. The thickest and most robust bone of the occiput is located at the external occipital protuberance (inion) and along the superior nuchal line. The bone thins significantly inferiorly towards the foramen magnum and laterally into the cerebellar fossae.
The occiput is carefully drilled using a drill with a depth stop to prevent plunging into the venous sinuses (specifically the transverse and confluence of sinuses). Bicortical purchase is optimal but must be executed with extreme caution to avoid dural laceration and massive venous hemorrhage. Once the occipital hardware and cervical screws are placed, pre-contoured rods are seated. The rods must be bent meticulously to match the patient's native occipitocervical lordosis; forcing the rod into the screws can lead to hardware pullout or iatrogenic malalignment.


Bone Grafting and Arthrodesis Optimization
Hardware provides immediate temporary stability; biological fusion provides the permanent cure. The posterior arch of C1, the lamina of C2, and the occiput are decorticated using a high-speed burr until bleeding cancellous bone is exposed. The C1-C2 facet joints should be vigorously denuded of cartilage and packed with local autograft or allograft.
Structural bone grafting is often employed. A tricortical iliac crest autograft can be wedged between the occiput and C2 spinous process or wired between C1 and C2. Copious amounts of cancellous autograft (often harvested from the posterior superior iliac spine) or high-quality allograft mixed with osteoinductive agents are packed over the decorticated surfaces.


Complications, Incidence Rates, and Salvage Management
Despite meticulous technique, posterior cervical arthrodesis carries a distinct and potentially severe complication profile. Anticipation and rapid management are the hallmarks of a master surgeon.
Intraoperative Adverse Events
The most dreaded intraoperative complication is injury to the vertebral artery (incidence ~1-4%). This typically occurs during aggressive lateral dissection of C1, errant C1 lateral mass drilling, or breach of the C2 pedicle. If arterial bleeding is encountered, the immediate priority is rapid tamponade with hemostatic agents (e.g., bone wax, surgical patties) and manual pressure. If bleeding is controlled, the screw can sometimes be placed to act as a permanent tamponade. If bleeding is uncontrollable or bilateral injury is suspected, immediate endovascular consultation for coiling or stenting is required. Bilateral vertebral artery injury is often fatal due to brainstem infarction.
Dural tears can occur during decompression or occipital drilling. Primary repair is often difficult due to the depth and limited access. Management typically involves patching with a synthetic or autologous fascial graft, application of a fibrin sealant, and placing the patient on flat bed rest postoperatively to prevent cerebrospinal fluid (CSF) fistulas.
Postoperative and Long-Term Complications
Postoperative C2 radiculopathy (occipital neuralgia) is common, occurring in up to 10-15% of patients due to manipulation, retraction, or entrapment of the greater occipital nerve during C1-C2 joint preparation. While often transient, it can be debilitating and may require targeted nerve blocks or, rarely, surgical transection of the nerve.
Hardware failure and pseudoarthrosis (nonunion) are long-term concerns, though their incidence has dramatically decreased (<5%) with the advent of rigid screw-rod constructs. Risk factors include poor bone quality (osteoporosis, RA), inadequate decortication, smoking, and failure to achieve rigid immobilization. Salvage management typically requires revision surgery, extension of the fusion construct, and enhancement of the biological milieu with autograft or bone morphogenetic proteins (BMP).
| Complication | Estimated Incidence | Prevention Strategy | Salvage / Management Protocol |
|---|---|---|---|
| Vertebral Artery Injury | 1.0% - 4.0% | Pre-op CTA; meticulous trajectory planning; avoid lateral C1 dissection. | Immediate tamponade (bone wax/screw); contralateral side must NOT be instrumented; Endovascular consult. |
| Occipital Neuralgia (C2) | 5.0% - 15.0% | Gentle C2 root retraction; avoid excessive bipolar cautery near the ganglion. | Gabapentinoids; Occipital nerve blocks; C2 nerve root transection (if intractable). |
| Dural Tear / CSF Leak | 2.0% - 6.0% | Depth stops on occipital drills; careful use of Kerrison rongeurs. | Primary repair if possible; Dural substitute overlay; Fibrin glue; Lumbar drain (refractory). |
| Pseudoarthrosis | 2.0% - 5.0% | Meticulous joint decortication; aggressive autografting; rigid fixation. | Revision instrumentation; extension of fusion levels; use of rhBMP-2 or iliac crest autograft. |
| Hardware Prominence | 5.0% - 10.0% | Low-profile occipital plates; countersinking screws where possible. | Hardware removal only after solid bony fusion is confirmed on CT scan. |
Phased Postoperative Rehabilitation Protocols
The immediate and long-term postoperative management is critical
Clinical & Radiographic Imaging Archive

