Orthopedic Spine Review | Dr Hutaif Spine Surgery Revie -...
Key Takeaway
For anyone wondering about ORTHOPEDIC MCQS ONLINE 012 SPINE, When a 56-year-old presents with leg weakness and an unsteady, wide-based gait without discrete lower extremity motor weakness, even with mild lumbar stenosis, the next appropriate action is MRI of the thoracic and cervical spine to evaluate for spinal cord compression. This helps resolve a common diagnostic res question a yearold patient’s symptoms can present, especially when lumbar findings are insufficient.
Orthopedic Spine Review | Dr Hutaif Spine Surgery Revie -...
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
A 14-year-old gymnast presents with lower back pain exacerbated by extension. Radiographs show a grade II spondylolisthesis at L5-S1. What is the most likely pathological mechanism?
Explanation
Question 2
A 65-year-old man presents with progressive clumsiness in his hands, difficulty buttoning his shirt, and a broad-based gait. Hoffman's sign is positive bilaterally. MRI shows severe cervical stenosis at C4-C6. What is the most reliable MRI predictor of poor surgical outcome after decompression?
Explanation
Question 3
A 13-year-old Risser 1 female presents with a right thoracic curve of 35 degrees. What is the most appropriate management?
Explanation
Question 4
A 35-year-old male falls from a height and sustains an L1 burst fracture. He is neurologically intact. Radiographs and CT show 20 degrees of kyphosis, 50% loss of vertebral body height, and 40% canal compromise. What is the most appropriate initial treatment?
Explanation
Question 5
An 80-year-old woman is involved in a low-speed motor vehicle collision. CT scan reveals a Type II odontoid fracture with 2 mm of posterior displacement. She is neurologically intact. What is the most appropriate treatment?
Explanation
Question 6
A 55-year-old man with a long-standing history of ankylosing spondylitis presents with severe back pain after a minor fall. Radiographs do not clearly show a fracture, but he has pinpoint tenderness at T10. What is the next best step in management?
Explanation
Question 7
A 30-year-old man presents after a motor vehicle accident with neck pain. Imaging shows a traumatic spondylolisthesis of the axis (C2) with bilateral pars fractures, 4 mm of translation, and 12 degrees of angulation (Levine-Edwards Type II). What is the recommended treatment?
Explanation
Question 8
A 42-year-old man presents with 6 weeks of right leg pain radiating down the lateral aspect of his calf to the dorsum of his foot. He has a 3/5 weakness in extensor hallucis longus (EHL). He has failed conservative therapy. Which nerve root is most likely compressed?
Explanation
Question 9
A 72-year-old man with a history of cervical stenosis falls forward, striking his chin. He presents with profound upper extremity weakness, particularly in his hands, but is able to walk with a spastic gait. His lower extremities have 4/5 strength. What is the most likely pathophysiological mechanism?
Explanation
Question 10
A 25-year-old motorcyclist sustains a Denis Zone 3 sacral fracture. Which of the following deficits is most likely to be associated with this injury pattern?
Explanation
Question 11
A 55-year-old intravenous drug user presents with progressive back pain, fevers, and acute onset of lower extremity weakness and urinary retention. MRI reveals an epidural fluid collection with peripheral enhancement compressing the thecal sac at T10. What is the most appropriate management?
Explanation
Question 12
A 6-year-old boy presents with a low posterior hairline, short webbed neck, and limited cervical range of motion. Radiographs show multiple fused cervical vertebrae. Which of the following systems is most crucial to evaluate in this patient?
Explanation
Question 13
A 40-year-old male presents to the emergency department with acute onset severe lower back pain, bilateral sciatica, perineal numbness, and inability to void for the past 12 hours. Post-void residual volume is 500 cc. MRI shows a massive L4-L5 disc extrusion filling the spinal canal. What is the optimal timeframe for surgical intervention to maximize the chance of full neurological recovery?
Explanation
Question 14
A 68-year-old female presents with neurogenic claudication and L4-L5 grade I degenerative spondylolisthesis. She has failed 6 months of conservative treatment. Dynamic radiographs show 4 mm of translation upon flexion. What is the gold standard surgical treatment?
Explanation
Question 15
A 16-year-old boy presents with an increasingly prominent mid-back curvature and aching pain after prolonged sitting. Lateral radiographs reveal a thoracic kyphosis of 65 degrees. What radiographic finding is necessary to confirm the diagnosis of Scheuermann's disease?
Explanation
Question 16
A 60-year-old Japanese male presents with progressive clumsiness of his hands, difficulty walking, and hyperreflexia in both upper and lower extremities. Lateral cervical radiograph reveals dense ossification extending vertically along the posterior aspect of the C3 to C6 vertebral bodies. Which surgical approach is generally preferred if the canal occupying ratio is 60% and cervical alignment is lordotic?
Explanation
Question 17
A 55-year-old woman with a history of breast cancer presents with severe, progressive midthoracic back pain. Neurological exam reveals 4/5 strength in the bilateral iliopsoas and hyperreflexia at the knees. MRI shows a destructive lesion at T8 with epidural extension compressing the spinal cord. She has an estimated life expectancy of 18 months. What is the most appropriate management?
Explanation
Question 18
A 65-year-old female with long-standing Rheumatoid Arthritis presents with neck pain and occipital headaches. Lateral cervical flexion-extension radiographs show an anterior atlantodental interval (ADI) of 11 mm. What is the most appropriate management?
Explanation
Question 19
A 60-year-old man on warfarin for atrial fibrillation undergoes a lumbar laminectomy. Six hours postoperatively, he complains of excruciating back pain and develops profound, rapidly progressive bilateral lower extremity weakness and saddle anesthesia. What is the most urgent next step?
Explanation
Question 20
An 82-year-old female presents with acute severe midline back pain after lifting a heavy box. Radiographs reveal a new T12 compression fracture with 20% loss of anterior height and no posterior wall involvement. She is neurologically intact. What is the best initial management?
Explanation
Question 21
A 5-year-old boy presents with a short neck, low posterior hairline, and limited cervical range of motion. Radiographs reveal congenital fusion of the C3-C4 and C5-C6 vertebral bodies. Which of the following is the most appropriate next screening test to evaluate for commonly associated anomalies?
Explanation
Question 22
A 65-year-old male undergoes a C3-C6 posterior cervical laminectomy and instrumented fusion for cervical spondylotic myelopathy. On post-operative day 2, he develops isolated, profound weakness of the right deltoid and biceps (Grade 2/5). Sensation is intact, and his lower extremity function is unchanged. Post-operative MRI shows adequate decompression with no epidural hematoma. What is the most likely etiology of this complication?
Explanation
Question 23
A 55-year-old male with a long-standing history of ankylosing spondylitis presents to the emergency department with severe back pain after a ground-level fall.
A CT scan demonstrates a fracture through the T8-T9 intervertebral disc space extending into the posterior elements. He is neurologically intact. What is the most appropriate management?
Explanation
Question 24
In evaluating a patient for adult spinal deformity correction, which of the following spinopelvic parameters is morphological, established at skeletal maturity, and remains fixed regardless of patient positioning or pelvic retroversion?
Explanation
Question 25
A 45-year-old male presents with severe right anterior thigh pain and weakness in knee extension. An MRI of the lumbar spine reveals a far lateral (extraforaminal) disc herniation at the L3-L4 level on the right. Which nerve root is most likely compressed by this specific herniation?
Explanation
Question 26
During correction of an adolescent idiopathic scoliosis deformity, there is a sudden and sustained loss of motor evoked potentials (MEPs) bilaterally, while somatosensory evoked potentials (SSEPs) remain at baseline. The patient's mean arterial pressure (MAP) is currently 85 mmHg. What is the most appropriate immediate step in management?
Explanation
Question 27
A 25-year-old male suffers a stab wound to the thoracic spine. Neurological examination reveals loss of motor function and proprioception in the right lower extremity, and loss of pain and temperature sensation in the left lower extremity. This presentation implies injury to which of the following combinations of spinal cord tracts?
Explanation
Question 28
A 14-year-old gymnast presents with chronic low back pain. Conservative management for 6 months has failed.
Radiographs demonstrate a Grade II isthmic spondylolisthesis at L5-S1. What is the recommended surgical treatment?
Explanation
Question 29
An 82-year-old female presents with neck pain following a motor vehicle collision. CT scan reveals a Type II odontoid fracture. Comorbidities include severe COPD and osteoporosis. She is neurologically intact. If she is managed non-operatively with a rigid cervical collar, which of the following is an established major risk factor for non-union?
Explanation
Question 30
A 16-year-old male presents with a 6-month history of well-localized mid-back pain that is worse at night and dramatically improves with ibuprofen. Imaging reveals a 1.2 cm sclerotic lesion with a central lucent nidus in the left lamina of T8. What is the most appropriate definitive management if conservative measures are poorly tolerated?
Explanation
Question 31
A 55-year-old diabetic male presents with 2 weeks of worsening back pain and low-grade fever. MRI reveals a ventral epidural abscess from L2 to L4. He has full motor strength, intact sensation, normal bowel/bladder function, and no mechanical instability. Blood cultures rapidly grow methicillin-sensitive Staphylococcus aureus (MSSA). What is the most appropriate initial management?
Explanation
Question 32
A 22-year-old male falls from a height of 30 feet. He has bilateral lower extremity weakness and perineal numbness.
Imaging demonstrates a transverse fracture through the S1-S2 level connecting bilateral longitudinal transforaminal sacral fractures (U-type fracture). What is the primary biomechanical goal of surgical fixation for this specific pattern?
Explanation
Question 33
A 19-year-old female is involved in a high-speed motor vehicle collision wearing only a lap belt. Radiographs show a transverse fracture through the spinous process, pedicles, and vertebral body of L2. Based on the mechanism of injury, what is the most commonly associated concomitant pathology?
Explanation
Question 34
According to the Thoracolumbar Injury Classification and Severity Score (TLICS), which of the following cumulative scores serves as a definitive indication for operative management?
Explanation
Question 35
A 42-year-old male presents to the emergency department with acute onset of severe low back pain, bilateral sciatica, and subjective perineal numbness. Which of the following clinical evaluations is considered the most sensitive indicator for objective urinary retention in the setting of suspected cauda equina syndrome?
Explanation
Question 36
Which of the following radiographic findings is most characteristic of early spinal tuberculosis (Pott's disease) when compared to pyogenic spondylodiscitis?
Explanation
Question 37
During the physical examination of a patient with suspected cervical spondylotic myelopathy, the examiner firmly flicks the distal phalanx of the middle finger into flexion. A positive response consists of reflexive flexion of the interphalangeal joint of the thumb and index finger. What is the name of this clinical sign?
Explanation
Question 38
A 60-year-old male of East Asian descent presents with progressive clumsiness in his hands and an unsteady gait.
Lateral cervical radiographs reveal a continuous, dense radiopaque stripe immediately posterior to the vertebral bodies from C3 to C6. What is the most likely diagnosis?
Explanation
Question 39
Which of the following is an essential radiographic criterion for the diagnosis of Diffuse Idiopathic Skeletal Hyperostosis (DISH) according to Resnick and Niwayama?
Explanation
Question 40
Within the Neurologic, Oncologic, Mechanical, and Systemic (NOMS) framework for evaluating metastatic spine tumors, which of the following tumor histologies is considered highly radioresistant, often prompting separation surgery followed by stereotactic radiosurgery (SRS) when causing epidural spinal cord compression?
Explanation
Question 41
A 75-year-old man falls and complains of severe neck pain. Radiographs reveal a Type II odontoid fracture. Which of the following parameters is the most significant risk factor for nonunion if managed conservatively?
Explanation
Question 42
A 35-year-old man falls from a 10-foot ladder. Imaging reveals an L1 burst fracture with widening of the interspinous distance, indicating a definite posterior ligamentous complex (PLC) disruption. He is neurologically intact. According to the Thoracolumbar Injury Classification and Severity (TLICS) score, what is the score and appropriate management?
Explanation
Question 43
A 60-year-old woman with a 20-year history of rheumatoid arthritis presents with progressive hand clumsiness and a broad-based gait. Cervical spine radiographs demonstrate atlantoaxial instability. What is the most critical radiographic parameter used to assess her risk of impending permanent neurological deterioration?
Explanation
Question 44
A 72-year-old man with cervical spondylosis suffers a hyperextension injury. He presents with 2/5 strength in his bilateral upper extremities and 4/5 strength in his lower extremities. He has variable sensory loss. Which specific spinal tract injury is responsible for this classic presentation?
Explanation
Question 45
A 45-year-old man develops acute, severe left anterior thigh pain and new-onset weakness in left knee extension. MRI of the lumbar spine reveals a massive far lateral (extraforaminal) disc herniation at the L3-L4 level on the left. Which nerve root is most likely compressed?
Explanation
Question 46
A 60-year-old man presents with severe back pain and a solitary L2 vertebral body metastasis secondary to renal cell carcinoma. He has impending cord compression, and his estimated life expectancy is 18 months. What is the most appropriate surgical treatment strategy?
Explanation
Question 47
When applying the Lenke classification system for adolescent idiopathic scoliosis, a minor curve must be included in the surgical fusion construct if it is deemed 'structural'. What radiographic criterion defines a structural minor curve in the coronal plane?
Explanation
Question 48
A 25-year-old diver impacts the bottom of a pool, sustaining an axial load injury. An open-mouth odontoid radiograph demonstrates a Jefferson fracture. According to Spence's rule, a combined lateral mass overhang of C1 on C2 greater than what measurement implies incompetence of the transverse alar ligament?
Explanation
Question 49
A 40-year-old woman presents with saddle anesthesia, bilateral sciatica, and acute urinary retention with a post-void residual volume of 450 mL. MRI confirms a massive L4-L5 central disc extrusion. What is the generally accepted optimal time window to perform decompression to maximize the chance of urologic recovery?
Explanation
Question 50
A 25-year-old male involved in a high-speed motor vehicle collision sustains a thoracolumbar fracture. Radiographs and CT demonstrate a fracture extending horizontally through the spinous process, pedicles, and vertebral body of L1. What is the primary pathomechanism of this specific injury pattern?
Explanation
Question 51
In an adult patient presenting with an L5-S1 isthmic spondylolisthesis and unilateral radicular leg pain, which nerve root is most commonly compressed, and what is the primary anatomical site of this compression?
Explanation
Question 52
A 68-year-old male with pre-existing cervical spondylosis falls forward and strikes his chin, causing a hyperextension injury to his neck. On examination, he has motor strength of 2/5 in his hands and 4/5 in his lower extremities. What is the most likely diagnosis?
Explanation
Question 53
A 55-year-old male with known renal cell carcinoma presents with progressive lower extremity weakness and bowel dysfunction.
Imaging reveals a destructive metastatic lesion at L3 causing mechanical collapse and severe canal stenosis. Operative decompression and stabilization are planned. What is the most critical preoperative step?
Explanation
Question 54
A 60-year-old patient undergoes a posterior cervical laminectomy and instrumented fusion from C3 to C6 for severe cervical myelopathy. On postoperative day 2, he develops profound new-onset weakness in his bilateral deltoids and biceps, with preserved strength elsewhere. Sensation is intact. What is the most likely etiology?
Explanation
Question 55
A 45-year-old obese male undergoes a complex T10-Pelvis posterior spinal fusion. Postoperatively, he complains of painless, profound bilateral vision loss. Examination reveals sluggish pupillary responses and optic disc swelling. Which of the following risk factors is most strongly associated with this complication?
Explanation
Question 56
A 30-year-old female sustains a Levine-Edwards Type IIa Hangman's fracture. Radiographs demonstrate an angulated C2 pars fracture with minimal translation. What treatment modality is strictly contraindicated in this specific injury pattern?
Explanation
Question 57
Which of the following congenital spinal anomalies carries the highest risk of rapid curve progression and invariably requires early surgical intervention?
Explanation
Question 58
A 50-year-old diabetic male presents with severe unremitting back pain. MRI shows findings consistent with L4-L5 discitis and osteomyelitis. He is neurologically intact, hemodynamically stable, and blood cultures are negative. What is the most appropriate next step in management?
Explanation
Question 59
A 70-year-old male with long-standing ankylosing spondylitis presents to the emergency department with neck pain after a ground-level fall. Neurologic exam is intact. CT scan reveals a transverse fracture through the C5-C6 disc space. What is the most dreaded immediate complication that must be monitored for in this patient?
Explanation
Question 60
A 42-year-old female presents with neck pain radiating down her left arm. Physical examination reveals a diminished brachioradialis reflex, decreased sensation over her left thumb and index finger, and weakness in wrist extension. Which cervical nerve root is most likely affected?
Explanation
Question 61
A 35-year-old male falls from a ladder and sustains an L1 burst fracture. He is neurologically intact. MRI confirms the posterior ligamentous complex (PLC) is completely intact. According to the Thoracolumbar Injury Classification and Severity (TLICS) score, what is the best initial management?
Explanation
Question 62
During a complex anterior thoracolumbar reconstruction, the surgeon must be mindful of the Artery of Adamkiewicz. Which of the following best describes the typical origin and function of this critical vessel?
Explanation
Question 63
A 22-year-old male requires the placement of a halo vest for a complex upper cervical spine injury.
Where is the correct anatomical "safe zone" for the placement of the anterior halo pins in an adult?
Explanation
Question 64
A 45-year-old man presents with severe lower back pain and right leg pain. An MRI reveals a far lateral (extraforaminal) disc herniation at the L4-L5 level. Which nerve root is most likely compressed, and what clinical finding would be expected?
Explanation
Question 65
An 82-year-old woman sustains a Type II odontoid fracture after a ground-level fall. Which of the following is considered a significant risk factor for nonunion if treated conservatively with a hard cervical collar?
Explanation
Question 66
A 50-year-old male presents with radiating neck pain into his left arm. Physical examination demonstrates weakness in wrist flexion, finger extension, and triceps extension, along with an absent triceps reflex. Which cervical nerve root is most likely affected?
Explanation
Question 67
In the surgical planning for an adult patient with severe sagittal imbalance, achieving proper spinopelvic parameters is critical to postoperative clinical success. What is the universally accepted target for the mismatch between Pelvic Incidence (PI) and Lumbar Lordosis (LL)?
Explanation
Question 68
A 70-year-old man with pre-existing cervical spondylosis sustains a hyperextension injury to his neck. He presents with severe motor weakness in his hands and arms, but is able to move his legs with only mild weakness. What is the typical long-term prognosis for this specific spinal cord injury syndrome?
Explanation
Question 69
A 55-year-old diabetic male presents with acute, severe, localized back pain and a low-grade fever. He has a history of recent intravenous catheter placement. Neurological examination is currently normal. What is the most common causative organism if an MRI confirms a spinal epidural abscess?
Explanation
Question 70
During the evaluation of a 2-year-old child with congenital scoliosis, various vertebral anomalies are noted on plain radiographs. Which of the following structural anomalies carries the highest risk for rapid and severe curve progression?
Explanation
Question 71
A 24-year-old male arrives at the trauma bay after a motorcycle accident with flaccid paralysis below the T4 level, absent reflexes, and hypotension. Which of the following clinical signs definitively indicates the resolution of the temporary physiological state known as spinal shock?
Explanation
Question 72
A 60-year-old patient with known systemic malignancy presents with an isolated spinal metastasis causing mechanical back pain but no acute neurological deficits. Which of the following primary tumor types is highly radiosensitive, often making radiation therapy the primary treatment modality over excisional surgery?
Explanation
Question 73
A 35-year-old unrestrained passenger is involved in a motor vehicle collision. Radiographs demonstrate a unilateral facet dislocation in the cervical spine.
What is the primary mechanism of injury leading to this specific pathology?
Explanation
Question 74
A 5-year-old is newly diagnosed with congenital scoliosis. Before contemplating any surgical intervention, which of the following imaging workups is strictly mandatory due to the high incidence of associated syndromic anomalies?
Explanation
Question 75
A 58-year-old male undergoes a 10-hour posterior spinal fusion for complex adult deformity, complicated by 2.5 liters of blood loss. Postoperatively, he complains of painless, bilateral visual loss. What is the most common etiology of postoperative visual loss (POVL) in this setting?
Explanation
Question 76
A 19-year-old female presents after a high-speed collision where she was wearing only a lap seatbelt. Imaging reveals a Chance fracture of L1. What concomitant injury must be highly suspected and urgently ruled out?
Explanation
Question 77
A 45-year-old male with long-standing Ankylosing Spondylitis (AS) reports new-onset neck pain after a minor trip-and-fall at home. Initial AP and lateral cervical radiographs are read as "normal with expected syndesmophytes." What is the most appropriate next step in management?
Explanation
Question 78
A 6-year-old boy is brought to the ER with transient lower extremity weakness and paresthesia following a trampoline fall. Complete spine X-rays and CT scans are negative for fracture or subluxation. An MRI reveals central cord edema. What biomechanical factor best explains the occurrence of Spinal Cord Injury Without Radiographic Abnormality (SCIWORA) in this patient?
Explanation
Question 79
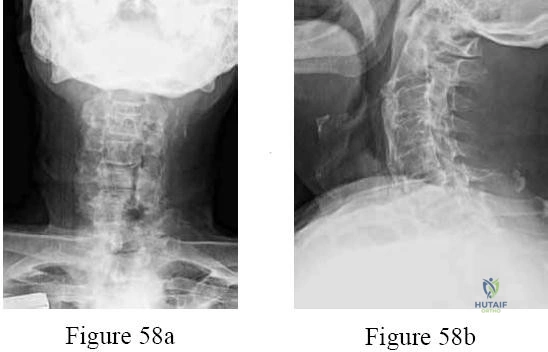
Which of the following demographic and clinical profiles is most characteristic of Ossification of the Posterior Longitudinal Ligament (OPLL)?
Explanation
None
