Posterior Glenohumeral Dislocation: Epidemiology, Anatomy, Diagnosis & Management
Key Takeaway
Posterior glenohumeral dislocation (PGHD) is an uncommon shoulder injury, often misdiagnosed, accounting for 2-5% of dislocations. It's classically linked to high-energy muscle contractions from epileptic seizures or electric shock. Key features include a reverse Hill-Sachs lesion (humeral head impaction) and potentially a reverse Bankart lesion (posterior labral tear), requiring prompt diagnosis and tailored management.
Introduction and Epidemiology
Posterior glenohumeral dislocation (PGHD) is a relatively uncommon injury, accounting for only 2-5% of all shoulder dislocations, significantly less frequent than anterior dislocations. Despite its lower incidence, it is often misdiagnosed or diagnosed late, with up to 50% of acute posterior dislocations missed on initial presentation, leading to increased morbidity and complex treatment challenges. The delay in diagnosis is largely attributable to the subtle clinical presentation and often misinterpreted conventional radiographs.
The typical mechanism of injury involves indirect trauma, classically associated with high-energy muscle contractions such as those occurring during epileptic seizures, electroconvulsion therapy, or electrical shock. This is often referred to memorably as the "3 Es" (Epilepsy, Electrocution, Ethanol withdrawal). Direct trauma to the anterior aspect of the shoulder, leading to posterior displacement of the humeral head, can also cause this injury, particularly in high-impact sports, football line play, or motor vehicle accidents where an axial load is applied to a flexed, adducted, and internally rotated arm. Other less common causes include falls, assaults, or iatrogenic injuries during surgical procedures. PGHD can be unilateral or bilateral, with bilateral dislocations almost pathognomonic for seizure activity or electrocution.
Acute diagnosis and prompt reduction are paramount to minimize complications such as avascular necrosis (AVN) of the humeral head, recurrent instability, chronic pain, and debilitating functional limitations. The recognition of specific radiographic signs and a high index of clinical suspicion are critical for timely intervention. Patients classically present with the arm locked in internal rotation, an inability to externally rotate the shoulder, a prominent coracoid process anteriorly, and a flattened anterior shoulder contour.
Surgical Anatomy and Biomechanics
A thorough understanding of the intricate anatomy and biomechanics of the glenohumeral joint is essential for addressing posterior shoulder dislocations. The glenohumeral joint is inherently unstable, relying heavily on dynamic stabilizers (rotator cuff muscles) and static stabilizers (capsuloligamentous structures, glenoid labrum, negative intra-articular pressure) for its stability.
Static Stabilizers
The static stabilizers are the primary restraints at the extremes of motion.
* Glenoid Labrum: The fibrocartilaginous rim deepens the glenoid fossa, increasing its articular surface area and providing an attachment point for the joint capsule and glenohumeral ligaments. A reverse Bankart lesion, an avulsion of the posterior labrum and periosteum from the posterior glenoid rim, is a common finding in PGHD.
* Glenohumeral Ligaments: The superior, middle, and inferior glenohumeral ligaments reinforce the joint capsule. The posterior band of the inferior glenohumeral ligament (PIGHL) and the posterior capsule are the primary static stabilizers resisting posterior translation of the humeral head, especially when the arm is in internal rotation, flexion, and adduction.
* Glenoid Retroversion: The glenoid typically has slight retroversion (0-7 degrees). Excessive glenoid retroversion or hypoplasia of the posterior glenoid rim can significantly predispose a patient to posterior instability.
Dynamic Stabilizers
The dynamic stabilizers compress the humeral head into the glenoid concavity during active motion.
* Rotator Cuff Muscles:
* Subscapularis: The largest and most powerful rotator cuff muscle, primarily responsible for internal rotation and anterior stability. In posterior dislocations, the subscapularis and pectoralis major often remain unopposed, pulling the humerus into severe internal rotation and exacerbating the impaction of the humeral head against the glenoid rim.
* Infraspinatus and Teres Minor: These muscles primarily externally rotate the humerus and contribute significantly to posterior and inferior stability by compressing the humeral head into the glenoid. In PGHD, severe internal rotation often leads to a mechanical block due to the humeral head impacting the posterior glenoid rim, completely preventing external rotation and rendering these dynamic stabilizers ineffective.
Osseous Structures
The bony architecture dictates the congruency of the joint. In posterior dislocations, the osseous structures frequently sustain significant damage due to the immense forces involved.
* Humeral Head: The articular surface of the humeral head can sustain an impaction fracture on its anteromedial aspect when forcefully driven against the posterior glenoid rim. This lesion is termed a reverse Hill-Sachs lesion (or McLaughlin lesion) and is a hallmark of posterior dislocations. Its size and location are critical determinants of joint stability and reducibility.
- Glenoid Fossa: Fractures of the posterior glenoid rim (reverse bony Bankart lesions) frequently occur as the humeral head is forced posteriorly. The integrity of the posterior glenoid is critical; defects greater than 20% of the glenoid width severely compromise the ability of the joint to remain reduced, often necessitating structural bone grafting.
Indications and Contraindications
The management of posterior glenohumeral dislocations is dictated by the chronicity of the injury, the size of the anteromedial humeral head defect (reverse Hill-Sachs lesion), the presence of glenoid bone loss, and the functional demands of the patient. Acute dislocations without significant bone loss are typically managed non-operatively with closed reduction, whereas chronic, locked dislocations or those with substantial osseous defects require surgical intervention.
| Clinical Scenario | Operative Indications | Non Operative Indications |
|---|---|---|
| Acute Dislocation (< 3 weeks) | Irreducible by closed means; Post-reduction instability; Large reverse Hill-Sachs (>20%); Posterior glenoid fracture (>20%) | Reducible closed; Stable in external rotation post-reduction; Small reverse Hill-Sachs (<20%); No significant glenoid fracture |
| Chronic Dislocation (> 3 weeks) | Locked posterior dislocation; Persistent pain and functional limitation; Young, active patient | Elderly, low-demand patient with minimal pain (skillful neglect); High surgical risk |
| Humeral Head Defect Size | Defect > 20-25% (requires transfer or grafting); Defect > 40-50% (requires arthroplasty) | Defect < 20% (often stable after reduction) |
| Recurrent Instability | Recurrent posterior subluxation/dislocation; Failure of conservative rehabilitation | First-time dislocation; Compliant with physical therapy |
Contraindications to surgical intervention include active local or systemic infection, severe medical comorbidities precluding anesthesia, advanced neuroarthropathy (Charcot joint), and non-compliant patients who cannot adhere to strict postoperative rehabilitation protocols. In elderly, low-demand patients with chronic, locked posterior dislocations that are relatively painless, non-operative management ("skillful neglect") may be a viable option, as the risks of complex reconstruction or arthroplasty may outweigh the functional benefits.
Pre Operative Planning and Patient Positioning
Thorough preoperative planning is essential for the successful management of posterior shoulder dislocations, particularly in chronic or complex cases involving significant bone loss.
Diagnostic Imaging Modalities
Standard radiographic evaluation must include a true anteroposterior (Grashey) view, a scapular Y view, and an axillary lateral view. The axillary lateral view is the most critical radiograph for confirming the diagnosis of a posterior dislocation, as it clearly demonstrates the posterior displacement of the humeral head relative to the glenoid.
On the AP view, several subtle signs may indicate a posterior dislocation:
* Lightbulb Sign: The humeral head appears symmetrical and rounded like a lightbulb due to fixed internal rotation.
* Trough Line Sign: A dense vertical line on the medial aspect of the humeral head representing the impacted reverse Hill-Sachs lesion.
* Rim Sign: Widening of the glenohumeral joint space (greater than 6 mm) between the anterior glenoid rim and the medial aspect of the humeral head.
Computed Tomography (CT) without and with 3D reconstruction is the gold standard for preoperative planning. It allows for precise quantification of the reverse Hill-Sachs defect (calculated as a percentage of the articular surface) and assessment of posterior glenoid bone loss or retroversion. Magnetic Resonance Imaging (MRI) or MR arthrography is indicated to evaluate the integrity of the posterior labrum, capsule, and rotator cuff, particularly in cases of recurrent posterior instability without massive bone loss.
Anesthesia and Patient Positioning
Surgical intervention can be performed under regional anesthesia (interscalene block) combined with general anesthesia. Patient positioning depends on the planned surgical approach and the specific procedures required.
- Beach Chair Position: Preferred for open anterior approaches (deltopectoral) used for subscapularis transfers (McLaughlin procedure), lesser tuberosity transfers (modified McLaughlin), anterior structural allografts, or shoulder arthroplasty. It allows for excellent visualization of the anterior structures and easy conversion to arthroplasty if necessary.
- Lateral Decubitus Position: Often preferred for arthroscopic posterior stabilization or open posterior approaches. The arm is placed in balanced suspension (typically 45 degrees of abduction and 15-20 degrees of forward flexion). This position provides excellent visualization of the posterior compartment and facilitates access to the posterior glenoid for labral repair or bone block procedures.
An Examination Under Anesthesia (EUA) should be performed prior to sterile prep and drape to assess the direction and degree of instability, the presence of a mechanical block, and the range of motion.
Detailed Surgical Approach and Technique
The surgical management of PGHD is highly individualized, ranging from arthroscopic soft tissue stabilization to complex open bony reconstructions and arthroplasty.
Closed Reduction Principles
For acute dislocations, closed reduction should be attempted promptly under procedural sedation or intra-articular local anesthetic block. The technique involves gentle in-line traction applied to the adducted arm, combined with anteriorly directed pressure on the posterior aspect of the humeral head. Counter-traction is applied via a sheet wrapped around the patient's thorax. Once the humeral head clears the posterior glenoid rim, gentle external rotation is applied to complete the reduction. Forceful external rotation must be strictly avoided prior to disengaging the head from the glenoid, as it can cause a spiral fracture of the surgical neck of the humerus.
Arthroscopic Posterior Labral Repair
Arthroscopic stabilization is indicated for recurrent posterior instability associated with a reverse Bankart lesion, posterior capsular redundancy, or a small, non-engaging reverse Hill-Sachs lesion.
- Portal Placement: A standard posterior viewing portal is established. An anterior portal is created via the rotator interval for instrumentation. An accessory posteroinferior portal (7 o'clock position) may be established for optimal anchor placement along the posterior glenoid rim.
- Diagnostic Arthroscopy: The joint is evaluated for labral tears, capsular laxity, chondral damage, and the size of the reverse Hill-Sachs lesion.
- Preparation: The posterior labrum and capsule are mobilized from the glenoid neck using a periosteal elevator. The glenoid rim is decorticated with a burr to create a bleeding bone bed to enhance healing.
- Repair: Suture anchors are placed along the posterior glenoid rim, typically starting inferiorly at the 6 or 7 o'clock position and progressing superiorly to the 9 or 10 o'clock position. Sutures are passed through the capsulolabral tissue, incorporating a capsular plication to address redundancy, and tied to secure the tissue to the glenoid rim.
Subscapularis and Lesser Tuberosity Transfers
For reverse Hill-Sachs lesions involving 20% to 40% of the articular surface, filling the defect is necessary to prevent engagement on the posterior glenoid rim.
- McLaughlin Procedure: The original technique described by McLaughlin involves a deltopectoral approach. The internervous plane is developed between the deltoid (axillary nerve) and the pectoralis major (medial and lateral pectoral nerves). The subscapularis tendon is detached from its insertion on the lesser tuberosity and sutured directly into the reverse Hill-Sachs defect.
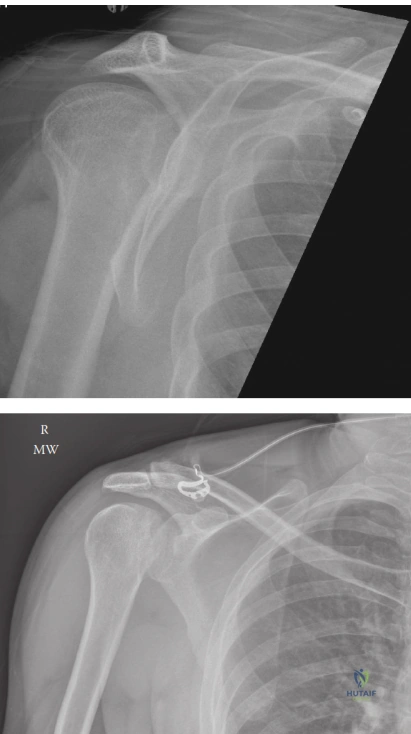
- Modified McLaughlin Procedure (Neer Modification): This is the modern standard for medium-sized defects. Instead of transferring the tendon alone, the lesser tuberosity is osteotomized along with the attached subscapularis tendon. The bone block is then mobilized and secured into the reverse Hill-Sachs defect using cancellous screws. This provides bone-to-bone healing, which is biomechanically superior to tendon-to-bone healing.
Structural Allograft Reconstruction
For massive reverse Hill-Sachs defects (typically 40% to 50% of the articular surface) in young, active patients where arthroplasty is undesirable, structural allograft reconstruction is indicated.
- Approach: A standard deltopectoral approach is utilized.
- Preparation: The reverse Hill-Sachs defect is debrided of fibrous tissue and sculpted to a geometric shape (usually a wedge or rectangle) to accept the graft.
- Graft Sizing: A structural allograft, typically a femoral head or humeral head allograft, is measured and cut to precisely match the dimensions of the defect.
- Fixation: The allograft is impacted into the defect and secured with headless compression screws or countersunk cancellous screws. The articular surface of the graft must be perfectly flush with the native humeral articular cartilage to prevent accelerated glenoid wear.
Arthroplasty Considerations
In older, lower-demand patients, or in cases where the reverse Hill-Sachs defect exceeds 50% of the articular surface or is accompanied by severe osteoarthritis, shoulder arthroplasty is the treatment of choice.
- Hemiarthroplasty: May be considered if the glenoid cartilage is pristine. However, outcomes are often compromised by eccentric posterior wear.
- Total Shoulder Arthroplasty (TSA): Generally preferred if there is any evidence of glenoid cartilage wear. Careful attention must be paid to glenoid version; excessive retroversion may require asymmetric reaming or bone grafting to prevent posterior subluxation of the prosthetic joint.
- Reverse Total Shoulder Arthroplasty (rTSA): Indicated in the setting of an irreparable rotator cuff tear or severe posterior glenoid bone loss that cannot be managed with standard TSA components.
Complications and Management
The management of posterior glenohumeral dislocations is fraught with potential complications, stemming from both the initial trauma and the subsequent surgical interventions. A comprehensive understanding of these risks is necessary for appropriate patient counseling and surgical planning.
| Complication | Estimated Incidence | Etiology / Pathophysiology | Prevention and Salvage Strategies |
|---|---|---|---|
| Missed Diagnosis | Up to 50% acutely | Subtle clinical signs; failure to obtain or properly interpret axillary lateral radiographs. | High clinical suspicion; mandatory axillary or scapular Y views for all shoulder trauma; CT scan if radiographs are equivocal. |
| Avascular Necrosis (AVN) | 5% - 15% | Disruption of the ascending branch of the anterior circumflex humeral artery; prolonged dislocation time. | Prompt reduction; meticulous surgical dissection preserving soft tissue attachments. Salvage: Arthroplasty. |
| Recurrent Instability | 10% - 20% | Failure to address capsular redundancy, posterior glenoid bone loss, or large reverse Hill-Sachs lesions. | Accurate preoperative measurement of bone defects; appropriate selection of bone block or transfer procedures over soft-tissue only repairs. Salvage: Revision stabilization or arthroplasty. |
| Post-Traumatic Osteoarthritis | 20% - 30% | Initial chondral impact; chronic subluxation; over-tightening of the posterior capsule (capsulorrhaphy arthropathy). | Anatomic restoration of joint congruency; avoiding excessive capsular plication. Salvage: Total Shoulder Arthroplasty. |
| Hardware Failure / Migration | < 5% | Poor bone quality; non-compliance with rehabilitation; improper screw placement. | Use of appropriate fixation constructs; countersinking screws in allografts; strict adherence to postoperative immobilization. Salvage: Hardware removal, revision fixation. |
| Neurovascular Injury | 1% - 3% | Injury to the axillary nerve during posterior approaches or suprascapular nerve during posterior glenoid dissection. | Meticulous identification of internervous planes; avoiding excessive medial retraction on the posterior glenoid neck. |
Post Operative Rehabilitation Protocols
Postoperative rehabilitation must be carefully tailored to the specific surgical procedure performed, balancing the need to protect the repair with the goal of restoring functional range of motion. The guiding principle for posterior stabilization is the avoidance of stress on the posterior capsule and any anterior transfers.
Phase 1: Protection and Immobilization (Weeks 0-4)
* The shoulder is immobilized in a specialized orthosis (often a "gunslinger" brace) that holds the arm in 10 to 20 degrees of external rotation and slight abduction. This position relaxes the posterior capsule and keeps the reverse Hill-Sachs lesion (or repair) away from the posterior glenoid rim.
* Strict avoidance of internal rotation, adduction, and forward flexion across the body.
* Active range of motion of the elbow, wrist, and hand is encouraged to prevent distal stiffness and edema.
Phase 2: Early Controlled Motion (Weeks 4-8)
* The brace is gradually weaned.
* Initiation of passive and active-assisted range of motion.
* Forward flexion and abduction are progressed as tolerated.
* Internal rotation is carefully introduced but restricted to neutral or minimal degrees to protect the posterior reconstruction.
* Submaximal isometric strengthening of the deltoid and rotator cuff begins.
Phase 3: Strengthening and Dynamic Stability (Weeks 8-12)
* Progression to full active range of motion.
* Isotonic strengthening of the rotator cuff and periscapular musculature. Focus on the posterior cuff (infraspinatus, teres minor) to enhance dynamic posterior stability.
* Closed kinetic chain exercises are introduced to improve proprioception and joint stability.
Phase 4: Return to Activity (Months 3-6+)
* Advanced strengthening and plyometric exercises.
* Sport-specific or work-specific functional training.
* Return to contact sports or heavy manual labor is generally restricted until 6 months postoperatively, contingent upon the restoration of near-normal strength, full dynamic stability, and radiographic healing of any osseous procedures.
Summary of Key Literature and Guidelines
The evolution of treatment for posterior glenohumeral dislocations is heavily grounded in foundational orthopedic literature. Understanding these key studies provides context for current treatment algorithms.
- McLaughlin (1952): Originally described the pathomechanics of the anteromedial humeral head impaction fracture (reverse Hill-Sachs lesion) and proposed the transfer of the subscapularis tendon into the defect to prevent engagement. This remains a cornerstone concept in the management of PGHD.
- Neer (Modified McLaughlin): Recognized the biomechanical limitations of tendon-to-bone healing in the original McLaughlin procedure and introduced the modification of transferring the lesser tuberosity with the subscapularis tendon, allowing for superior bone-to-bone healing.
- Gerber et al.: Pioneered the use of structural allografts (femoral head) for the reconstruction of massive reverse Hill-Sachs defects, demonstrating excellent long-term survivorship and functional outcomes in young patients who are poor candidates for arthroplasty.
- Provencher et al.: Contributed significantly to the modern understanding of glenoid and humeral head bone loss, establishing volumetric analysis techniques via 3D CT. Their work solidified the guidelines that defects greater than 20-25% of the articular surface generally require structural intervention rather than soft tissue repair alone.
- Bradley et al.: Provided extensive data on arthroscopic posterior stabilization, highlighting the importance of addressing capsular redundancy and identifying the posterior band of the IGHL as the critical structure in preventing posterior translation.
Current guidelines emphasize a high index of suspicion in the emergency setting, mandatory orthogonal imaging, precise quantification of bone loss via advanced imaging, and a tailored surgical approach that addresses both soft tissue laxity and osseous defects to restore durable glenohumeral stability.
