Arthroscopic Management of Posterior Glenohumeral Instability and Hill-Sachs Lesions
Key Takeaway
Arthroscopic management of posterior glenohumeral instability requires meticulous portal placement and capsulolabral repair. For engaging Hill-Sachs lesions, the arthroscopic remplissage technique provides a robust solution by tenodesing the infraspinatus and posterior capsule into the humeral defect. This guide details the step-by-step surgical techniques, biomechanical principles, and postoperative rehabilitation protocols for posterior humeral avulsion of the glenohumeral ligament (PHAGL) and Hill-Sachs remplissage procedures.
Comprehensive Introduction and Patho-Epidemiology
Posterior glenohumeral instability represents a complex, multifaceted spectrum of shoulder pathology that has historically been underdiagnosed, underappreciated, and technically demanding to manage. While anterior glenohumeral instability dominates the clinical landscape, posterior instability accounts for approximately 2% to 10% of all shoulder instability presentations. The epidemiology of posterior instability typically involves distinct patient populations, most notably collision athletes (such as American football linemen and ice hockey players), weightlifters, and individuals subjected to high-energy trauma, seizure disorders, or electrical shock. The classic mechanism of injury involves an axial load applied to a forward-flexed, adducted, and internally rotated arm, driving the humeral head posteriorly against the glenoid rim.
Among the primary anatomical lesions responsible for recurrent posterior instability is the Posterior Humeral Avulsion of the Glenohumeral Ligament (PHAGL). Unlike the more common posterior Bankart lesion—which involves the detachment of the capsulolabral complex from the posterior glenoid rim—a PHAGL involves the catastrophic failure of the posterior band of the inferior glenohumeral ligament (IGHL) at its humeral insertion. This lesion is particularly insidious because it often occurs without an associated osseous Bankart lesion or overt labral tear, making it easily missed on standard non-contrast magnetic resonance imaging (MRI) or during a cursory diagnostic arthroscopy. Failure to recognize and anatomically repair a PHAGL lesion is a well-documented cause of persistent, disabling posterior instability and surgical failure.
Concurrently, the management of glenohumeral instability frequently involves addressing bipolar bone loss, a scenario where both glenoid and humeral head osseous defects coexist and interact. In the context of anterior instability, the Hill-Sachs lesion—a posterolateral humeral head impaction fracture created when the humeral head dislocates and impacts the anterior glenoid rim—poses a significant biomechanical challenge. When a Hill-Sachs lesion is deemed "engaging" (meaning the defect drops over the anterior glenoid rim during abduction and external rotation, levering the joint out of socket), it mandates targeted surgical intervention to prevent recurrent dislocation.
The arthroscopic remplissage (derived from the French word for "to fill") technique, originally conceptualized and popularized by Wolf and Purchase, offers a highly effective, joint-preserving solution. By converting an intra-articular osseous defect into an extra-articular one via the tenodesis of the infraspinatus tendon and posterior capsule into the Hill-Sachs defect, the remplissage effectively alters the glenoid track. This comprehensive textbook chapter details the intricate pathoanatomy, rigorous preoperative evaluation, and step-by-step operative techniques for both the arthroscopic repair of a PHAGL lesion and the Hill-Sachs remplissage, providing orthopedic surgeons with an evidence-based framework for mastering these complex instability patterns.
Detailed Surgical Anatomy and Biomechanics
A profound understanding of the static and dynamic stabilizers of the glenohumeral joint is an absolute prerequisite for successful arthroscopic management of posterior instability and bipolar bone loss. The glenohumeral joint is inherently unstable, relying heavily on a delicate interplay between osseous geometry, capsulolabral integrity, and neuromuscular control. The posterior capsuloligamentous complex is thinner and more compliant than its anterior counterpart, making it uniquely susceptible to stretch and avulsion under specific loading conditions.
The inferior glenohumeral ligament (IGHL) complex is the primary static stabilizer of the shoulder, functioning much like a hammock suspending the humeral head. It consists of an anterior band, an axillary pouch, and a posterior band. The posterior band of the IGHL originates from the posterior lower quadrant of the glenoid labrum (approximately the 7 o'clock to 9 o'clock position in a right shoulder) and inserts onto the posterior aspect of the anatomical neck of the humerus. During internal rotation, flexion, and adduction, the posterior band of the IGHL becomes taut, preventing posterior translation of the humeral head. A PHAGL lesion occurs when this band is traumatically avulsed from the humeral neck, completely disrupting the hammock mechanism and allowing uninhibited posterior subluxation or dislocation. The avulsion typically occurs at the transition zone between the capsule and the humeral articular cartilage, often retracting medially and inferiorly, which obscures visualization during standard arthroscopy.
The biomechanics of the Hill-Sachs lesion are best understood through the paradigm of the "glenoid track," a concept brilliantly elucidated by Yamamoto and Itoi. The glenoid track is the contact zone on the posterior articular surface of the humeral head that articulates with the glenoid during maximum abduction and external rotation. Its width is calculated as 83% of the intact anterior-to-posterior width of the glenoid, minus the width of any anterior glenoid bone loss. If a Hill-Sachs lesion remains within the boundaries of this track (an "on-track" lesion), the articular cartilage of the humeral head maintains contact with the glenoid rim, and the shoulder remains stable.
Conversely, if the medial margin of the Hill-Sachs lesion extends beyond the medial margin of the glenoid track (an "off-track" lesion), the defect will engage the anterior glenoid rim, leading to a catastrophic loss of the fulcrum and subsequent dislocation. The arthroscopic remplissage directly addresses an off-track lesion by tenodesing the infraspinatus and posterior capsule into the defect. This non-anatomical but biomechanically sound procedure effectively "fills" the defect, preventing the anterior glenoid rim from dropping into the impaction fracture. Furthermore, it acts as a dynamic posterior tether, slightly restricting extreme external rotation and preventing the humeral head from translating anteriorly enough to engage the defect.
Exhaustive Indications and Contraindications
The decision-making algorithm for treating posterior instability and engaging Hill-Sachs lesions requires a meticulous analysis of the patient's physiological age, activity demands, degree of capsular laxity, and precise quantification of bipolar bone loss. Surgical intervention is not a one-size-fits-all endeavor; inappropriate patient selection is the leading cause of recurrent instability or unacceptable postoperative stiffness.
For isolated posterior instability, non-operative management (focused on periscapular and posterior deltoid strengthening) is often the first line of treatment, particularly for atraumatic or voluntary subluxators. However, a documented PHAGL lesion represents a structural failure of the primary static stabilizer that rarely heals conservatively due to the continuous synovial fluid bathing the avulsed footprint. Therefore, the presence of a symptomatic PHAGL lesion in an active patient with recurrent posterior instability is an absolute indication for surgical repair.
The indications for an arthroscopic remplissage are intimately tied to the precise calculation of bipolar bone loss. Remplissage is indicated for patients with recurrent anterior instability who possess an engaging (off-track) Hill-Sachs lesion in the setting of subcritical anterior glenoid bone loss (typically defined as less than 15% to 20% of the glenoid width). It is highly effective as an adjunct to an arthroscopic anterior Bankart repair. However, if anterior glenoid bone loss exceeds the critical threshold of 20% to 25%, an isolated soft-tissue repair with remplissage is biomechanically insufficient. In these scenarios of critical bone loss, a bone-block augmentation procedure, such as a Latarjet or distal tibial allograft, is absolutely contraindicated for isolated remplissage and mandates structural glenoid reconstruction.
| Clinical Scenario | Primary Indication | Contraindications | Preferred Surgical Intervention |
|---|---|---|---|
| Symptomatic PHAGL Lesion | Recurrent posterior instability, failed conservative therapy, positive J-sign on MRI. | Voluntary instability without structural lesion, advanced glenohumeral osteoarthritis. | Arthroscopic Posterior Capsular Repair (PHAGL Repair) to humeral neck. |
| Off-Track Hill-Sachs (<15% Glenoid Bone Loss) | Recurrent anterior instability, engaging defect on dynamic arthroscopy, subcritical glenoid bone loss. | Critical glenoid bone loss (>20%), overhead throwing athletes (due to ER loss). | Arthroscopic Anterior Bankart Repair WITH Remplissage. |
| Off-Track Hill-Sachs (>20% Glenoid Bone Loss) | Critical anterior glenoid bone loss, massive Hill-Sachs lesion, revision instability surgery. | Inability to comply with complex rehab, active joint infection. | Open or Arthroscopic Latarjet / Anterior Bone Block Augmentation. |
| Massive Hill-Sachs (>30% Articular Surface) | Severe humeral head impaction with intact or reconstructed glenoid. | Subcritical lesions amenable to remplissage, poor bone stock. | Humeral Head Osteoarticular Allograft or Arthroplasty (if older). |
Pre-Operative Planning, Templating, and Patient Positioning
Preoperative planning begins with a rigorous clinical examination. Patients with posterior instability often present with a positive Jerk test, Kim test, and posterior apprehension in the flexed, adducted, and internally rotated position. For anterior instability with a suspected engaging Hill-Sachs lesion, apprehension is typically maximal in abduction and external rotation. The surgeon must carefully assess generalized ligamentous laxity (Beighton score) to differentiate between traumatic structural lesions and multidirectional instability.
High-quality imaging is paramount. Standard radiographs must include a true anteroposterior (Grashey) view, a scapular Y view, and an axillary lateral view. A Stryker notch view is particularly useful for visualizing the posterolateral humeral head defect. However, three-dimensional computed tomography (3D-CT) with digital subtraction of the humeral head is the gold standard for quantifying glenoid bone loss. The en face view of the glenoid allows the surgeon to calculate bone loss using the "best-fit circle" or Pico method. Magnetic Resonance Arthrography (MRA) in the ABER (abduction and external rotation) position is highly sensitive for detecting capsulolabral pathology. A PHAGL lesion classically demonstrates the "J-sign" on axial and coronal MRA, where contrast extravasates down the humeral neck posteriorly, indicating a breach in the capsular insertion.
Patient positioning in the operating room is a critical determinant of surgical success, particularly for posterior and inferior capsular work. While some surgeons prefer the beach chair position, the lateral decubitus position is vastly superior for posterior shoulder arthroscopy because it provides unparalleled visualization and allows for precise control of capsular tension.
The patient is placed in the lateral decubitus position and secured with a vacuum beanbag and a kidney rest. Absolute torso stability is essential to prevent shifting during the procedure. The operative arm is suspended using a commercially available traction device (e.g., STAR sleeve). For an isolated PHAGL repair, place the arm in 60 degrees of abduction and 20 degrees of forward flexion, applying 10 to 12 lbs of longitudinal traction. This specific vector opens the posterior glenohumeral joint space and places the posterior capsule under appropriate tension for anatomical repair. Crucially, the surgeon must avoid excessive internal rotation during traction, as this can artificially obliterate the posterior joint space and make visualization of the PHAGL footprint exceedingly difficult. For a remplissage procedure, the patient should be tilted posteriorly approximately 30 degrees to allow superior access to the posterior shoulder, with the arm suspended in 30 degrees of abduction and 15 degrees of forward flexion with 15 lbs of distal traction.
Step-by-Step Surgical Approach and Fixation Technique
Portal Strategy and Diagnostic Arthroscopy
A meticulous portal strategy is the foundation of complex shoulder arthroscopy. A standard posterior viewing portal is established approximately 2 cm inferior and 1 cm medial to the posterolateral acromial angle. An anterosuperior portal is established in the rotator interval, just anterior to the supraspinatus tendon and posterior to the long head of the biceps. This portal serves as the primary viewing portal during posterior repairs. An anteroinferior working portal is placed just superior to the subscapularis tendon.
A thorough diagnostic arthroscopy is performed to evaluate the biceps anchor, rotator cuff, articular surfaces, and the entire capsulolabral circumference. The surgeon must dynamically assess the Hill-Sachs lesion by taking the arm off traction and placing it into abduction and external rotation to confirm engagement with the anterior glenoid rim.
Arthroscopic Repair of Posterior Humeral Avulsion of the Glenohumeral Ligament
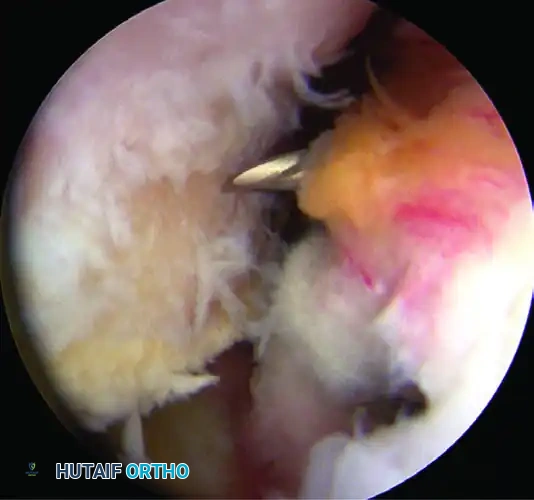
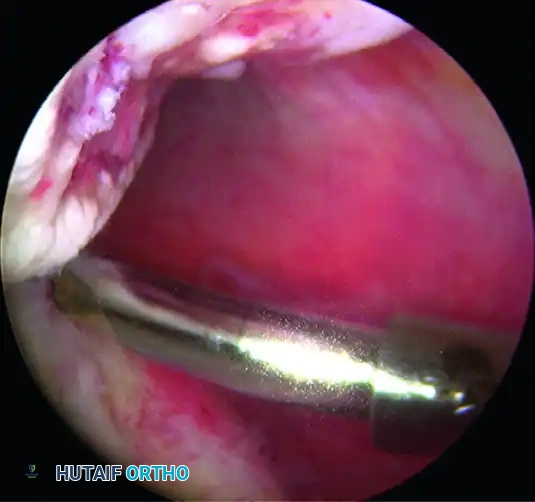
- Footprint Preparation: Once the PHAGL lesion is identified, the camera is moved to the anterosuperior portal. The avulsed posterior capsular edge is debrided to healthy, bleeding tissue using an arthroscopic shaver. An arthroscopic burr is then introduced through the posterior portal to lightly decorticate the anatomical footprint on the posterior humeral neck. This must be done meticulously to create a bleeding bone bed that promotes biological healing without creating a stress riser in the humeral neck.
- Accessory Posterior Portal: Establish a posterior 7-o’clock portal (accessory posterior) using spinal needle localization. This portal is essential for achieving the correct orthogonal angle of approach to the inferior aspect of the humeral neck for anchor placement.
- Inferior Anchor Placement: Introduce a biocomposite or all-suture anchor (typically 3.0mm to 4.75mm) into the inferior aspect of the anatomical attachment on the posterior humeral neck through the 7-o'clock portal.
- Suture Passing: Pass a penetrating device (e.g., a crescent hook or Spectrum) through the torn posterior capsule, approximately 7 mm from its free edge, ensuring a robust bite of the IGHL complex. Retrieve the inferior suture limb and pull it back out through the inferior capsule. The anterosuperior portal is used to maintain tension on the capsule with a grasper during this step.
- Knot Tying: Tie the mattress sutures down snugly, securing the inferior portion of the tear to the humeral neck. Arthroscopic sliding-locking knots (e.g., SMC or Weston knots) followed by alternating half-hitches are recommended to ensure a low-profile, secure construct.
- Superior Anchor Placement and Final Compression: Place a second biocomposite anchor in the more superior aspect of the anatomical capsular attachment. Use the penetrating device to grab the inferior suture of the second anchor, passing it through the capsule, followed by the superior suture, ensuring a 7 mm tissue bridge between passes. Tie this arthroscopic mattress suture while viewing from the superior portal to obtain excellent compression of the capsule to the neck.
The Remplissage Procedure for Engaging Hill-Sachs Lesions
Step 1: Defect Assessment and Portal Optimization
Switch the arthroscope from the posterior portal to the anterosuperior portal, and place a working cannula into the posterior portal. While viewing from the anterosuperior portal, rigorously assess the Hill-Sachs lesion, the extent of glenoid bone loss, and the anterior labral lesion.
Evaluate the posterior portal location. It is correct only if located directly over the Hill-Sachs lesion at an angle permitting the orthogonal placement of two suture anchors. If the trajectory is sub-optimal, establish a dedicated remplissage portal using a spinal needle to ensure a perpendicular approach to the defect.
Step 2: Bed Preparation
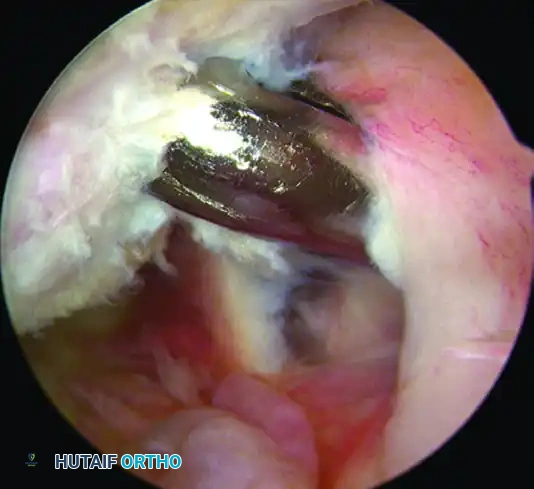
Gently freshen the sclerotic surface of the engaging Hill-Sachs lesion using an arthroscopic burr in reverse mode. Using the burr in reverse removes fibrous tissue and creates a bleeding bone bed without excising critical subchondral bone. Removing too much bone will inadvertently deepen the defect, exacerbating the pathology and potentially leading to a fracture. Freshen the surface of the entire posterior and inferior capsule overlying the defect with a whisker blade to stimulate a healing response.
Step 3: Subdeltoid Cannula Retraction
While maintaining the camera in the anterosuperior portal, carefully withdraw the cannula in the posterior portal out of the posterior capsule and infraspinatus tendon, but not through the deltoid muscle. The mouth of the cannula should now rest in the subdeltoid space, allowing extra-articular manipulation of the sutures.
Step 4: Inferior Anchor Placement
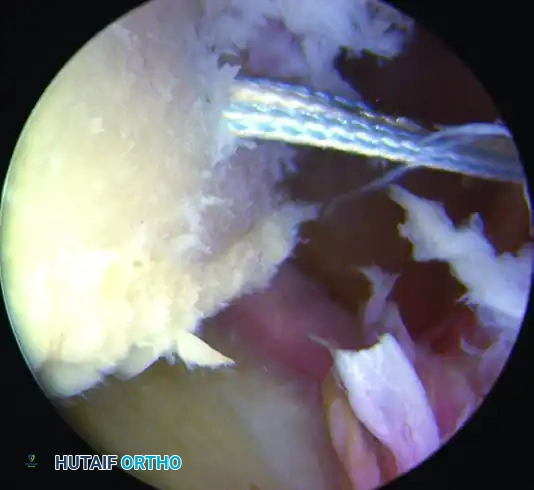
Through the preexisting portal, pass the anchor cannula with its obturator percutaneously through the infraspinatus tendon and posterior capsule. Place the first biocomposite suture anchor into the inferior aspect of the prepared Hill-Sachs lesion.
Pass a penetrating grasper through the tendon and posterior capsule to grasp and pull one suture limb approximately 1 cm inferior to the initial portal entry site, creating a wide mattress configuration.
Step 5: Superior Anchor Placement
Place a second anchor in the superior aspect of the Hill-Sachs lesion. Use the grasper penetrator in the same fashion to pass one suture limb 1 cm superior to the initial portal entry site.
Step 6: Extra-articular Knot Tying
CRITICAL WARNING: The anterior labrum and glenoid neck MUST be prepared, and anterior anchors placed, before proceeding with tying the remplissage. Once the remplissage is tied, posterior capsular tension increases dramatically, severely restricting anterior joint working space.
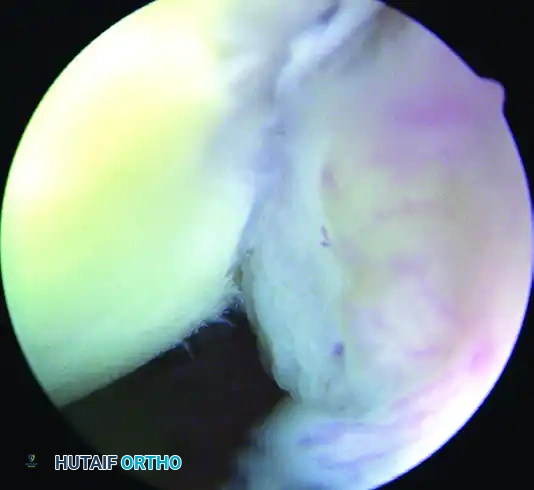
Once anterior anchors are placed, return to the posterior compartment. Tie the inferior suture first. The knots must remain extra-articular, resting in the subdeltoid space on the superficial surface of the infraspinatus. Tie the superior suture to complete the remplissage. These mattress sutures draw the infraspinatus and posterior capsule down into the abraded bony surface, effectively obliterating the defect.
Step 7: Completion of Anterior Repair
With the remplissage tied, return to the anterior compartment to complete the Bankart repair using the previously placed anchors. On completion, check glenohumeral stability dynamically and close the portals.
Complications, Incidence Rates, and Salvage Management
While arthroscopic stabilization procedures are generally safe, complications in the management of complex posterior instability and bipolar bone loss can be debilitating. The surgeon must be acutely aware of the anatomical risks, particularly the proximity of the axillary nerve during inferior capsular work. The axillary nerve runs dangerously close (often within 2 to 3 mm) to the inferior capsule at the 6 o'clock position. Over-penetration of instruments or aggressive thermal ablation in this zone can lead to permanent denervation of the deltoid and teres minor.
A unique and expected consequence of the remplissage procedure is a mild loss of external rotation. Because the posterior capsule and infraspinatus are tethered into the humeral head defect, patients typically experience a 5 to 10-degree loss of external rotation with the arm at the side. While clinically insignificant for the vast majority of patients, this can be career-ending for elite overhead throwing athletes (e.g., baseball pitchers). Therefore, remplissage is generally avoided in this specific demographic.
Recurrent instability remains the most significant complication, often stemming from a failure to recognize critical glenoid bone loss preoperatively. If an isolated remplissage fails in the setting of unrecognized critical bone loss, salvage management requires a transition to an open or arthroscopic Latarjet procedure or a distal tibial allograft reconstruction.
| Complication | Estimated Incidence | Etiology / Risk Factors | Salvage / Management Strategy |
|---|---|---|---|
| Recurrent Instability | 5% - 12% | Unrecognized critical glenoid bone loss (>20%), non-compliance with rehab, new high-energy trauma. | Revision stabilization with bone block augmentation (Latarjet or Iliac Crest Bone Graft). |
| Loss of External Rotation | 80% - 100% (Mild) | Inherent biomechanical tethering of the infraspinatus/capsule into the Hill-Sachs defect. | Aggressive late-phase physical therapy. Rarely requires arthroscopic capsular release. |
| Axillary Nerve Injury | < 1% | Blind suture passing at the 6 o'clock position, aggressive electrocautery near inferior capsule. | Observation and EMG at 3 months. Nerve exploration/grafting if no recovery by 6 months. |
| Hardware Failure / Anchor Pullout | 1% - 3% | Poor bone density in the Hill-Sachs defect, aggressive early mobilization, improper anchor trajectory. | Revision arthroscopy, removal of loose bodies, larger diameter anchors or conversion to open procedure. |
| Chondrolysis | < 0.5% | Intra-articular prominent hardware, excessive thermal energy, continuous intra-articular pain pumps (historical). | Devastating complication. Requires comprehensive cartilage restoration or arthroplasty depending on age. |
Phased Post-Operative Rehabilitation Protocols
Postoperative rehabilitation following complex capsuloligamentous repairs and tenodesis procedures must strike a delicate balance between protecting the biological healing of the repaired tissues and preventing debilitating arthrofibrosis. The protocol must be strictly individualized based on the patient’s specific pathology, tissue quality, and the exact procedures performed. Communication between the operating surgeon and the physical therapist is non-negotiable.
Phase 1: Maximum Protection and Immobilization (Weeks 0-6)
The primary goal of this phase is to protect the surgical repair while allowing for basic hygiene.
* Sling Use: The patient is placed in a rigid Ultrasling. For isolated posterior repairs (PHAGL), the arm is maintained in neutral to slight external rotation (10-15 degrees) to remove all tension from the posterior capsule. For a combined anterior Bankart and Remplissage, the arm is kept in strict neutral rotation.
* Activities of Daily Living (ADLs): Patients are allowed to remove the immobilizer only for controlled, waist-level ADLs (e.g., eating, showering, keyboard use) within 1 to 2 days postoperatively.
* Positional Restrictions: During ADLs, the arm must remain strictly adducted. The patient must not abduct the shoulder and must not externally rotate beyond neutral. Passive range of motion (PROM) is limited to forward elevation up to 90 degrees in the scapular plane.
Phase 2: Controlled Mobilization (Weeks 6-12)
Biological incorporation of the anchors and soft tissue begins, allowing for gradual stress application.
* Range of Motion: The sling is discontinued. Active and active-assisted range of motion is initiated. For PHAGL repairs, stretching into internal rotation must be progressed extremely cautiously. For remplissage patients, stretching into external rotation is advanced slowly, recognizing that a mild permanent deficit is expected and protective.
* Scapular Dyskinesis: Heavy emphasis is placed on closed-chain kinetic exercises and scapular stabilization to prevent compensatory movement patterns.
Phase 3: Strengthening Phase (Weeks 12-16)
- Resistive Strengthening: Isotonic and isokinetic strengthening begins, focusing heavily on the dynamic stabilizers (rotator cuff and periscapular musculature).
- Plyometrics: Light plyometric exercises below shoulder level can be introduced toward the end of this phase for athletic patients.
Phase 4: Return to Play and Advanced Function (Weeks 16 to 6+ Months)
- Work/Sport Specific Training: Progression to overhead activities and sport-specific drills.
- Clearance: No at-risk work activities, heavy overhead lifting, or contact sports are permitted for a minimum of 6 months. Return to collision sports (football, hockey) often requires 7 to 9 months to allow for complete biological incorporation and restoration of neuromuscular proprioception.
Summary of Landmark Literature and Clinical Guidelines
The modern management of posterior instability and engaging Hill-Sachs lesions is built upon a foundation of rigorous biomechanical and clinical research. Orthopedic surgeons must be intimately familiar with the landmark studies that have shaped our current treatment algorithms.
The concept of the "Glenoid Track" was revolutionized by Itoi and Yamamoto (2007), who provided the biomechanical framework for understanding bipolar bone loss. Their cadaveric studies definitively demonstrated how the interaction between glenoid bone loss and the Hill-Sachs lesion dictates engagement, shifting the paradigm away from merely looking at the size of the humeral defect in isolation.
The Arthroscopic Remplissage was first described by Wolf and Purchase in 2008. Their initial case series demonstrated that tenodesis of the infraspinatus and posterior capsule into the Hill-Sachs defect was a safe and highly effective method for preventing recurrent anterior instability without the morbidity associated with open bone grafting procedures. Subsequent long-term follow-up studies by Boileau et al. (2012) confirmed excellent survivorship of the procedure, though they quantified the expected, albeit clinically benign, loss of external rotation.
For cases of critical bone loss where remplissage is contraindicated, Lafosse and Boyle detailed the All-Arthroscopic Latarjet procedure. While demonstrating excellent clinical results and minimal complications in expert hands, the literature universally cautions that this is an exceptionally demanding procedure with a steep learning curve. The consensus guidelines from the American Academy of Orthopaedic Surgeons (AAOS) and the International Society of Arthroscopy, Knee Surgery and Orthopaedic Sports Medicine (ISAKOS) currently recommend that bone block augmentations (open or arthroscopic) be reserved for patients with >20% anterior glenoid bone loss, while the Bankart plus Remplissage remains the gold standard for off-track lesions with subcritical bone loss.
This academic synthesis is based on established protocols from Hutaifortho's Operative Orthopaedics and has been medically reviewed by Prof. Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon. It is designed to assist orthopedic residents, fellows, and practicing surgeons in surgical preparation and board reviews (AAOS, FRCS, Arab Board).
This academic resource was prepared and medically reviewed by Prof. Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon. It is formulated specifically for medical students, orthopedic residents, and surgeons preparing for high-stakes board examinations (AAOS, FRCS Tr & Orth, Arab Board).
