Pediatric Knee Fractures: When is a Long Leg Cast Necessary?
Key Takeaway
For anyone wondering about Pediatric Knee Fractures: When is a Long Leg Cast Necessary?, A long leg cast is an orthopedic immobilization device extending from the upper thigh down to the foot, commonly used to stabilize fractures of the femur, tibia, or knee joint in pediatric patients. It provides crucial support for healing conditions like distal femoral physeal fractures in children, preventing movement across the knee and lower leg to ensure proper recovery and alignment.
Comprehensive Introduction and Patho-Epidemiology
The pediatric knee represents a complex biomechanical nexus where the demands of weight-bearing and locomotion intersect with the vulnerabilities of the immature, growing skeleton. Fractures about the pediatric knee, specifically involving the distal femoral and proximal tibial physes, are high-stakes clinical entities. Because the ligaments in the skeletally immature patient are inherently more resistant to tensile stresses than the cartilaginous physeal plates and adjacent metaphyseal bone, trauma that would typically result in a ligamentous sprain or rupture in an adult often leads to physeal separation or osseous avulsion in a child. Understanding the patho-epidemiology of these injuries is paramount for the orthopedic surgeon, as mismanagement can lead to devastating long-term consequences, including severe angular deformities, profound leg-length discrepancies, and irreversible neurovascular compromise.
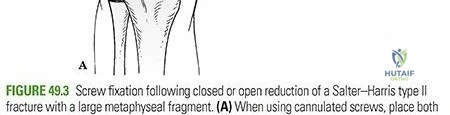
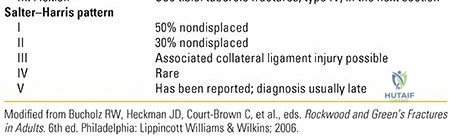
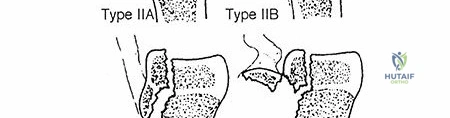
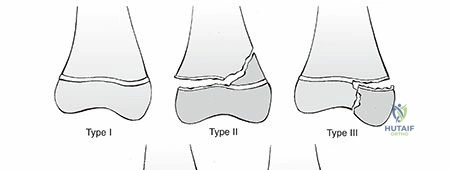
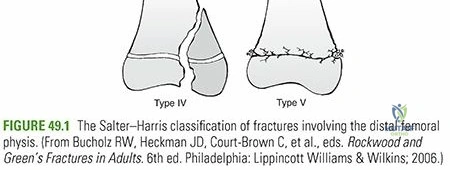
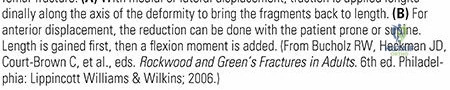
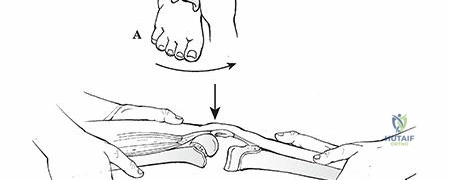
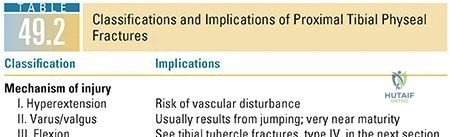
Distal femoral physeal fractures are the most commonly encountered physeal injuries around the knee, yet they remain relatively rare in the broader context of pediatric trauma. They comprise approximately 1% to 6% of all physeal injuries and represent less than 1% of all fractures in children. However, they account for a highly significant 12% to 18% of all pediatric femur fractures. The typical demographic profile for these injuries skews heavily toward adolescents, with males being affected significantly more often than females. The vast majority of these injuries—roughly two-thirds—are classified as Salter–Harris type II fractures. The mechanism of injury is frequently high-energy direct trauma, such as vehicular collisions or severe athletic trauma. For instance, a classic presentation involves a lateral blow to the knee while the foot is firmly planted in a cleated shoe, a scenario ubiquitous in American football and rugby. Indirect injuries, driven by extreme varus/valgus or hyperextension/hyperflexion forces, result in simultaneous compression on one aspect of the physis and distraction on the opposite side, initiating a tear on the tension side that propagates through the physis and exits through the metaphysis.
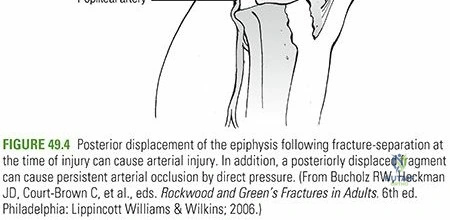
In stark contrast, proximal tibial physeal fractures are exceedingly rare, comprising a mere 0.6% to 0.8% of all physeal injuries. The average age of incidence is approximately 14 years, again predominantly affecting adolescent males. The relative rarity of proximal tibial physeal fractures is attributed to the robust anatomical protection afforded to this region. The proximal tibial physis is shielded laterally by the proximal fibula and the robust tibiofibular syndesmotic ligaments, and anteriorly by the expansive insertion of the patellar tendon onto the tibial tubercle. Furthermore, the undulating, interlocking topography of the proximal tibial physis provides inherent resistance to shear forces. However, when these fractures do occur, they are frequently associated with severe hyperextension forces and carry a notoriously high risk of popliteal artery injury and acute compartment syndrome.
Beyond high-energy athletic and vehicular trauma, the orthopedic surgeon must maintain a high index of suspicion for non-accidental trauma and pathologic fractures. In infants and non-ambulatory children, a distal femoral physeal separation should immediately raise the clinical suspicion of child abuse, prompting a comprehensive skeletal survey and pediatric protective services evaluation. Birth injuries, particularly those secondary to breech presentations or in patients with underlying neuromuscular conditions such as arthrogryposis multiplex congenita, can also result in iatrogenic physeal separations during delivery. Furthermore, minimal trauma can precipitate a fracture in conditions that cause generalized weakening of the physeal architecture, including acute hematogenous osteomyelitis, leukemia, rickets, and myelodysplasia. Recognizing the underlying patho-epidemiology is the first critical step in determining the appropriate treatment trajectory, particularly when deciding if a long leg cast will suffice or if operative intervention is mandated.
Detailed Surgical Anatomy and Biomechanics
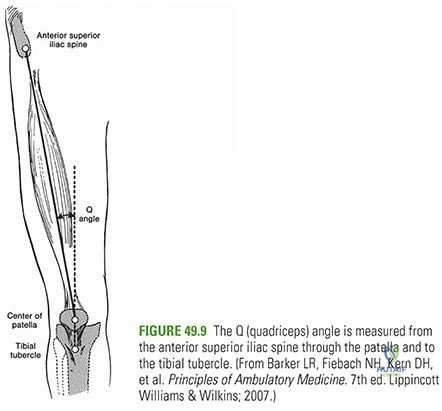
The knee is a complex ginglymoid (hinge) joint that fundamentally consists of three distinct but biomechanically linked articulations: the patellofemoral, tibiofemoral, and proximal tibiofibular joints. Under normal cyclic loading conditions, the knee joint is subjected to immense forces, experiencing up to five times the body weight with every single step during normal ambulation, and significantly higher multiples during athletic activities like jumping and cutting. The normal functional range of motion extends from approximately 10 degrees of hyperextension to 140 degrees of flexion. Crucially, the knee is not a simple uniaxial hinge; it accommodates 8 to 12 degrees of internal and external rotation through its flexion-extension arc, a biomechanical necessity dictated by the "screw-home" mechanism. Both dynamic and static stability are conferred predominantly by an intricate envelope of soft tissues—encompassing the cruciate and collateral ligaments, the musculotendinous units, and the menisci—working in concert with the osseous topography of the femoral condyles and tibial plateaus.
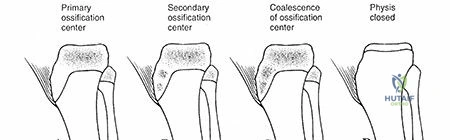
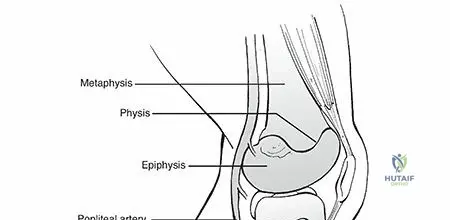
Understanding the chronologic appearance and closure of the secondary ossification centers is critical for accurate radiographic interpretation and surgical planning. There are three primary physeal plates around the knee with secondary ossification centers. The distal femoral ossification center is typically present at birth, appearing around the 39th fetal week, and serves as a reliable radiological marker for fetal maturity. The proximal tibial ossification center appears shortly thereafter, typically by 2 months of age. The tibial tubercle, which develops as a traction apophysis, begins to ossify much later, around 9 years of age. The patella, functioning as the largest sesamoid bone in the body, develops its own ossification center between 3 and 5 years of age. Physeal closure follows a predictable sequence but varies slightly by sex. The tibial tubercle physis closes between 15 and 17 years of age, fusing proximally to distally. The distal femoral and proximal tibial physes are among the last to close in the body, typically fusing between 16 and 19 years of age.
The distal femoral epiphysis is the largest and fastest-growing physis in the human body. Together, the distal femoral and proximal tibial physes are the engines of lower extremity longitudinal growth. The distal femur contributes approximately 9 mm of length per year (accounting for 70% of the femur's growth and 37% of the entire lower extremity's growth), while the proximal tibia contributes approximately 6 mm per year (accounting for 55% of the tibia's growth and 28% of the lower extremity's growth). Combined, these two growth plates are responsible for a staggering two-thirds of the total longitudinal growth of the lower limb. This immense growth potential is a double-edged sword: while it allows for substantial remodeling of fractures in the sagittal plane, any injury that disrupts the germinal layers of these physes—such as a crushing Salter-Harris V injury or a trans-physeal fracture—carries a profound risk of premature asymmetric or symmetric growth arrest, leading to severe angular deformities or limb length discrepancies.
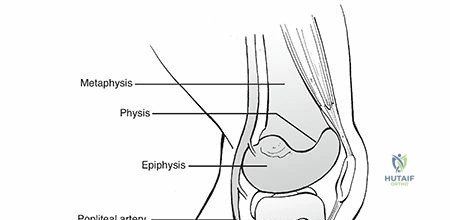
The neurovascular anatomy posterior to the knee joint is of paramount surgical importance. The popliteal artery is firmly tethered both proximally at the adductor hiatus and distally at the soleus arch. As it traverses the posterior aspect of the knee capsule, it gives off the superior and inferior geniculate branches, which form a vital anastomotic network. In the setting of a hyperextension injury to the distal femur, the distal fragment (epiphysis) is displaced anteriorly, driving the sharp, jagged proximal metaphyseal spike directly posteriorly into the popliteal fossa. This metaphyseal spike can easily lacerate, contuse, or stretch the tethered popliteal artery, leading to catastrophic limb ischemia. Similarly, the sciatic nerve bifurcates into the tibial and common peroneal nerves at the level of the distal femur. The common peroneal nerve is particularly vulnerable to traction injuries during severe varus stress or secondary to massive anterior/medial displacement of the epiphysis.
Exhaustive Indications and Contraindications
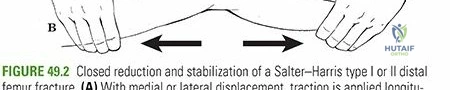
The decision algorithm for managing pediatric knee fractures centers around restoring anatomic joint congruity, achieving absolute mechanical stability, and minimizing iatrogenic trauma to the physis. The fundamental question of "When is a long leg cast necessary?" is answered by evaluating the fracture pattern, the degree of displacement, and the inherent stability of the joint post-reduction. Non-operative management with closed reduction and long leg casting is strictly indicated for non-displaced Salter-Harris type I and II fractures of the distal femur and proximal tibia. Furthermore, displaced Salter-Harris I and II fractures that can be anatomically reduced closed and demonstrate robust stability through a full arc of motion under fluoroscopic stress are excellent candidates for cast immobilization. The intact periosteal hinge, typically located on the compression side of the injury, must be utilized to maintain the reduction via a meticulously molded cast.


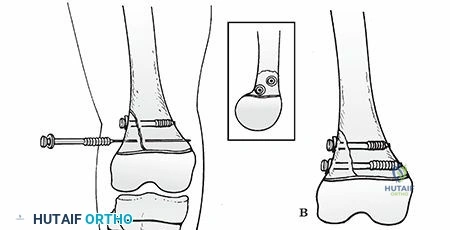
Operative intervention, conversely, is mandated when closed reduction fails to achieve or maintain acceptable alignment. Irreducible Salter-Harris type II fractures are a classic indication for open reduction. The irreducibility is almost invariably caused by the interposition of torn periosteum, muscle tissue, or the neurovascular bundle into the fracture site. Unstable reductions, where the fracture easily displaces upon release of manual traction or during the application of the cast, also necessitate surgical fixation. Furthermore, all Salter-Harris type III and type IV fractures are absolute indications for precise anatomic reduction and internal fixation. Because these fracture patterns traverse the articular surface, any residual step-off or gap will lead to early-onset post-traumatic osteoarthritis. Joint congruity must be restored flawlessly, and the fixation must be rigid enough to allow for early mobilization to prevent debilitating knee stiffness.
Contraindications to isolated long leg casting are critical to recognize to avoid devastating complications. The presence of a vascular injury, suspected or confirmed, is an absolute contraindication to closed management without surgical exploration. A cool, pulseless foot mandates immediate reduction; if perfusion is not instantly restored, emergent vascular exploration is required. Similarly, evolving compartment syndrome, particularly common with proximal tibial physeal fractures, precludes the use of a circumferential cast. Polytraumatized patients with "floating knee" injuries (ipsilateral femoral and tibial shaft fractures) or multiple system injuries require rigid internal or external fixation to facilitate nursing care, pulmonary toilet, and early mobilization.
Indications and Contraindications Table
| Treatment Modality | Absolute Indications | Relative Indications | Absolute Contraindications |
|---|---|---|---|
| Long Leg Cast (Non-Operative) | - Non-displaced SH I & II fractures - Stable, concentrically reduced SH I & II fractures - Patient with prohibitively high surgical risk |
- Minimally displaced SH III fractures (<2mm step-off) in very young children (controversial) | - Vascular compromise/ischemia - Evolving compartment syndrome - Open fractures - Irreducible fractures (soft tissue interposition) |
| Open Reduction Internal Fixation (ORIF) | - All displaced SH III & IV fractures - Irreducible SH I & II fractures - Open fractures requiring debridement - Concomitant vascular injury requiring repair |
- Unstable SH I & II fractures post-closed reduction - "Floating knee" polytrauma scenarios - Severe ipsilateral soft tissue injury precluding casting |
- Active, untreated local infection (relative to definitive internal hardware) - Medically unstable patient (damage control orthopedics preferred) |

Pre-Operative Planning, Templating, and Patient Positioning
The clinical evaluation of a patient with a suspected pediatric knee fracture must be exhaustive and systematic. Patients typically present with an absolute inability to bear weight on the injured extremity. However, it is crucial to note that patients with non-displaced physeal injuries from low-energy mechanisms may still ambulate, albeit with a pronounced antalgic gait. Older children and adolescents frequently report hearing or feeling a distinct "pop" at the moment of impact, accompanied by a rapid-onset knee effusion (hemarthrosis) and diffuse soft tissue swelling. This clinical picture is notoriously easy to confuse with an acute anterior cruciate ligament (ACL) or meniscal tear. The knee is typically held in a flexed position due to profound hamstring spasm. Gross shortening or angular deformity may be present, but its absence does not rule out a severe injury that has spontaneously reduced. A meticulous, documented neurovascular assessment is the single most critical step in the primary survey, given the high risk of traction injury, laceration, or compression of the popliteal vessels and peroneal nerve. Point tenderness meticulously localized over the physis—palpated at the level of the adductor tubercle and the superior pole of the patella—is the hallmark sign of a physeal injury.
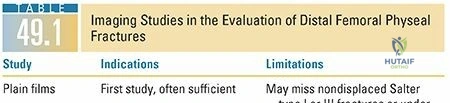
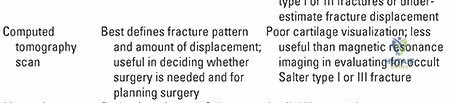
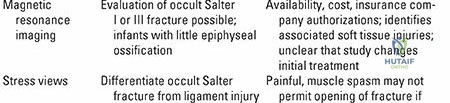
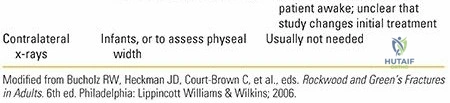
Standard radiographic evaluation mandates high-quality, orthogonal Anteroposterior (AP), lateral, and oblique views of the affected knee. The physeal line in a skeletally immature patient should appear as a radiolucent band approximately 3 to 5 mm thick until the onset of adolescence. Any widening, asymmetry, or irregularity of this line is highly suspicious for a non-displaced Salter-Harris I injury. If the diagnosis remains equivocal, radiographs of the contralateral uninjured lower extremity should be obtained for direct comparison. In cases where the clinical examination strongly suggests a
Clinical & Radiographic Imaging Archive