
Comprehensive Introduction and Patho-Epidemiology
Pediatric femoral shaft and knee fractures represent a complex and highly nuanced domain within pediatric orthopedic traumatology. These injuries require the treating orthopedic surgeon to possess a profound understanding of skeletal growth, biomechanics, and age-specific treatment algorithms. Femoral shaft fractures account for approximately 1.6% of all fractures in the pediatric population. Despite this relatively low overall incidence, they are a significant source of morbidity, often requiring hospitalization, specialized immobilization, or surgical intervention. The demographic distribution demonstrates a strong male predilection, with boys being affected more commonly than girls at a ratio of 2.6:1. Furthermore, there is a well-documented seasonal variation, with a markedly higher incidence of these fractures occurring during the summer months when children are engaged in higher-risk outdoor activities.
The epidemiologic profile of pediatric femoral shaft fractures exhibits a classic bimodal distribution, which is deeply intertwined with both the developmental stages of the child and the evolving biomechanical properties of the maturing femur. The first peak in incidence occurs in early childhood, specifically between the ages of 2 and 4 years. During this stage, the immature woven bone is highly susceptible to low-energy torsional and bending forces sustained during normal play or minor trauma. The second peak occurs in mid-to-late adolescence. By this stage, the femur has undergone significant remodeling, requiring high-energy mechanisms, such as motor vehicle collisions or high-impact athletic trauma, to cause mechanical failure.
Mechanism of injury is intrinsically linked to the age of the patient and must be scrutinized meticulously, particularly in the very young. Direct trauma, including motor vehicle accidents, pedestrian-versus-auto injuries, and falls, represents a large portion of these injuries. However, in children younger than walking age (typically under 12 months), up to 80% of femoral shaft fractures are the result of non-accidental trauma (child abuse). This alarming statistic necessitates a comprehensive child protection evaluation, including a skeletal survey and ophthalmologic examination, for any infant presenting with a femur fracture. As the child reaches toddlerhood, the incidence of abuse as the primary etiology decreases to approximately 30%. Conversely, in the adolescent population, greater than 90% of femoral fractures are the direct result of high-energy motor vehicle or motorcycle accidents.
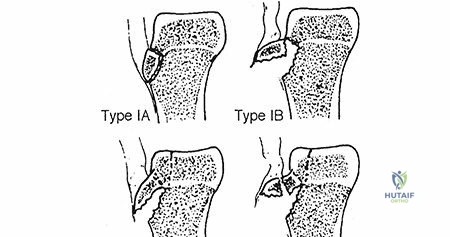
Indirect trauma, primarily rotational injury, typically results in spiral or oblique fracture patterns and is often seen in toddlers whose foot becomes planted while the body twists. Pathologic fractures must also be considered in the differential diagnosis. Conditions such as osteogenesis imperfecta, nonossifying fibromas, unicameral bone cysts, aneurysmal bone cysts, and malignant tumors can compromise the structural integrity of the femur. Furthermore, systemic neuromuscular conditions, such as severe myelomeningocele or cerebral palsy, often result in profound generalized osteopenia, predisposing these vulnerable patients to fractures from seemingly trivial trauma or during routine physical therapy and diaper changes.
Detailed Surgical Anatomy and Biomechanics
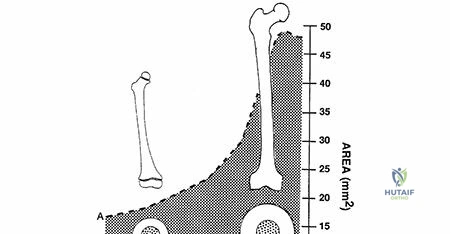
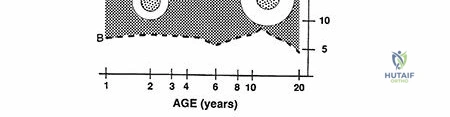
The structural evolution of the pediatric femur is a marvel of biomechanical adaptation. During early childhood, the femur undergoes continuous remodeling, transitioning from primarily weaker, highly cellular woven bone to highly organized, stronger lamellar bone. Up to the age of 16 years, there is a geometric increase in both the femoral shaft diameter and the relative cortical thickness. This specific geometric expansion results in a markedly increased area moment of inertia, which exponentially increases the bone's resistance to bending and torsional stresses. This biomechanical maturation perfectly explains the bimodal distribution of injury patterns: younger patients experience mechanical failure under low-load conditions reached in normal play, whereas adolescents require massive, high-energy trauma to reach the stresses necessary to fracture the mature lamellar cortex.
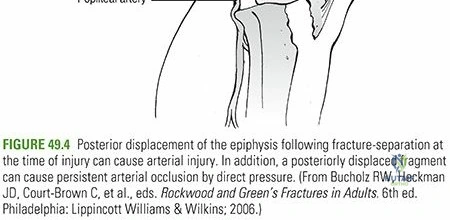
The vascular anatomy of the pediatric proximal femur is of paramount importance to the orthopedic surgeon, particularly when considering intramedullary fixation. The primary blood supply to the developing femoral head is derived from the medial femoral circumflex artery, which gives rise to the lateral ascending cervical vessels. These delicate vessels cross the capsule at the level of the trochanteric notch and traverse the posterosuperior aspect of the femoral neck. Antegrade intramedullary nailing utilizing a piriformis fossa entry point places these critical vessels at extreme risk, either through direct iatrogenic disruption or secondary to intracapsular hematoma and elevated pressure. Consequently, the piriformis starting point is strictly contraindicated in skeletally immature patients due to the unacceptable risk of devastating avascular necrosis (AVN) of the femoral head.
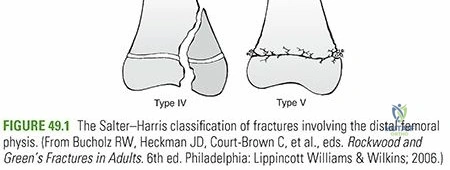
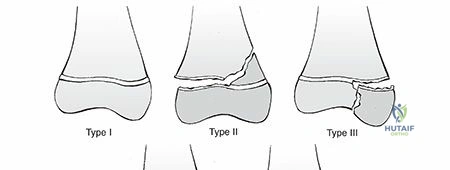
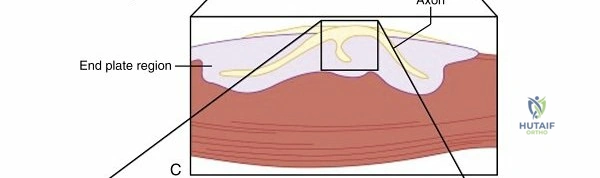
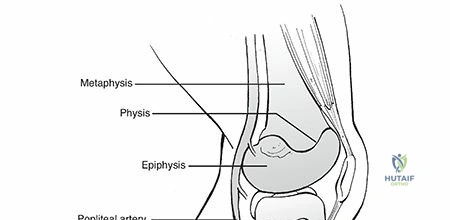
Distally, the pediatric knee functions as a complex ginglymoid (hinge) joint consisting of three distinct articulations: the patellofemoral, tibiofemoral, and tibiofibular joints. Under normal cyclic loading, the knee joint may experience reactive forces up to five times body weight per step. The dynamic and static stability of the knee is conferred predominantly by the robust soft tissues—ligaments, menisci, and musculotendinous units—rather than the bony topography. Because the ligaments in the immature skeleton are significantly more resistant to tensile stresses than the adjacent physeal plates and metaphyseal bone, trauma that would typically cause a ligamentous sprain or rupture in an adult frequently leads to physeal separations and avulsion fractures in the child.
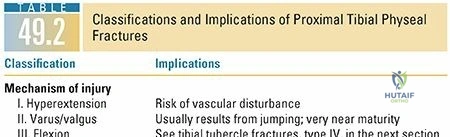
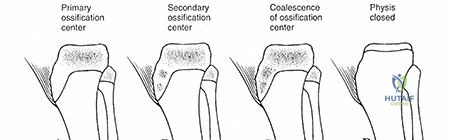
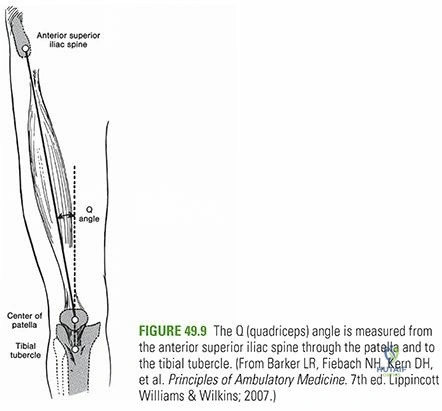
The growth centers around the knee are critical drivers of lower extremity alignment and length. There are three primary physeal plates with secondary ossification centers in this region. The distal femoral ossification center appears by the 39th fetal week and is the largest and fastest-growing physis in the human body, contributing approximately 9 mm of longitudinal growth per year (roughly 70% of the femur's length and 37% of the entire lower extremity's length). It typically closes between 16 and 19 years of age. The proximal tibial ossification center appears by 2 months of age and provides roughly 6 mm of growth per year, closing similarly between 16 and 19 years. The tibial tubercle apophysis, the insertion site of the patellar tendon, ossifies around 9 years of age and closes between 15 and 17 years. The patella itself is the largest sesamoid bone in the body, with its ossification center appearing between 3 and 5 years of age. The distal femoral physis lacks inherent ligamentous protection, as the collateral ligaments insert onto the epiphysis, making it highly susceptible to varus/valgus and hyperextension shear forces.
Exhaustive Indications and Contraindications
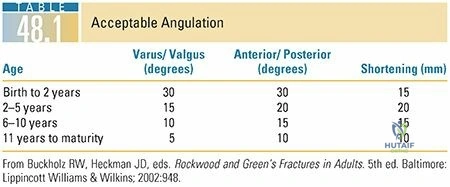
Surgical decision-making for pediatric femoral shaft fractures is heavily dictated by a combination of the patient's chronological age, physiological maturity, body weight, fracture pattern, and the mechanism of injury. A rigid, one-size-fits-all approach is inappropriate; rather, the surgeon must employ a highly individualized algorithm. For infants under 6 months of age, non-operative management with a Pavlik harness or a rigid posterior splint is almost universally indicated. In this age group, the profound remodeling potential of the woven bone allows for acceptance of significant angulation and overriding. Traction and immediate spica casting are rarely necessary and can complicate routine infant care and hygiene.
For children aged 6 months to 4 years, early single-leg or one-and-a-half spica casting is the gold standard, utilized in greater than 95% of cases. Immediate spica casting is indicated for isolated, closed fractures with acceptable initial shortening (less than 2-3 cm). If the fracture is highly unstable and acceptable length and alignment cannot be maintained, a brief period of skeletal traction—utilizing a distal femoral pin placed carefully proximal to the distal femoral physis—may be required prior to casting. External fixation in this toddler age group is generally reserved as a salvage procedure or for severe polytrauma, massive open fractures, or extensive burn injuries where soft tissue access is mandatory.
In the school-aged child (4 to 12 years), the treatment paradigm shifts significantly toward operative intervention. Flexible (elastic) intramedullary nailing, placed in a retrograde fashion, is the workhorse technique for length-stable, transverse, or short oblique fractures. However, flexible nails have strict biomechanical limitations and are generally contraindicated in children weighing more than 100 lbs (45 kg) or in those with highly comminuted, length-unstable fracture patterns (e.g., long spiral fractures or butterfly fragments). In these heavier children or complex patterns, the elastic nails lack the rigidity to prevent progressive shortening and varus collapse. For such cases, submuscular bridge plating or, in older children approaching maturity, rigid lateral-entry intramedullary nailing becomes the indicated treatment.
| Treatment Modality | Primary Indications | Absolute/Relative Contraindications |
|---|---|---|
| Pavlik Harness / Splint | Infants < 6 months, low-energy isolated fractures. | Polytrauma, severe skin abrasions, open fractures. |
| Early Spica Casting | Ages 6 months to 4 years, isolated closed fractures, < 2-3 cm shortening. | Polytrauma, severe head injury, open fractures, massive swelling, body habitus > 99th percentile. |
| Flexible Intramedullary Nails | Ages 4 to 11 years, weight < 100 lbs (45 kg), length-stable patterns (transverse/short oblique). | Weight > 100 lbs, length-unstable patterns (severe comminution/long spiral), narrow medullary canal. |
| Submuscular Bridge Plating | Length-unstable fractures, weight > 100 lbs, proximal/distal metaphyseal extension, polytrauma. | Severe soft tissue compromise over the lateral thigh preventing safe percutaneous insertion. |
| Rigid Intramedullary Nailing | Adolescents (>12 years), weight > 100 lbs, length-unstable patterns. | Open physes (if using piriformis entry - absolute contraindication), narrow canal diameter. |
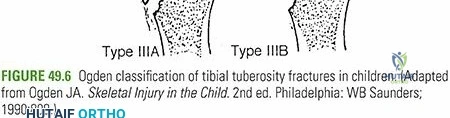
| External Fixation | Damage control orthopedics, severe open fractures (Gustilo IIIB/IIIC), burns, vascular injuries. | Definitive fixation in isolated fractures (due to high refracture and pin tract infection rates). |
Pre-Operative Planning, Templating, and Patient Positioning
The clinical evaluation of a child with a femoral shaft fracture must begin with a systematic Advanced Trauma Life Support (ATLS) protocol, particularly in cases of high-energy trauma. A femoral shaft fracture results in an absolute inability to ambulate, accompanied by extreme pain, gross deformity, and variable thigh swelling. The diagnosis can be challenging in nonambulatory children with severe cerebral palsy or in polytraumatized, intubated patients. The Waddell triad—consisting of a head injury, intra-abdominal or intrathoracic trauma, and a femoral shaft fracture—is strongly associated with pedestrian-versus-motor vehicle accidents and indicates a high-energy mechanism with potential for massive occult volume loss. While hypotension from an isolated pediatric femur fracture is uncommon, a severely tense, swollen thigh may indicate significant hemorrhage into the muscular compartments. True compartment syndrome of the thigh is exceptionally rare due to the large volume of the compartments, but it can occur with severe vascular injury or massive crush mechanisms.

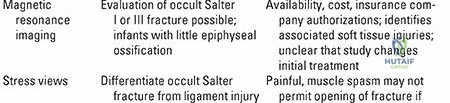
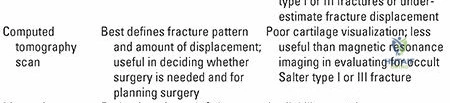
A meticulous neurovascular examination is mandatory. Any splints or compressive bandages placed by emergency medical services in the field must be completely removed to allow for a 360-degree inspection of the soft tissues to definitively rule out an open fracture. The ipsilateral hip and knee must be thoroughly examined. Radiographic evaluation requires high-quality, orthogonal anteroposterior (AP) and lateral views of the entire femur. Critically, the imaging must include dedicated views of the ipsilateral hip and knee to rule out associated injuries, such as basicervical or femoral neck fractures, traumatic hip dislocations, distal femoral physeal separations, or tibial plateau fractures. Advanced imaging, such as MRI or CT, is generally unnecessary for displaced diaphyseal fractures but is invaluable for diagnosing occult, non-displaced stress fractures or evaluating intra-articular knee pathology.

Pre-operative radiographic templating is a critical step that must not be bypassed. When planning for flexible intramedullary nailing, the surgeon must measure the narrowest diameter of the medullary canal on the AP and lateral radiographs. The appropriate nail size is determined by calculating 40% of the narrowest canal diameter; two nails of identical diameter must be used to ensure balanced three-point fixation and prevent asymmetric bending forces that lead to coronal or sagittal malalignment. When templating for submuscular plates, the plate must be long enough to allow for a wide span across the fracture site, ideally achieving a plate-span ratio greater than 3:1 and a screw density of less than 0.5 to promote flexible fixation and secondary bone healing via callus formation.
Patient positioning in the operating room dictates the ease of reduction and the quality of fluoroscopic imaging. For flexible nailing or submuscular plating, the patient is typically positioned supine on a completely radiolucent flat Jackson table. A bump is placed under the ipsilateral hip to correct external rotation. The entire limb is prepped and draped free to allow for intraoperative traction, manipulation, and assessment of clinical alignment. Alternatively, for rigid intramedullary nailing in older adolescents, a fracture table may be utilized with skeletal traction via a distal femoral or proximal tibial pin. The fracture table allows for sustained, controlled traction and facilitates unhindered access to the proximal femur for a lateral trochanteric entry point.
Step-by-Step Surgical Approach and Fixation Technique
Flexible (Elastic) Intramedullary Nailing
Flexible intramedullary nailing (FIN) relies on the biomechanical principle of balanced, symmetrical three-point fixation within the medullary canal. The procedure is performed with the patient supine on a radiolucent table. Two appropriately sized titanium or stainless steel elastic nails are selected. The entry points are located on the medial and lateral aspects of the distal femoral metaphysis, approximately 2.5 to 3.0 cm proximal to the distal femoral physis to avoid iatrogenic growth arrest. Under fluoroscopic guidance, small longitudinal incisions are made, and the fascia is incised in line with the skin.
An awl or drill is used to breach the near cortex at a 45-degree angle to the shaft, angling proximally to facilitate nail insertion. The nails are pre-bent to create a gentle bow; the apex of the bow should rest exactly at the level of the fracture site when fully seated. The lateral nail is typically introduced first and advanced to the fracture site, followed by the medial nail. Closed reduction of the fracture is then performed using manual longitudinal traction and manipulation. Once reduced, the nails are sequentially advanced across the fracture site into the proximal fragment.

The tips of the nails should be driven into the dense cancellous bone of the proximal metaphysis. The medial nail is directed toward the lesser trochanter or femoral neck, while the lateral nail is directed toward the greater trochanter. This divergent placement maximizes rotational stability. The nails are then cut, leaving 1 to 2 cm protruding from the distal cortex to facilitate future removal, but they must be carefully contoured to lie flat against the metaphyseal flare to minimize debilitating soft tissue irritation and painful bursitis.
Submuscular Bridge Plating
For length-unstable fractures or children exceeding the weight limits for FIN, submuscular bridge plating offers robust, rotationally stable fixation without the morbidity of a massive open approach. The patient is positioned supine on a radiolucent table. A 3.5-mm or 4.5-mm locking compression plate (LCP) is selected based on patient size. The plate is pre-contoured to match the gentle anterior bow of the femur. A 3- to 4-cm incision is made either proximally (at the vastus ridge) or distally (lateral epicondyle), depending on the fracture location.
The vastus lateralis is elevated off the lateral intermuscular septum, and an extra-periosteal, submuscular tunnel is created using a blunt Cobb elevator or the plate itself. The plate is slid across the fracture site under fluoroscopic guidance. Reduction is achieved using manual traction, percutaneous reduction forceps, or temporary external fixator pins acting as "joysticks."
Once length, alignment, and rotation are restored, the plate is secured proximally and distally with locking screws inserted through percutaneous stab incisions. The surgeon must ensure a long working length (the distance between the innermost screws) to allow for elastic deformation of the construct, which promotes robust secondary bone healing via endochondral ossification. This technique preserves the fracture hematoma and minimizes periosteal stripping, leading to rapid, reliable union.
Rigid Intramedullary Nailing (Lateral Trochanteric Entry)
In the adolescent patient approaching skeletal maturity, rigid, reamed, locked intramedullary nailing is the gold standard. To completely eliminate the risk of femoral head osteonecrosis associated with the piriformis entry point, a lateral trochanteric or pure greater trochanteric starting point is utilized. The patient is positioned on a fracture table or a flat radiolucent table. A longitudinal incision is made proximal to the greater trochanter.
Under biplanar fluoroscopy, a guide pin is inserted into the lateral aspect of the greater trochanter, ensuring the trajectory remains lateral to the trochanteric fossa to avoid the ascending cervical vasculature. The proximal femur is opened with a rigid reamer, and a ball-tipped guide wire is passed across the reduced fracture site into the distal metaphysis, stopping strictly proximal to the distal femoral physis.

The canal is sequentially reamed to 1.0 to 1.5 mm larger than the anticipated nail diameter. An appropriately sized locked intramedullary nail is then inserted. Proximal and distal interlocking screws are placed to provide absolute rotational and axial stability. This technique allows for immediate weight-bearing and rapid return to function, making it ideal for the high-demand adolescent population.
Complications, Incidence Rates, and Salvage Management
Despite the generally favorable outcomes associated with pediatric femoral shaft fractures, complications can and do occur, requiring astute clinical vigilance and prompt intervention. Leg length discrepancy (LLD) is the most common complication, manifesting either as overgrowth or shortening. Overgrowth of 1.5 to 2.0 cm is a well-documented phenomenon, particularly in children aged 2 to 10 years treated non-operatively with spica casting. This hyperemic response to fracture healing is most pronounced during the initial 2 years post-injury and is most common with distal third fractures. Conversely, initial shortening of up to 2.0 cm is entirely acceptable in younger children due to this anticipated overgrowth. However, for fractures with greater than 3.0 cm of initial shortening, preliminary skeletal traction is mandatory before spica casting. If unacceptable shortening is identified at 6 weeks post-fracture, the surgeon must decide between acute osteoclasis with external fixation distraction or delaying for a definitive limb length equalization procedure (e.g., epiphysiodesis
Clinical & Radiographic Imaging Archive



Detailed Chapters & Topics
Dive deeper into specialized chapters regarding pediatric-femoral-shaft-and-knee-fractures-and-dislocations