Distal Femoral Physeal Fractures: An Intraoperative Masterclass

Key Takeaway
This masterclass guides fellows through the surgical management of distal femoral physeal fractures. We cover comprehensive anatomy, meticulous preoperative planning, and step-by-step intraoperative execution for Salter-Harris types I-IV. Learn critical reduction techniques, precise hardware placement, and strategies for avoiding common pitfalls. Postoperative care and complication management are also thoroughly discussed, ensuring optimal patient outcomes.
Comprehensive Introduction and Patho-Epidemiology
Welcome, colleagues and fellows, to the operating theater. Today, we are undertaking a masterclass on a challenging, highly consequential, and structurally crucial area of pediatric orthopedic trauma: distal femoral physeal fractures. These injuries, while occasionally appearing radiographically straightforward, demand meticulous attention to detail, profound anatomical knowledge, and precise surgical execution. The unique biology and immense growth potential of the distal femoral physis dictate that our margin for error is virtually nonexistent. Our paramount objective today—and in every such case—is to achieve absolute anatomical reduction and rigid, stable fixation while minimizing any further iatrogenic damage to this vital growth plate. In doing so, we strive to preserve future limb length, maintain mechanical axis alignment, and prevent the devastating sequelae of premature physeal closure.
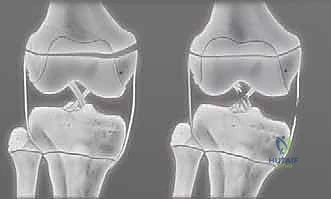
Let us begin by establishing a rigorous definition of the pathology we are addressing. Distal femoral physeal fractures inherently involve the structural failure of the femoral condyles at the level of the physis, separating the epiphysis from the metaphysis. The mechanism of injury typically involves a high-energy shearing, avulsion, or bending force applied to the pediatric knee. This force vector can lead to a catastrophic "shaving off" of the intricate, interlocking undulations of the growth plate. Furthermore, severe "scuffing" of the delicate germinal layer of the physis by the sharp, rigid metaphyseal bone frequently occurs during the initial displacement and, critically, during subsequent forceful or repeated attempted closed reductions of the epiphysis.
Epidemiologically, distal femoral physeal fractures account for approximately 1% to 5% of all physeal injuries and roughly 7% of lower extremity physeal fractures. Despite their relative rarity, they command a disproportionate amount of our clinical attention due to their exceptionally high complication rates. The peak incidence occurs during early adolescence—typically between the ages of 10 and 14 years for males, and slightly earlier for females—coinciding with periods of rapid skeletal growth and increased participation in high-impact collision sports or exposure to motor vehicle trauma. The vulnerability of the distal femoral physis during this developmental window is exacerbated by the relative biomechanical weakness of the hypertrophic zone of the cartilage compared to the robust, mature collateral and cruciate ligaments of the knee joint.
Classification and Prognostication
These fractures are universally categorized utilizing the Salter-Harris classification system, a framework that remains indispensable for guiding our operative strategy, determining the fixation construct, and counseling the family regarding prognosis. The classification is predicated on the anatomical pathway of the fracture line through the epiphysis, physis, and metaphysis.
- Salter-Harris Types I and II: These are extra-articular physeal separations. Type I injuries involve a pure shear through the physis, often presenting radiographically as a widened physis or requiring stress views for diagnosis. Type II, the most common variant, includes the classic Thurston-Holland fragment—a metaphyseal bony wedge attached to the displaced epiphysis. While historically considered to have a more favorable prognosis for continued growth compared to intra-articular variants, distal femoral Salter-Harris II fractures are notoriously deceptive. They are far more prone to growth disturbance (up to 40-50% in some series) compared to equivalent physeal injuries in the distal radius or distal tibia, largely due to the severe initial displacement and the undulating topography of the distal femur.
- Salter-Harris Types III and IV: These represent complex intra-articular fractures. Type III involves a vertical fracture line originating at the articular surface, traversing the epiphysis, and exiting horizontally through the physis. Type IV extends from the articular surface, through the epiphysis, crosses the physis, and exits through the metaphysis. These high-energy, intra-articular injuries carry an exceptionally high risk of both growth derangement (due to cross-physeal cellular communication and subsequent bar formation) and articular incongruity (leading to early-onset post-traumatic osteoarthritis). They universally necessitate open anatomical reduction and rigid internal fixation.

Parents and guardians must be exhaustively counseled preoperatively regarding the stark reality of these injuries. The possibility of growth derangement—manifesting specifically as profound limb shortening or progressive angular deformity (varus, valgus, or recurvatum)—is a direct consequence of the initial traumatic physeal damage, and it may occur regardless of our flawless surgical execution. Our primary objectives are to restore absolute articular congruity when applicable, stabilize the metaphysis to the epiphysis to prevent further shear, and meticulously protect the surviving cellular architecture of the distal femoral growth plate.
Detailed Surgical Anatomy and Biomechanics
Before a scalpel is ever passed, a profound, three-dimensional understanding of the regional anatomy and biomechanics is paramount. The distal femoral physis is not merely another growth plate; it is one of the fastest-growing and most biomechanically significant structures in the developing human skeleton, contributing massively to the overall length and alignment of the lower extremity.
The Distal Femoral Physis and Growth Dynamics
The distal femoral physis is responsible for approximately 70% of the growth of the femur and an astounding 40% of the overall growth of the entire lower extremity. It grows at a remarkable rate of approximately 9 to 10 millimeters per year during peak adolescent velocity. This extraordinary growth rate is precisely why any disruption, cellular death, or bony bar formation here will rapidly become symptomatic, manifesting as a severe leg length discrepancy or a profound angular deformity within months of the injury.
Anatomically, the physis itself is remarkable for its complex, non-planar topography. It features multiple macroscopic undulations, ridges, and mammillary processes that interlock the epiphysis and metaphysis. These structures provide immense inherent stability against physiological shear and torsional forces. However, in the setting of supraphysiological trauma, this very topography becomes a liability. As the epiphysis translates forcefully across the metaphysis, these interlocking ridges act as abrasive surfaces, severely damaging the proliferating and reserve zones of the physis. Damage to these undulations during the initial injury, or iatrogenically during forceful, unrefined reduction maneuvers, will significantly impair future growth.
Ligamentous Attachments and Deforming Forces
The complex ligamentous anatomy of the knee dictates the displacement patterns of these fractures and heavily influences our reduction strategies.
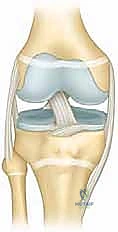
* Collateral Ligaments: The medial collateral ligament (MCL) and lateral collateral ligament (LCL) originate directly from the medial and lateral femoral condyles (the epiphysis), respectively. In a varus or valgus stress injury, the robust collateral ligaments typically remain intact, transferring the destructive energy directly to the weaker physis, resulting in a Salter-Harris I or II fracture. The intact ligaments can be utilized during closed reduction maneuvers by applying tension to guide the epiphyseal fragment back into alignment.
* Cruciate Ligaments: The anterior cruciate ligament (ACL) and posterior cruciate ligament (PCL) originate deep within the intercondylar notch of the distal femoral epiphysis. While not directly involved in the fracture line of extra-articular physeal fractures, their assessment is vital. In severe hyperextension injuries, the strong pull of the cruciates can contribute to the anterior displacement of the distal fragment.
* Gastrocnemius Muscle: The medial and lateral heads of the gastrocnemius originate on the posterior aspect of the distal femoral epiphysis. This muscular attachment acts as a massive deforming force, consistently pulling the distal epiphyseal fragment into apex-posterior angulation (flexion) and posterior translation, complicating reduction and necessitating specific patient positioning.

Neurovascular Structures in the Popliteal Fossa
This is a critical, high-stakes anatomical zone, fellows. The popliteal artery and the common peroneal nerve are in perilous proximity to the distal femur, particularly along its posterior aspect.
- Popliteal Artery: Located deep within the popliteal fossa, the popliteal artery lies immediately posterior to the distal femur. It is firmly tethered proximally at the adductor hiatus and distally at the soleus arch. This rigid tethering makes it exceptionally vulnerable to stretch, intimal tearing, or complete transection in hyperextension injuries where the jagged metaphyseal shaft is driven posteriorly into the popliteal space. Any compromise to this vessel can lead to devastating consequences, including limb loss.
- Peroneal Nerve: The common peroneal nerve courses laterally and distally around the fibular neck, but its more proximal course within the popliteal fossa and its lateral branches are at severe risk. This is particularly true with lateral displacement of the fracture fragments, during forceful reduction of a valgus deformity, or during percutaneous pin placement from a direct lateral approach.
Muscular Intervals for Open Approaches
While percutaneous techniques are favored to minimize soft tissue disruption and preserve the periosteal blood supply, open approaches are mandatory for intra-articular fractures or irreducible extra-articular variants. A deep understanding of muscular intervals is required:
* Medial Approach: Often utilized for medial condyle fractures (Salter-Harris III/IV) or irreducible SH II fractures with medial periosteal interposition. The incision develops the interval between the vastus medialis anteriorly and the adductor magnus or medial hamstrings posteriorly. Care must be taken to protect the superior medial genicular artery.
* Lateral Approach: Typically involves a longitudinal incision developing the plane between the vastus lateralis and the lateral intermuscular septum. This provides excellent exposure to the lateral metaphysis and condyle but requires meticulous retraction to avoid injury to the superior lateral genicular vessels and the peroneal nerve posteriorly.
Exhaustive Indications and Contraindications
Surgical decision-making in distal femoral physeal fractures requires a nuanced balancing of risks: the risk of growth arrest from the injury itself versus the risk of iatrogenic damage from surgical intervention. The following table delineates the standard indications and contraindications for operative management.
| Parameter | Indications for Surgical Intervention (CRPP or ORIF) | Contraindications / Non-Operative Management |
|---|---|---|
| Fracture Displacement | Any displacement > 2mm in any plane (coronal, sagittal, or axial). | Truly non-displaced Salter-Harris I or II fractures (proven on stress views/CT). |
| Articular Congruity | All Salter-Harris Type III and IV fractures (require absolute anatomical reduction). | N/A - Intra-articular fractures are never managed non-operatively if displaced. |
| Reduction Status | Failure to achieve or maintain acceptable alignment via closed reduction. | Stable, anatomical reduction achieved closed and maintainable in a cast (rarely recommended due to loss of reduction risk). |
| Soft Tissue Interposition | Irreducible fractures due to periosteum, muscle, or neurovascular entrapment. | N/A - Entrapment mandates immediate open exploration. |
| Neurovascular Status | Vascular compromise requiring exploration; compartment syndrome requiring fasciotomy. | Severe, life-threatening polytrauma where limb salvage is secondary to damage control resuscitation (relative contraindication). |
| Systemic Factors | Open fractures requiring immediate debridement and stabilization. | Active, untreated local infection (e.g., overlying cellulitis or osteomyelitis) precluding hardware placement. |

Surgical Decision-Making Paradigms
The contemporary orthopedic paradigm has shifted aggressively toward operative stabilization for nearly all displaced distal femoral physeal fractures. Historically, closed reduction and cast immobilization were attempted more frequently. However, the exceedingly high rates of secondary displacement within the cast, coupled with the catastrophic consequences of malunion in a rapidly growing femur, have rendered non-operative management largely obsolete for anything other than strictly non-displaced injuries. Even in cases where a perfect closed reduction is achieved in the emergency department, the deforming forces of the gastrocnemius and adductors often lead to insidious loss of reduction. Therefore, percutaneous pinning or screw fixation is heavily favored to lock the reduction in place, allowing the physis to heal without ongoing shear stress.

Pre-Operative Planning, Templating, and Patient Positioning
Thorough, exhaustive preoperative planning is the absolute cornerstone of a successful surgical outcome. In the pediatric trauma setting, rushing to the operating room without a complete understanding of the fracture morphology is a recipe for disaster.
Preoperative Assessment and Clinical Examination
- Patient History: It is crucial to ascertain the exact direction, magnitude, and mechanism of the injuring force. A hyperextension injury suggests a high risk of popliteal artery injury and posterior metaphyseal displacement. A valgus stress injury suggests a lateral physeal crush with medial tension failure. This history helps predict the displacement pattern and guides the reduction maneuvers.
- Physical Examination:
- Neurovascular Status: This cannot be overstated. Routinely and meticulously assess distal pulses (dorsalis pedis, posterior tibial) utilizing a Doppler if necessary. Assess neural function comprehensively (peroneal nerve: active dorsiflexion, sensation in the first dorsal web space; tibial nerve: active plantarflexion, sensation in the plantar sole). Document these findings meticulously before any intervention.
- Inspection and Palpation: The knee is typically grossly swollen, ecchymotic, and may appear clinically dislocated. Remember, true tibiofemoral knee dislocation is exceedingly uncommon in skeletally immature patients; a severe distal femoral physeal separation is far more likely to mimic a dislocation.

- Compartment Assessment: The high-energy nature of these injuries, combined with massive local hemorrhage, places the patient at significant risk for thigh or calf compartment syndrome. Maintain a high index of suspicion.
Advanced Imaging Studies
Standard plain radiographs are the starting point, but they are rarely sufficient for definitive operative planning in complex cases.
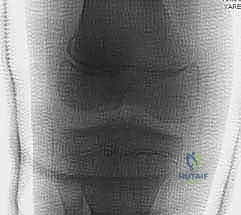
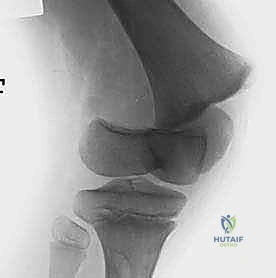
* Plain Radiographs: Standard anteroposterior (AP) and lateral views of the distal femur and knee are essential. These provide a global overview of the fracture pattern, the degree of translation and angulation, and the presence of a Thurston-Holland fragment.
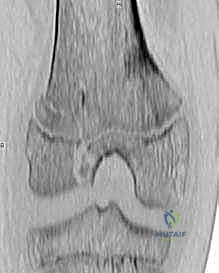
* Computed Tomography (CT): For any suspected Salter-Harris III or IV intra-articular fracture, a CT scan with 3D reconstructions is mandatory. It delineates the exact size, location, and displacement of the articular fragments, allowing the surgeon to plan the precise trajectory of interfragmentary screws to avoid crossing the physis.
* Magnetic Resonance Imaging (MRI): While less commonly used in the acute trauma setting due to logistical constraints, MRI is invaluable for assessing purely cartilaginous injuries in very young patients where the epiphysis is largely unossified, or for evaluating concomitant ligamentous or meniscal pathology.
Patient Positioning and Operating Room Setup
Proper positioning is critical to neutralize deforming forces and facilitate unimpeded fluoroscopic imaging. The patient is placed supine on a fully radiolucent Jackson table or a standard operating table with a radiolucent extension. A bump is frequently placed under the ipsilateral hip to correct natural external rotation.
Crucially, a sterile bump or a radiolucent triangle should be available to place under the distal thigh or proximal tibia. For fractures with apex-posterior angulation (driven by the gastrocnemius), flexing the knee to 60-90 degrees relaxes the gastrocnemius, significantly aiding reduction. The fluoroscopy C-arm must be positioned to allow effortless, orthogonal AP and lateral imaging without moving the violently injured limb. The surgeon should confirm that perfect lateral views of the femoral condyles can be obtained before prepping and draping.
Step-by-Step Surgical Approach and Fixation Technique
The surgical execution must be a symphony of gentle handling, precise imaging, and rigid mechanical stabilization. We will divide our approach based on the necessity for open versus closed techniques.
Closed Reduction and Percutaneous Pinning (CRPP)
For displaced Salter-Harris I and II fractures, CRPP is the gold standard. The reduction maneuver must be deliberate and single-pass if possible. Repeated, forceful grinding of the metaphyseal bone against the physis will invariably cause iatrogenic growth arrest.
1. Neutralization: With the patient under deep general anesthesia and full muscle relaxation, the knee is flexed to 90 degrees to neutralize the gastrocnemius pull.
2. Traction and Translation: Longitudinal traction is applied in the line of the deformity. For the classic anteriorly displaced epiphysis, an anteriorly directed force is applied to the distal femoral shaft while a posteriorly directed force is applied to the femoral condyles.
3. Correction of Angulation: Varus or valgus malalignment is corrected by utilizing the intact collateral ligaments as a tension band.
4. Provisional Fixation: Once fluoroscopy confirms an anatomical reduction on both AP and lateral views, provisional fixation is achieved with smooth Kirschner wires.

Hardware Selection and Placement Strategies
The choice of hardware is dictated by the fracture pattern and the volume of the metaphyseal fragment.
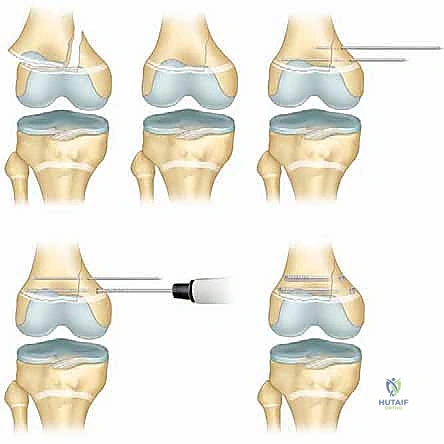
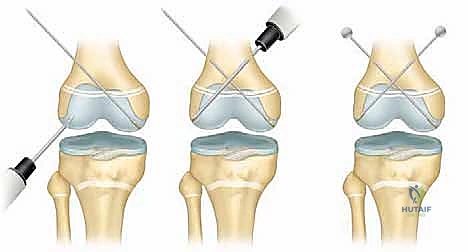
* Crossed Smooth Steinmann Pins: For pure SH I or SH II fractures with a very small Thurston-Holland fragment, crossed smooth pins (typically 2.0mm to 3.2mm depending on patient size) are utilized. These must cross proximal to the fracture line and ideally cross the physis at the most central, vertical angle possible to minimize the cross-sectional area of physeal violation. Avoid the peripheral perichondrial ring of LaCroix, as injury here strongly predisposes to peripheral bar formation.
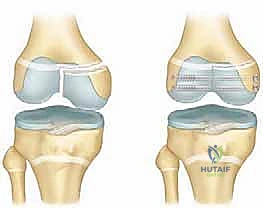
* Cannulated Screws: If a robust Thurston-Holland fragment is present, it is highly preferable to utilize partially threaded cannulated screws (typically 4.0mm or 4.5mm) directed from the metaphyseal fragment into the main metaphyseal shaft, entirely avoiding the physis. This provides rigid interfragmentary compression without violating the growth plate.

Open Reduction and Internal Fixation (ORIF)
Open reduction is absolutely mandated for all displaced Salter-Harris III and IV fractures, and for SH I/II fractures that are irreducible closed due to periosteal entrapment (most commonly the medial periosteum in a valgus injury).
- Approach: Utilize a medial or lateral approach based on the fracture anatomy. For intra-articular fractures, an arthrotomy is performed to directly visualize the articular surface.
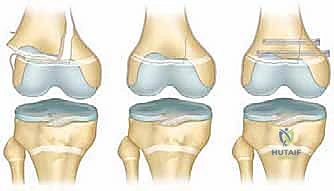
- Debridement: The fracture hematoma is evacuated. In SH II fractures, the entrapped periosteum is carefully extracted from the physeal gap using a Freer elevator. Do not aggressively curette the physis.
- Articular Reduction: For SH III/IV fractures, the articular surface must be reduced perfectly. Even a 1mm step-off is unacceptable and will lead to rapid joint degeneration. The reduction is provisionally held with pointed reduction forceps.
- Epiphyseal Fixation: The epiphyseal fragments are stabilized using partially threaded cannulated screws placed strictly parallel to the physis, entirely within the epiphysis. Fluoroscopy must confirm that these screws do not violate the joint space or the growth plate.
- Metaphyseal Fixation: For SH IV fractures, the metaphyseal component is subsequently stabilized to the main shaft, bridging the physis only if absolutely necessary for stability, and ideally using smooth pins if crossing is unavoidable.
Complications, Incidence Rates, and Salvage Management
The distal femoral physis is unforgiving. Complications are frequent and can be severely debilitating. A comprehensive understanding of these risks is essential for both preoperative counseling and long-term postoperative surveillance.
| Complication | Estimated Incidence | Pathophysiology & Risk Factors | Salvage / Management Strategy |
|---|---|---|---|
| Premature Physeal Arrest | 30% - 50% | Direct crushing of germinal cells; cross-physeal hardware; severe initial displacement. | Resection of osseous bar with interposition graft (if <50% involved); Epiphysiodesis of contralateral limb. |
| Leg Length Discrepancy (LLD) | 20% - 40% | Complete or partial central physeal arrest leading to stunted longitudinal growth. | Shoe lifts (mild); Contralateral epiphysiodesis; Ipsilateral limb lengthening (distal femoral osteotomy/Ilizarov). |
| Angular Deformity | 15% - 30% | Asymmetrical peripheral physeal arrest (e.g., medial arrest leading to genu varum). | Guided growth (8-plates) for remaining growth; Corrective closing/opening wedge osteotomies at skeletal maturity. |
| Loss of Reduction | 5% - 10% | Inadequate fixation; premature weight-bearing; extreme deforming muscle forces. | Immediate revision surgery with more rigid internal fixation (ORIF). |
| Joint Stiffness / Arthrofibrosis | 10% - 20% | Prolonged immobilization; intra-articular scar tissue formation; prominent hardware. | Aggressive physical therapy; Manipulation under anesthesia (MUA); Arthroscopic lysis of adhesions. |
| Neurovascular Injury | 1% - 3% | Popliteal artery tear/thrombosis; Peroneal nerve stretch during extreme displacement. | Immediate vascular surgery consultation/repair; Nerve exploration if no recovery noted clinically or on EMG. |
Growth Arrest and Angular Deformity
The most feared complication is the formation of a physeal bar—a bridge of solid bone crossing the physis, tethering the epiphysis to the metaphysis. If this bar forms centrally, it acts as a tether, leading to a progressive and profound leg length discrepancy. If the bar forms peripherally (e.g., on the medial side following a valgus crush injury), the lateral physis continues to grow, driving the limb into a severe varus deformity.
Surveillance is mandatory. Patients must be followed with serial long-leg alignment radiographs every 6 months for at least 2 years post-injury, or until skeletal maturity. If a bar is identified early and involves less than 40-50% of the physeal cross-sectional area, a bar resection and interposition of fat or Cranioplast may restore growth. If the bar is massive, or if the patient is nearing skeletal maturity, contralateral epiphysiodesis to equalize leg lengths, or corrective osteotomies to realign the mechanical axis, become the primary salvage pathways.



Neurovascular Compromise and Compartment Syndrome
While less common than growth disturbances, neurovascular complications are immediate limb-threatening emergencies. The popliteal artery can be stretched, intimal-torn, or completely transected. If pulses are absent post-reduction, an immediate on-table angiogram or vascular surgery consultation is required. Do not assume vascular spasm. Similarly, the massive swelling associated with these fractures can rapidly evolve into thigh or calf compartment syndrome. Prophylactic fasciotomies are rarely indicated, but a zero-tolerance threshold for clinical signs (pain out of proportion, pain with passive stretch, tense compartments) must be maintained, followed by immediate compartmental pressure monitoring and therapeutic fasciotomy if thresholds are breached.
Phased
