Submuscular Bridge Plating of Pediatric Femoral Shaft Fractures: An Intraoperative Masterclass

Key Takeaway
This masterclass guides you through submuscular bridge plating for pediatric femoral shaft fractures. We cover meticulous preoperative planning, precise patient positioning, and a granular, real-time intraoperative execution. Learn critical anatomical considerations, instrument use, and advanced techniques like "perfect circle" screw placement. We also detail pearls, pitfalls, and comprehensive postoperative care, ensuring optimal outcomes for unstable comminuted or oblique femur fractures in pediatric patients.
Comprehensive Introduction and Patho-Epidemiology
Pediatric femoral shaft fractures represent a significant proportion of major skeletal trauma in children, typically exhibiting a bimodal distribution driven by low-energy falls in toddlers and high-energy mechanisms—such as motor vehicle collisions or sports trauma—in older children and adolescents. Historically, the management of these fractures relied heavily on conservative measures, primarily early spica casting. While casting remains the gold standard for children under the age of five, the paradigm for older children has shifted dramatically toward operative intervention. This evolution is driven by the need to minimize psychological trauma, reduce the burden of prolonged immobilization on families, and mitigate the risks of malunion, joint stiffness, and length discrepancies inherent to non-operative management in heavier, more muscular patients.
Among the operative armamentarium, submuscular bridge plating has emerged as a profoundly elegant and mechanically sound technique. It represents a quantum leap from the traditional open plating methods that demanded extensive periosteal stripping and devascularization of the fracture fragments, which frequently led to delayed union, nonunion, or catastrophic implant failure. By adopting a minimally invasive, biologically respectful approach, submuscular plating adheres to the principles of biologic osteosynthesis. The technique deliberately bypasses the zone of injury, preserving the crucial fracture hematoma and the periosteal blood supply, thereby fostering robust secondary bone healing via endochondral ossification.
The specific niche for submuscular bridge plating lies primarily in length-unstable fracture patterns—such as highly comminuted, long oblique, or spiral fractures—in children aged 6 years to skeletal maturity. In this demographic, elastic stable intramedullary nailing (ESIN) often fails to provide adequate axial or rotational stability, leading to shortening or malrotation. Conversely, rigid trochanteric-entry intramedullary nailing carries a well-documented, albeit low, risk of iatrogenic avascular necrosis (AVN) of the femoral head or proximal femoral valgus deformity due to apophyseal arrest. Submuscular plating elegantly navigates between these extremes, offering the rigid length and rotational control of a plate without the biologic insult of an open approach or the vascular risks of a rigid nail.
This chapter is designed as an exhaustive, intraoperative masterclass for orthopedic surgeons, fellows, and residents. We will meticulously deconstruct the submuscular bridge plating technique, moving far beyond basic principles to explore the nuanced soft-tissue handling, precise fluoroscopic navigation, and advanced biomechanical strategies required to execute this procedure flawlessly. Our objective is to provide a definitive reference that empowers the operating surgeon to tackle complex pediatric femur fractures with confidence, maximizing biologic healing while minimizing iatrogenic complications.
Detailed Surgical Anatomy and Biomechanics
Osteology and Biomechanical Principles
The femoral shaft is a thick, cylindrical cortical tube that acts as the primary weight-bearing strut of the lower extremity. For the purposes of submuscular plating, our anatomical boundaries span from the greater trochanteric apophysis proximally to the flare of the distal femoral metaphysis. Recognizing the natural anterior bow of the femur is critical; while modern plates must be contoured to approximate this curvature, absolute precision is not strictly necessary. The pediatric femur possesses remarkable remodeling potential, and the bone will frequently reduce to the contour of the plate. The primary biomechanical goal is to achieve relative stability, not the absolute stability sought in articular fractures.
Bridge plating functions on the principle of splintage. By securing the plate to the proximal and distal intact bony segments and leaving the comminuted fracture zone untouched, the surgeon creates a flexible construct. This flexibility is heavily dependent on the "working length" of the plate—the distance between the innermost proximal and distal screws. A longer working length decreases the stiffness of the construct, allowing for controlled micromotion at the fracture site. According to Perren’s strain theory, this micromotion stimulates exuberant callus formation. If the construct is too rigid (e.g., screws placed too close to the fracture), the strain may be too low to induce secondary healing, potentially leading to stress shielding, delayed union, or plate fatigue failure.
The choice of implant profoundly influences these biomechanics. A 4.5-mm narrow low-contact dynamic compression plate (LC-DCP) is the workhorse for this procedure. Its scalloped undersurface minimizes periosteal compression, further preserving the cortical blood supply. In osteopenic bone or in highly proximal/distal fractures where cortical purchase is limited, locking compression plates (LCP) act as internal fixators. Locking screws provide angular stability independent of plate-to-bone friction, effectively distributing stress across the entire construct and preventing secondary loss of reduction in mechanically challenging environments.
Muscular Intervals and Soft Tissue Envelopes
Navigating the lateral thigh requires a deep understanding of its fascial and muscular layers to exploit the correct avascular planes. The outermost boundary is the tensor fascia lata (TFL) and its distal continuation, the iliotibial (IT) band. This thick, fibrous structure must be incised to access the deeper muscular compartments. Beneath the IT band lies the vastus lateralis, the largest and most powerful muscle of the quadriceps femoris group. The vastus lateralis originates from the greater trochanter and the lateral lip of the linea aspera, wrapping around the lateral aspect of the femur.
The critical maneuver in submuscular plating is identifying the interval deep to the vastus lateralis. Specifically, the surgeon must dissect beneath the obliquely oriented distal fibers of the vastus lateralis to access the lateral femoral periosteum. This epi-periosteal plane is remarkably avascular and can be developed with minimal blunt dissection. By tunneling the plate within this specific plane, the surgeon lifts the vastus lateralis off the femur without stripping the periosteum or disrupting the muscular perforators that supply the bone.
Proximally, the anatomy becomes more complex due to the insertions of the gluteus medius and minimus on the greater trochanter. When extending the plate proximally, extreme care must be taken to avoid violating the trochanteric apophysis, as iatrogenic injury here can lead to premature physeal closure and subsequent coxa valga or limb length discrepancy. The plate should sit firmly on the lateral cortex, distal to the apophyseal growth plate, securely nestled beneath the vastus lateralis origin.
Neurovascular Topography and At-Risk Structures
The lateral submuscular approach is inherently safe, deliberately avoiding the major neurovascular bundle (femoral artery, vein, and nerve) located in the anterior and medial compartments of the thigh. However, the lateral approach is not entirely devoid of neurovascular considerations. The lateral femoral cutaneous nerve (LFCN) typically courses anteriorly and medially, but significant anatomic variations exist. While rarely encountered in the deep epi-periosteal plane, aggressive proximal dissection or errant percutaneous stab incisions could theoretically put variable branches of the LFCN at risk, leading to painful neuromas or lateral thigh numbness.
The primary vascular structures of concern are the perforating arteries. Arising from the profunda femoris artery, these vessels pierce the adductor magnus and the lateral intermuscular septum to supply the vastus lateralis and the lateral femoral cortex. There are typically three to four perforators distributed along the linea aspera. While the submuscular tunnel is created anterior to the linea aspera, aggressive, sweeping blunt dissection in the mid-shaft can inadvertently avulse these perforators, leading to brisk, difficult-to-control hemorrhage within the muscle belly. Maintaining the tunneling instrument (or the plate itself) strictly on the bone minimizes this risk.
Finally, the distal femoral physis represents a critical "no-go" zone. The distal extent of the plate and the trajectory of the most distal screws must be meticulously planned and fluoroscopically verified to ensure they remain strictly epiphyseal/metaphyseal and do not violate the undulating distal growth plate. Iatrogenic physeal arrest in the distal femur is a devastating complication that can result in profound angular deformity and leg length discrepancy, given that the distal femur contributes approximately 70% of the longitudinal growth of the entire femur.
Exhaustive Indications and Contraindications
Patient selection is the cornerstone of success in submuscular bridge plating. This technique is not a panacea for all pediatric femur fractures but rather a highly specialized tool for specific mechanical and demographic scenarios. The ideal candidate is a child between the ages of 6 and 12 years (or up to skeletal maturity depending on weight and bone size) who has sustained a high-energy, length-unstable fracture. Length instability is defined by fracture morphology: long spiral, long oblique, or highly comminuted patterns where the cortical ends cannot be securely interlocked. In these patterns, elastic nails (TENs) cannot resist the powerful deforming forces of the thigh musculature, leading to telescoping and shortening.
Submuscular plating is also highly advantageous in the polytraumatized pediatric patient. Children with concomitant head injuries, pulmonary contusions, or solid organ injuries require rapid, definitive, and rigid stabilization of long bone fractures to facilitate nursing care, upright positioning, and early mobilization. Furthermore, in patients with spasticity (e.g., cerebral palsy), the intense and unpredictable muscle spasms can easily overpower flexible intramedullary constructs; the rigid construct of a bridge plate provides the necessary mechanical resilience to maintain alignment during the healing phase.
Conversely, there are distinct contraindications. Absolute contraindications include active local infection or severe, highly contaminated open fractures (e.g., Gustilo-Anderson Type III) where placing extensive hardware could precipitate catastrophic osteomyelitis. Relative contraindications include very proximal (subtrochanteric) or very distal (supracondylar) fractures where the remaining bone stock is insufficient to accommodate the requisite number of screws (typically a minimum of three, preferably more) for stable fixation. In such extreme proximal or distal cases, specialized pediatric locking plates or alternative fixation strategies may be required.
| Feature | Indications for Submuscular Plating | Contraindications / Relative Contraindications |
|---|---|---|
| Age / Weight | 6 years to skeletal maturity; > 40-50 kg where TENs fail | < 5 years (spica cast preferred); Adults (IM nail preferred) |
| Fracture Morphology | Comminuted, long oblique, spiral (length-unstable) | Transverse, short oblique (length-stable; TENs preferred) |
| Fracture Location | Diaphyseal, diaphyseal-metaphyseal junction | Extreme subtrochanteric or supracondylar (limited screw purchase) |
| Soft Tissue Status | Closed fractures, Gustilo Type I/II open fractures | Gustilo Type III open fractures with severe contamination |
| Patient Status | Polytrauma, head injury, spastic neuromuscular disease | Active local soft tissue or bone infection |
Pre-Operative Planning, Templating, and Patient Positioning
Implant Selection and Pre-Operative Templating
Meticulous preoperative planning differentiates a smooth, efficient surgery from an intraoperative struggle. The first decision is plate selection. For the vast majority of pediatric femoral shaft fractures, a 4.5-mm narrow LC-DCP provides optimal strength and a favorable biological profile. If the bone is osteopenic, or if the fracture is highly proximal or distal necessitating enhanced angular stability, a 4.5-mm narrow LCP (locking compression plate) is selected. The plate must be long enough to span the entire fracture zone while allowing for adequate fixation proximally and distally. The standard "rule of sixes" applies: aim for a plate long enough to accommodate at least six screw holes proximal to the fracture and six holes distal to it, yielding typical plate lengths of 10 to 16 holes.
Because the plate will be inserted submuscularly, it must be pre-contoured to match the native anatomy of the femur. The femur exhibits a distinct anterior bow and a varus curvature proximally. Using a table plate bender, the surgeon imparts a gentle, sweeping anterior bow to the plate. It is generally safer to slightly under-contour the plate rather than over-contour it; an over-contoured plate can displace the fracture into extension when the screws are tightened.
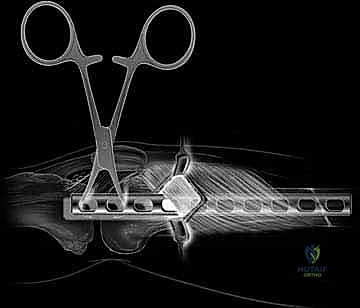
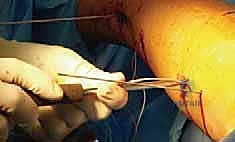
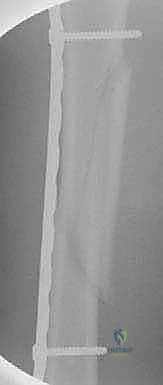
Intraoperative templating is a critical step before making any incisions. The contoured plate is placed on the skin over the anterior thigh. Using the fluoroscopic C-arm in a lateral projection, the surgeon "shadows" the plate against the lateral femur. This allows for real-time visual confirmation that the length is appropriate (spanning from the trochanteric apophysis to the distal metaphysis) and that the contour closely matches the native femoral bow.

TECH FIG 2 • The plate on the anterior thigh shadowing the lateral femur with fluoroscopy to evaluate plate contour and length.
Patient Positioning and Operating Room Setup
Proper patient positioning is arguably the most critical determinant of intraoperative success in submuscular plating. The preferred setup utilizes a radiolucent fracture table. The patient is positioned supine, and the injured extremity is placed into a boot traction system. This traction is non-negotiable; it provides the continuous longitudinal force necessary to overcome the massive deforming pull of the thigh musculature, allowing the surgeon to establish provisional reduction of length and rotation before the plate is introduced.
To facilitate unhindered fluoroscopic imaging, the patient's legs are arranged in an anteroposterior (AP) scissored position. The injured leg is held in traction, while the well leg is extended backward and abducted, either on a spar of the fracture table or supported by a well-leg holder. This scissoring prevents the well leg from superimposing over the fractured femur during lateral fluoroscopy.

TECH FIG 1 • Patient positioning in boot traction with the legs scissored in the AP direction.
If a fracture table is unavailable, a flat radiolucent Jackson or OSI table can be utilized. However, this demands dedicated surgical assistants to apply and maintain manual traction throughout the critical phases of reduction and plate application, which can be physically exhausting and less consistent than mechanical traction. Regardless of the table used, the C-arm must be positioned on the contralateral side of the injury, draped sterilely, and verified to have a full, unobstructed sweep from the hip to the knee in both true AP and true lateral projections.
Provisional Reduction Techniques
The absolute prerequisite before initiating the surgical incision is achieving a satisfactory provisional reduction of the fracture in terms of length and rotation. While coronal and sagittal alignment can be fine-tuned using the plate and strategically placed screws, correcting severe shortening or malrotation after the plate is submuscularly tunneled is exceedingly difficult and risks significant soft tissue damage.
Length is restored via the mechanical traction boot. The surgeon must clinically assess rotational alignment by observing the orientation of the patella relative to the foot. In a normal supine position, with the patella pointing directly anteriorly (towards the ceiling), the foot should rest in approximately 15 degrees of external rotation. Comparing this alignment to the uninjured contralateral limb is essential.
Fluoroscopy is then utilized to confirm the reduction. The surgeon evaluates the cortical profiles at the fracture site; cortical step-offs or a mismatch in the diameter of the proximal and distal fragments on the lateral view often indicate residual malrotation. Furthermore, evaluating the profile of the lesser trochanter on the AP view provides an excellent internal landmark for proximal segment rotation. If closed traction fails to achieve acceptable alignment due to soft tissue interposition or buttonholing of the fracture fragments, percutaneous joysticks (Schanz pins) or F-tools may be cautiously introduced into the proximal and distal fragments to manipulate them into position prior to plating.
Step-by-Step Surgical Approach and Fixation Technique
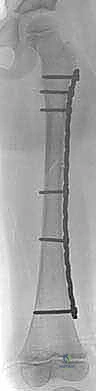
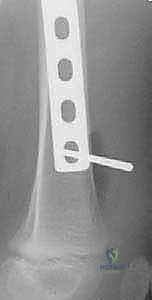
Clinical & Radiographic Imaging Archive