Cracking 11 Pediatric Cases: The Bar with Contralateral Guide
Key Takeaway
Discover the latest medical recommendations for Cracking 11 Pediatric Cases: The Bar with Contralateral Guide. A femur fracture in a 3-month-old nonambulatory child strongly indicates nonaccidental trauma (NAT), with an 80% likelihood. The immediate next step is a thorough full-body examination, including skin assessment, to identify other injuries. Management of such fractures might involve immobilization with a spica cast, potentially incorporating a bar with contralateral leg support for stability and proper alignment.
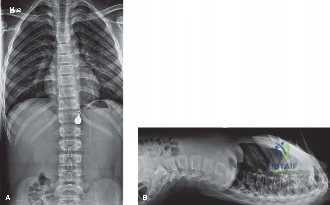
You are in the ED. A 3-month-old male is brought in by his grandmother with a swollen left thigh and "pseudoparalysis." The history is vague, and there is no reported mechanism of injury. A radiograph of the femur is obtained.

What is your immediate clinical concern, and how would you structure your initial management?
Candidate: My main concern is non-accidental trauma (NAT). I would stabilize the limb, admit the child to the hospital, and perform a full physical exam. I would order a skeletal survey and consult the pediatric safeguarding team.
Candidates often miss the medicolegal urgency. Failing to explicitly state that the child is "not for discharge," failing to order specific head imaging, or suggesting a "babygram" instead of a formal Skeletal Survey are major red flags.
The candidate must articulate: 1. Diagnostic Priority: Suspect NAT due to the age and lack of high-energy mechanism (diaphyseal fractures in non-ambulators have high specificity for abuse). 2. Immediate Action: Admission is mandatory for child safety; do not discharge. 3. Comprehensive Workup: Order a formal 21-view Skeletal Survey (ACR guidelines), non-contrast head CT to rule out abusive head trauma, and an ophthalmology consult for retinal hemorrhages. 4. Multidisciplinary approach: Early involvement of pediatric social services/safeguarding teams.
You mentioned the Skeletal Survey. Explain the rationale behind the order, and what specific findings would you be looking for that increase the specificity for abuse?
Candidate: A formal survey is required to identify occult fractures that may be in different stages of healing. I am looking for classic metaphyseal lesions (CML), rib fractures—especially posterior ones—and scapular or sternal fractures.
Providing a generic list of fractures without explaining why they are highly specific. For instance, failing to note that posterior rib fractures are pathognomonic for thoracic compression (grabbing/shaking).
Classify the lesions by their mechanical specificity: 1. CML (Classic Metaphyseal Lesion): Indicates shearing/avulsion forces. 2. Posterior Rib Fractures: Caused by thoracic compression; very high specificity. 3. Scapular, Sternal, and Spinous Process fractures: Rare in accidental childhood injury. 4. Temporal/Stages of healing: The most powerful evidence is identifying fractures of different ages, which confirms a history of repeated, non-accidental force.
The femur fracture is a mid-shaft spiral fracture. How do you manage this in a 3-month-old, and what are the limitations of the treatment you choose?

Candidate: I would manage this non-operatively with a Pavlik harness or a hip spica cast. Infants remodel angulation well, so we accept some deformity, but I need to watch for rotation.
Ignoring the "social" aspect of the decision. In an NAT case, a Pavlik harness might be contraindicated if there is any concern about compliance or if the child is to be placed in protective custody, where consistent harness adjustment by caregivers cannot be guaranteed.
State that non-operative management is the standard. Decision: Hip spica cast is often preferred over Pavlik in NAT cases for guaranteed immobilization and protection. Biomechanical targets: Remodeling allows for 30 degrees of angulation/1.5-2cm shortening, but rotational malalignment does not remodel. The cast must control rotation. Mention the "90-90" reduction technique and the necessity of the "belly-space" towel during application.
