Unlocking Shoulder Arthroscopy: Your Head and Glenoid Guide
Key Takeaway
Learn more about Unlocking Shoulder Arthroscopy: Your Head and Glenoid Guide and how to manage it. Shoulder arthroscopy is a procedure to visualize and examine the shoulder, a spheroidal multiaxial joint where the head of the humerus articulates with the glenoid fossa. This fiberoptic examination allows surgeons to assess bony anatomy, including the head and glenoid, along with surrounding muscles and capsular structures, to diagnose and treat injuries or pathology.
Introduction and Epidemiology
Shoulder arthroscopy has revolutionized the management of glenohumeral and subacromial pathology, transitioning historically open procedures into minimally invasive, highly precise interventions. As a spheroidal multiaxial joint, the shoulder relies heavily on a complex interplay between static capsuloligamentous structures and dynamic musculotendinous units to maintain stability while permitting the greatest range of motion of any joint in the human body. Arthroscopy provides unparalleled visualization of these intra-articular and bursal structures, utilizing fiberoptic instrumentation to diagnose and treat a wide spectrum of disorders.

The epidemiology of shoulder pathology presents a distinct bimodal distribution heavily influenced by patient age and activity level. Patients under the age of 40 typically present with conditions related to micro-trauma, acute traumatic events, or overuse, predominantly manifesting as glenohumeral instability or superior labrum anterior and posterior lesions. Conversely, patients over the age of 40 more frequently exhibit degenerative processes, including rotator cuff tendinopathy, full-thickness rotator cuff tears, subacromial impingement syndrome, and glenohumeral osteoarthritis. The natural history of untreated shoulder pathology often follows a predictable trajectory of progressive dysfunction. Recurrent instability rates decrease with advancing age due to capsular stiffening, whereas the prevalence of rotator cuff tears increases exponentially with age, often leading to progressive pain, motion loss, degenerative joint changes, and profound functional impairment if left unaddressed.
Surgical Anatomy and Biomechanics
A profound understanding of shoulder anatomy and biomechanics is the cornerstone of successful arthroscopic intervention. The shoulder complex achieves its massive functional envelope through a delicate balance of bony geometry, static restraints, and dynamic force couples.
Osteology and Articular Geometry
The glenohumeral joint is a highly incongruous articulation between the shallow glenoid fossa of the scapula and the hemispherical head of the humerus. The glenoid is typically retroverted between 1 and 2 degrees and has a slight superior inclination. The articular surface area of the glenoid covers only approximately 25 to 30 percent of the humeral head at any given time, creating a "golf ball on a tee" configuration. This inherent bony instability necessitates robust soft tissue stabilization.

Static Stabilizers and Capsuloligamentous Complex
The static stabilizers of the shoulder include the glenoid labrum, the joint capsule, and the glenohumeral ligaments. The labrum is a wedge-shaped, fibrocartilaginous structure that circumscribes the glenoid rim. It deepens the glenoid concavity by up to 50 percent and increases the surface area of the articulation, thereby enhancing stability through a "chock block" effect and concavity compression. The long head of the biceps tendon anchors at the superior labrum (the supraglenoid tubercle), acting as a humeral head depressor and contributing to anterior stability in abduction and external rotation.

The capsuloligamentous complex consists of discrete thickenings within the joint capsule:
* Superior Glenohumeral Ligament: Restrains inferior translation of the adducted shoulder.
* Middle Glenohumeral Ligament: Restrains anterior translation in the mid-range of abduction (45 degrees).
* Inferior Glenohumeral Ligament Complex: The most critical static stabilizer, consisting of an anterior band, a posterior band, and an axillary pouch. The anterior band is the primary restraint to anterior translation when the shoulder is abducted to 90 degrees and externally rotated.

Dynamic Stabilizers and Rotator Cuff
The dynamic stabilizers are primarily the four muscles of the rotator cuff: the supraspinatus, infraspinatus, teres minor, and subscapularis. These muscles function collectively to compress the humeral head into the glenoid concavity during active motion, a concept known as concavity compression. They also create critical force couples in both the coronal and transverse planes to balance the superior shear forces generated by the deltoid muscle.

Furthermore, the scapulothoracic articulation plays a vital role in overall shoulder biomechanics. The scapular stabilizers—including the rhomboids, levator scapulae, trapezius, and serratus anterior—must position the glenoid optimally in space to maintain the length-tension relationships of the rotator cuff and prevent impingement. Scapular dyskinesia is a frequent concomitant finding in patients with intrinsic shoulder pathology and must be addressed during rehabilitation.
Indications and Contraindications
Patient selection for shoulder arthroscopy relies on a meticulous history and a comprehensive physical examination. The mechanism of injury (traumatic versus insidious onset), the character of the pain (rest pain, night pain, activity-related), and the presence of mechanical symptoms or weakness guide the diagnostic algorithm.
Physical examination must include inspection for muscle atrophy (particularly in the supraspinatus and infraspinatus fossae), evaluation of scapular kinematics, and precise palpation. Range of motion testing helps differentiate between adhesive capsulitis (global loss of passive motion) and rotator cuff pathology (preserved passive motion with active weakness or pain). Provocative testing is essential:
* Rotator Cuff: Jobe test (supraspinatus), external rotation lag sign (infraspinatus), Hornblower sign (teres minor), and belly-press or bear-hug tests (subscapularis).
* Impingement: Neer and Hawkins-Kennedy signs.
* Instability: Apprehension, relocation, and anterior release tests.
* Labral Pathology: O'Brien active compression test and dynamic shear tests.


| Pathology | Operative Indications | Non Operative Indications |
|---|---|---|
| Anterior Instability | Recurrent dislocations, significant bone loss (Bony Bankart), failed conservative therapy, young high-demand athletes (relative). | First-time dislocation without structural deficit, voluntary dislocators, older low-demand patients. |
| Rotator Cuff Tears | Acute traumatic full-thickness tears, symptomatic chronic full-thickness tears failing >3 months of PT, significant weakness. | Partial-thickness tears (<50%), asymptomatic tears, elderly low-demand patients, advanced fatty infiltration (Goutallier 3-4). |
| Subacromial Impingement | Refractory pain failing 3-6 months of comprehensive physical therapy and corticosteroid injections, morphological acromial spurring (Type III). | First-line treatment for all patients, concurrent adhesive capsulitis (must treat stiffness first). |
| SLAP Lesions | Type II/IV lesions with mechanical symptoms failing conservative care, young overhead athletes (with caution). | Asymptomatic incidental findings, older patients (biceps tenodesis preferred over repair). |
Pre Operative Planning and Patient Positioning
Thorough preoperative planning mitigates intraoperative complications and ensures appropriate equipment is available.
Advanced Imaging Modalities
Standard radiographs (True AP, Scapular Y, and Axillary lateral views) are mandatory to assess joint space, acromial morphology, and gross osseous defects. Magnetic Resonance Imaging is the gold standard for evaluating soft tissue structures, providing detailed visualization of rotator cuff integrity, muscle atrophy, and fatty infiltration. MR Arthrography is highly sensitive for detecting labral pathology and capsular tears. In cases of recurrent instability, a computed tomography scan with 3D reconstruction and digital subtraction of the humeral head is critical for quantifying glenoid bone loss to determine if an arthroscopic soft tissue stabilization is sufficient or if a bone-block augmentation is required.

Anesthesia and Patient Positioning
Shoulder arthroscopy is typically performed under general anesthesia supplemented by a regional interscalene nerve block, which provides excellent intraoperative muscle relaxation and postoperative analgesia.
Surgeons generally utilize one of two patient positions, each with distinct biomechanical and physiological considerations:
* Lateral Decubitus: The patient is positioned on their non-operative side with the operative arm suspended in balanced traction (typically 10 to 15 pounds) at 45 degrees of abduction and 15 degrees of forward flexion. This position provides excellent visualization of the glenohumeral joint, particularly the inferior capsule and labrum, and naturally distracts the joint. However, it requires careful padding of all bony prominences to prevent neuropraxia and carries a minor risk of traction-related brachial plexus injury.
* Beach Chair: The patient is seated upright at approximately 45 to 60 degrees. This position affords an anatomic orientation, allows for easy conversion to an open procedure if necessary, and facilitates dynamic examination of the shoulder under anesthesia. However, it requires meticulous management of blood pressure to maintain adequate cerebral perfusion pressure and avoid catastrophic cerebral ischemic events.


Detailed Surgical Approach and Technique
Proficiency in shoulder arthroscopy requires a systematic, reproducible approach to portal placement and diagnostic evaluation.
Diagnostic Arthroscopy and Portal Placement
The standard posterior viewing portal is established first. The anatomic landmarks are the posterolateral corner of the acromion, the distal clavicle, and the coracoid process. The posterior portal is typically placed 2 cm inferior and 1 cm medial to the posterolateral acromial border. The arthroscope is introduced through the internervous plane between the infraspinatus (suprascapular nerve) and the teres minor (axillary nerve), directing the trocar toward the coracoid process to enter the glenohumeral joint.

An anterior working portal is then established under direct intra-articular visualization. An outside-in technique using a spinal needle ensures optimal trajectory. The needle is introduced through the rotator interval—a triangular space bordered superiorly by the supraspinatus, inferiorly by the subscapularis, and medially by the coracoid process. Placing the portal lateral to the coracoid process and superior to the subscapularis tendon minimizes the risk of injury to the musculocutaneous nerve and cephalic vein.
Glenohumeral Joint Evaluation
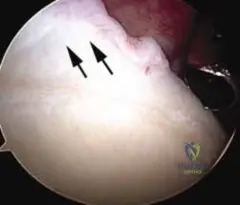
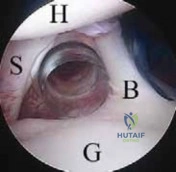
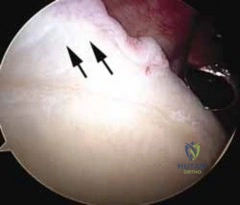
A systematic 15-point diagnostic sweep ensures no pathology is overlooked. The evaluation begins at the biceps anchor and superior labrum, assessing for fraying or detachment (SLAP lesions). The arthroscope is then directed anteriorly to evaluate the superior and middle glenohumeral ligaments and the subscapularis tendon insertion.

The anterior labrum and inferior capsular recess (axillary pouch) are inspected for Bankart lesions, capsular tears, or loose bodies. The bare area of the glenoid is visualized; a normal central osseous defect must not be confused with a chondral lesion. The posterior labrum and capsule are then examined. Finally, the arthroscope is directed superiorly to evaluate the articular surface of the supraspinatus and infraspinatus tendons for partial-thickness tears or footprint avulsions.

Subacromial Space Evaluation
Following the glenohumeral evaluation, the arthroscope is redirected into the subacromial space. A lateral portal is typically established 2 to 3 cm lateral to the acromion to serve as the primary working portal for subacromial procedures.

An extensive bursectomy is often required to achieve adequate visualization. The coracoacromial ligament and the undersurface of the acromion are inspected for morphological spurring or reactive changes indicative of impingement. The bursal surface of the rotator cuff is meticulously probed to identify full-thickness or partial-thickness bursal-sided tears. If a rotator cuff tear is identified, the mobility of the tendon, the quality of the tissue, and the status of the footprint are assessed to plan the repair strategy, which may involve single-row, double-row, or transosseous-equivalent techniques.
Complications and Management
While shoulder arthroscopy is generally safe, complications can occur and must be recognized and managed promptly. Thorough knowledge of regional neurovascular anatomy is the primary defense against iatrogenic injury.

| Complication | Incidence | Etiology and Risk Factors | Salvage and Management Strategies |
|---|---|---|---|
| Nerve Injury | 1-2% | Axillary nerve (inferior portal placement), Musculocutaneous nerve (medial anterior portal), Traction neuropraxia (lateral decubitus). | Most are transient neuropraxias resolving in 3-6 months. Observe with serial EMGs. Surgical exploration if no recovery at 3-6 months. |
| Infection | <1% | Cutibacterium acnes is the most common pathogen. Higher risk in males, revision surgery, and prolonged operative times. | Arthroscopic irrigation and debridement, hardware retention if stable, targeted systemic antibiotic therapy based on extended cultures (14 days). |
| Postoperative Stiffness | 4-15% | Prolonged immobilization, inadequate preoperative rehabilitation of adhesive capsulitis, over-tensioning of capsular repairs. | Aggressive physical therapy, oral NSAIDs/corticosteroids. Arthroscopic capsular release if refractory after 6 months of conservative care. |
| Hardware Failure | 2-5% | Anchor pullout due to poor bone quality (osteopenia), improper insertion angle, or aggressive early rehabilitation. | Revision surgery with larger anchors, alternative fixation pathways, or conversion to open procedures if massive bone loss occurs. |
| Fluid Extravasation | 5-10% | High pump pressures, prolonged surgical time, lack of outflow cannula. | Usually resolves spontaneously. Monitor airway if massive cervical extravasation occurs. Terminate procedure if compartment syndrome is suspected. |
Post Operative Rehabilitation Protocols
Postoperative rehabilitation is as critical to clinical success as the surgical execution itself. Protocols must be tailored to the specific pathology treated, balancing the mechanical protection of the healing tissue with the prevention of secondary stiffness. Biological healing dictates the timeline; the transition from disorganized Type III collagen to mature, linearly oriented Type I collagen takes approximately 6 to 12 weeks.

Standard rotator cuff repair rehabilitation follows a phased approach:
* Phase I (0-4 weeks): Strict sling immobilization. Passive range of motion within safe zones to prevent adhesions while protecting the repair. Pendulum exercises and scapular retractions.
* Phase II (4-8 weeks): Discontinuation of the sling. Initiation of active-assisted range of motion, progressing to active range of motion. Avoidance of early resistive exercises.
* Phase III (8-12 weeks): Initiation of gentle isometric and isotonic strengthening. Focus on restoring force couples and scapulothoracic kinematics.
* Phase IV (3-6 months): Advanced strengthening, plyometrics, and return to sport or heavy manual labor specific activities.
For instability repairs, rehabilitation emphasizes the protection of the anterior capsulolabral structures. External rotation is typically limited to neutral for the first 4 weeks, with a gradual return to full abduction and external rotation by 12 weeks to prevent stretching of the reconstructed tissue.
Summary of Key Literature and Guidelines
The evolution of shoulder arthroscopy is heavily supported by foundational orthopedic literature and evolving clinical guidelines. Neer's original descriptions of subacromial impingement laid the groundwork for acromioplasty, though modern literature (including recent AAOS Clinical Practice Guidelines) suggests that routine acromioplasty does not significantly improve outcomes over rotator cuff repair alone.
Burkhart's biomechanical studies on the "suspension bridge" model and transverse force couples remain critical for understanding the mechanics of massive rotator cuff tears and the rationale for partial repairs in irreparable cases. For instability, the classic open Bankart repair described by Rowe has been largely supplanted by arthroscopic techniques, with long-term studies by Boileau and others demonstrating equivalent recurrence rates provided patient selection is appropriate (e.g., utilizing the Instability Severity Index Score to rule out significant bone loss).
Furthermore, the management of SLAP lesions has shifted dramatically. Snyder's original classification guided early arthroscopic repairs, but recent high-level evidence indicates that biceps tenodesis yields superior clinical outcomes and lower complication rates compared to SLAP repair in patients over the age of 35 to 40, reflecting a paradigm shift in modern arthroscopic shoulder surgery.
Clinical & Radiographic Imaging
