Pediatric OCD: When to Consider Drilling for the Femoral
Key Takeaway
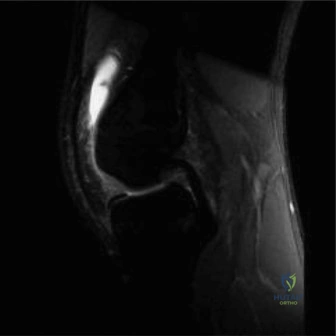
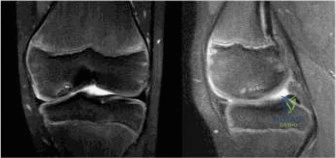
This article provides essential research regarding Pediatric OCD: When to Consider Drilling for the Femoral. Osteochondritis Dissecans (OCD) of the femoral condyle, often affecting young athletes, involves a lesion of bone and cartilage. Diagnosis includes plain films and MRI. While stable lesions in pediatric patients often heal with protected weight-bearing and bracing, surgical interventions like arthroscopic **drilling for the femoral** lesion, either antegrade or retrograde, may be performed for unstable or non-healing OCD cases.
A 13-year-old male presents with a 4-month history of vague, activity-related medial knee pain. He denies any acute injury. Physical examination reveals a trace effusion and tenderness over the medial femoral condyle at 90 degrees of flexion. The Wilson test is positive. What is the most likely diagnosis, and what are the critical components of your initial radiographic assessment?

Candidate: The most likely diagnosis is Juvenile Osteochondritis Dissecans (JOCD) of the medial femoral condyle. For the initial workup, I would order AP, lateral, and skyline views of the knee. I should also check for skeletal maturity.
Failing to mention the "Tunnel View" (PA flexion view). Candidates often forget that the classic OCD location on the lateral aspect of the medial femoral condyle is frequently obscured on a standard AP radiograph due to anatomical overlap. Also, failing to mention evaluation of the contralateral knee is a common oversight.
The clinical picture is diagnostic of JOCD. My radiographic series must include weight-bearing AP, true lateral, skyline, and crucially, a PA tunnel (notch) view to profile the posterosuperior articular surface of the condyle. I would also assess physeal status for skeletal maturity. I must evaluate the contralateral asymptomatic knee, as bilateral involvement occurs in 15-25% of cases.
You have diagnosed a stable JOCD lesion. MRI confirms the absence of a fluid cleft. The patient is 12 years old with open physes. What is the management strategy, and what criteria determine the transition to surgical intervention?
Candidate: Since the lesion is stable in a skeletally immature patient, I would recommend non-operative management. This involves activity modification and restricted weight-bearing for 3 to 6 months. I would move to surgery if it fails to heal.
Vague timelines and failure to define "failure." Candidates often forget that "failure" is defined by persistent clinical symptoms AND lack of radiographic/MRI progress after 3-6 months. They also fail to mention that the goal of surgery (drilling) is to stimulate vascularization of the necrotic subchondral bone.
The initial treatment is non-operative: 3-6 months of activity modification and restricted loading. Surgical intervention (subchondral drilling) is indicated if there is (1) failure of conservative care, (2) progression to instability (ICRS Grade II/III), or (3) approaching skeletal maturity where the healing window is closing. The biological objective of drilling is to disrupt the sclerotic rim and stimulate angiogenesis from the marrow elements into the necrotic bone fragment.
During retrograde drilling of a stable JOCD lesion, what is your primary intraoperative concern, and how do you mitigate it?

Candidate: The biggest worry is damaging the growth plate. I would use fluoroscopy to make sure I avoid the physis and don't penetrate the cartilage.
Inadequate mention of the "technical demand." Simply saying "use fluoroscopy" is insufficient. A high-scoring candidate must emphasize the precision required to bypass the physis entirely and the specific depth control to stop 2-3mm short of the subchondral bone plate to avoid iatrogenic cartilage damage.
The primary complication to avoid is iatrogenic injury to the distal femoral physis, which risks premature closure and angular deformity. I mitigate this by: (1) Pre-operative templating using MRI to map the lesion relative to the physis, (2) Utilizing intraoperative multi-planar fluoroscopy to ensure the drill trajectory avoids the physis, and (3) Constant monitoring of drill depth, aiming to terminate 2-3mm short of the articular cartilage to preserve the chondral surface while reaching the necrotic zone.
