Congenital Knee Dislocation: Pathology & Surgical Management

Key Takeaway
Congenital dislocation of the knee is a rare pediatric deformity characterized by anterior displacement of the tibia on the femur. Management depends on severity, ranging from serial casting in newborns to comprehensive surgical release in refractory cases. The Curtis and Fisher technique remains the gold standard for operative correction, utilizing anterior capsular release and quadriceps lengthening to restore joint congruity and functional flexion.
Comprehensive Introduction and Patho-Epidemiology
Congenital hyperextension and dislocation of the knee (CDK) represents a profound, highly complex spectrum of rare pediatric deformities characterized by the anterior displacement and fixed subluxation or dislocation of the tibia relative to the distal femur. First described in the 19th century, this condition continues to present a formidable reconstructive challenge for the pediatric orthopedic surgeon. The deformity is not merely an isolated capsular contracture but a multi-structural, teratologic anomaly involving the entire extensor mechanism, the collateral and cruciate ligaments, the posterior capsule, and the neurovascular bundle. The estimated incidence of CDK is approximately 1 in 100,000 live births, making it a rare entity that requires specialized, tertiary-level orthopedic care. It exhibits a slight female predominance and can present bilaterally in up to 30% of cases.
The etiology of congenital knee dislocation is multifactorial and is broadly categorized into intrinsic (genetic/syndromic) and extrinsic (packaging) causes. Extrinsic factors are typically related to severe intrauterine molding and packaging disorders. Conditions such as oligohydramnios, breech presentation, and primigravida status severely restrict the intrauterine space, forcing the fetal knees into a prolonged, rigid hyperextended posture. In these idiopathic or "packaging" cases, the prognosis is generally favorable, and the deformity is more amenable to early conservative management. Conversely, intrinsic causes are associated with underlying syndromic, genetic, or neuromuscular disorders. CDK is a hallmark finding in Larsen syndrome, arthrogryposis multiplex congenita (AMC), and myelomeningocele. In these syndromic patients, the dislocation is rigid, teratologic, and highly refractory to conservative measures, almost universally necessitating extensive surgical release.
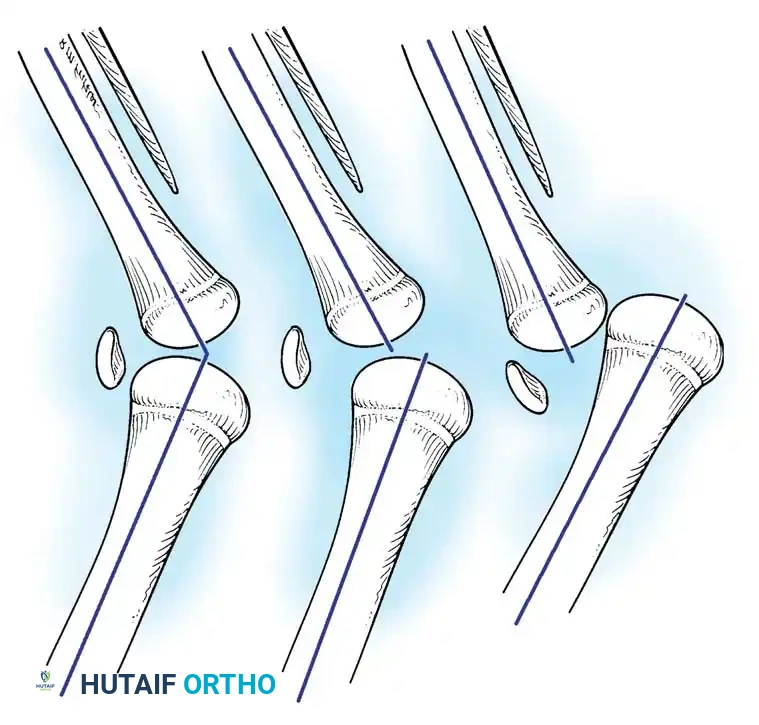
Understanding the classification and grading of severity is critical for establishing a treatment algorithm. The condition is universally divided into three distinct grades based on the severity of the tibiofemoral displacement, joint congruity, and the rigidity of the contracture. Grade 1 (Congenital Hyperextension) represents the mildest form; the tibia is hyperextended on the femur, but the articular surfaces remain congruent, and the joint can typically be passively flexed to neutral. Grade 2 (Congenital Hyperextension with Anterior Subluxation) is characterized by the anterior subluxation of the tibia on the femoral condyles. Joint congruity is partially lost, and passive flexion is significantly restricted by the contracted extensor mechanism. Grade 3 (Congenital Anterior Dislocation) is the most severe manifestation, featuring complete anterior dislocation of the tibia on the femur. The proximal tibia rests on the anterior aspect of the distal femur, and the femoral condyles are prominent posteriorly in the popliteal fossa.
Congenital hyperextension or dislocation of the knee is rarely an isolated finding; it is highly associated with skeletal abnormalities elsewhere in the extremity. The presence of CDK should immediately prompt a comprehensive evaluation for developmental dysplasia of the hip (DDH) and congenital talipes equinovarus (clubfoot). In a landmark epidemiological review, concurrent DDH was identified in up to 45% of children presenting with CDK. This concurrent presentation dictates a strict hierarchy of treatment: surgical or conservative correction of the knee must invariably precede the treatment of the hip. A flexed knee is an absolute biomechanical prerequisite for the application of a Pavlik harness or a spica cast required to treat DDH. Failure to recognize this hierarchy will result in the inability to stabilize the hip joint, leading to persistent dysplasia or frank dislocation.
Detailed Surgical Anatomy and Biomechanics
The pathoanatomy of congenital knee dislocation varies directly with the severity of the deformity, but a universal, defining feature across all grades is the severe, unyielding contracture of the anterior capsule of the knee and the quadriceps mechanism. The quadriceps muscle, particularly the rectus femoris and vastus intermedius, undergoes severe fibrotic degeneration. The muscle fibers are replaced by dense, inelastic collagenous tissue, effectively tethering the patella and the tibial tubercle to the proximal femur. The suprapatellar pouch is frequently entirely obliterated by the adherent quadriceps tendon, eliminating the normal gliding mechanism of the extensor apparatus.
Significant intraarticular and extraarticular ligamentous alterations accompany the muscular contractures. As the severity of the anterior displacement of the tibia increases, the cruciate ligaments undergo profound morphological changes. Intraoperative findings and advanced imaging frequently demonstrate cruciate ligaments that are markedly attenuated, elongated, or completely absent. While early embryological theories postulated that primary aplasia of the cruciate ligaments was the inciting event for CDK, contemporary understanding suggests that this attenuation is a secondary, adaptive result of the chronic anterior dislocation and altered mechanical stresses during fetal development. The collateral ligaments also exhibit severe positional distortion. In Grade 3 dislocations, the tibial and fibular collateral ligaments course anteriorly from their femoral epicondylar attachments, shifting their functional vectors and acting as primary tethers that resist joint reduction and flexion.
The biomechanical consequences of these anatomic distortions are profound, culminating in what is known as paradoxical extension. In a normal knee, the hamstring tendons (semimembranosus, semitendinosus, and biceps femoris) course posterior to the mechanical axis of the knee joint, functioning as primary flexors. However, in severe Grade 3 anterior dislocations, the extreme anterior translation of the tibia causes the insertion points of the hamstrings to subluxate anteriorly, crossing anterior to the mechanical axis of rotation. In this pathological configuration, the hamstrings function paradoxically as extensors of the knee. Any attempt to actively or passively flex the knee engages the hamstrings, which paradoxically forcefully hyperextend the joint further. This biomechanical trap severely complicates non-operative reduction and represents a primary indication for surgical intervention.
Patellar dysplasia and maltracking are ubiquitous in this patient population. In more than half of affected knees, the patella is hypoplastic, fragmented, or completely absent at birth. When present, the patella is almost universally displaced laterally, tethered by a fibrotic, contracted vastus lateralis and an abbreviated iliotibial band. The medial patellofemoral ligament (MPFL) equivalent is stretched and incompetent. Surgical reconstruction must therefore not only address the sagittal plane deformity (hyperextension) but also meticulously correct the coronal plane malalignment (lateral patellar tracking) to ensure long-term joint congruity and prevent early-onset patellofemoral arthrosis.
Exhaustive Indications and Contraindications
The decision-making process for the management of congenital knee dislocation requires a nuanced understanding of the patient's age, the rigidity of the deformity, and the presence of syndromic associations. Non-operative management is the absolute first line of treatment for neonates presenting with idiopathic Grade 1 or Grade 2 deformities. Serial casting, gentle manipulation, and the use of a Pavlik harness are highly successful in this demographic, provided the intervention is initiated within the first few days of life before the soft tissues lose their maternal hormone-induced laxity.
Operative intervention is strictly indicated when non-operative measures fail to achieve a concentric reduction and functional flexion (defined as >90 degrees of passive flexion) after 3 to 6 months of dedicated conservative management. Furthermore, older infants and toddlers presenting with neglected CDK are automatic candidates for surgery, as the contracted anterior structures and adaptive bony changes preclude any possibility of closed reduction. Patients with syndromic CDK, particularly those with arthrogryposis multiplex congenita or Larsen syndrome, possess rigid, teratologic dislocations that are universally refractory to casting. In these cases, early surgical intervention is indicated to facilitate the subsequent management of concurrent hip and foot deformities.
Contraindications to surgical intervention are primarily related to the patient's overall medical stability and the presence of more life-threatening congenital anomalies. Severe, uncorrected cardiac defects or profound respiratory compromise (often seen in severe syndromic packaging disorders) must take absolute precedence over orthopedic reconstruction. Additionally, active local or systemic infection is an absolute contraindication to elective orthopedic surgery. Relative contraindications include profound, non-ambulatory neuromuscular devastation where the functional benefit of a reduced knee is negligible, though even in these cases, reduction may be pursued to facilitate seating and nursing care.
| Category | Operative Indications | Contraindications |
|---|---|---|
| Patient Demographics | Neglected presentation (>6 months of age); Failure of 3-6 months of dedicated serial casting. | Medically unstable neonate; Severe, uncorrected congenital cardiac or respiratory anomalies. |
| Deformity Characteristics | Rigid Grade 2 or Grade 3 dislocations; Paradoxical hamstring extension; Fixed lateral patellar dislocation. | Grade 1 hyperextension passively correctable to >90 degrees flexion; Active local or systemic infection. |
| Syndromic Associations | Arthrogryposis Multiplex Congenita; Larsen Syndrome; Myelomeningocele with rigid deformity. | Profound, non-ambulatory neuromuscular devastation where functional goals are limited to comfort care (Relative). |
| Concurrent Anomalies | Presence of severe DDH requiring a flexed knee for Pavlik/spica treatment (necessitates early knee surgery). | Severe, uncorrected spinal anomalies (e.g., severe congenital kyphosis) taking surgical precedence. |
Pre-Operative Planning, Templating, and Patient Positioning
Thorough clinical evaluation and meticulous pre-operative planning are the cornerstones of successful surgical reconstruction in CDK. The diagnosis is typically obvious at birth, with the newborn presenting with a knee locked in severe hyperextension. Deep transverse skin creases are often visible over the anterior aspect of the joint, indicating chronic intrauterine malpositioning and forewarning the surgeon of the severe lack of anterior skin envelope available for post-operative flexion. Palpation reveals prominent, uncovered femoral condyles in the popliteal fossa, with the tibial plateau resting anteriorly. A comprehensive neurovascular examination is mandatory, as the popliteal artery is stretched tightly across the posterior aspect of the prominent femoral condyles, putting it at risk during both closed manipulation and open reduction.
Radiographic evaluation is essential to confirm the grade of dislocation and assess for associated dysplasias. Standard anteroposterior (AP) and true lateral radiographs of the knee must be obtained. The lateral radiograph will clearly demonstrate the anterior displacement of the tibia and fibula relative to the distal femur. In the neonate, the unossified chondral epiphyses can make radiographic interpretation challenging. In such cases, ultrasonography is an invaluable adjunct, allowing for real-time, dynamic assessment of joint congruity, the status of the unossified patella, and the degree of cartilaginous deformation of the distal femur and proximal tibia.

Advanced imaging, such as Magnetic Resonance Imaging (MRI), is rarely necessary for routine idiopathic cases but becomes highly valuable in older, neglected cases or complex syndromic presentations. MRI provides exquisite detail regarding the presence or absence of the cruciate ligaments, the degree of quadriceps fibrosis, and the exact anatomical location of the collateral ligament insertions. Templating involves planning the extent of the quadriceps lengthening. The surgeon must decide between an inverted V-Y plasty or a step-cut Z-plasty based on the anticipated excursion required.
Patient positioning in the operating room must facilitate circumferential access to the affected limb. The patient is placed supine on the operating table. A small bump is placed under the ipsilateral hip to control external rotation of the limb. A well-padded pediatric pneumatic tourniquet is applied to the proximal thigh, as proximal as possible to allow adequate exposure of the quadriceps mechanism. The entire lower extremity, from the tourniquet to the toes, is prepped and draped free to allow for dynamic assessment of range of motion and patellar tracking throughout the procedure. Prophylactic intravenous antibiotics are administered prior to tourniquet inflation.
Step-by-Step Surgical Approach and Fixation Technique
The definitive surgical management of congenital knee dislocation is the comprehensive soft-tissue reconstruction described by Curtis and Fisher. This procedure remains the gold standard and is designed to systematically address every contracted structure preventing concentric reduction and functional flexion. The surgery demands meticulous tissue handling and a profound understanding of pediatric knee anatomy.
Incision and Extensor Mechanism Exposure
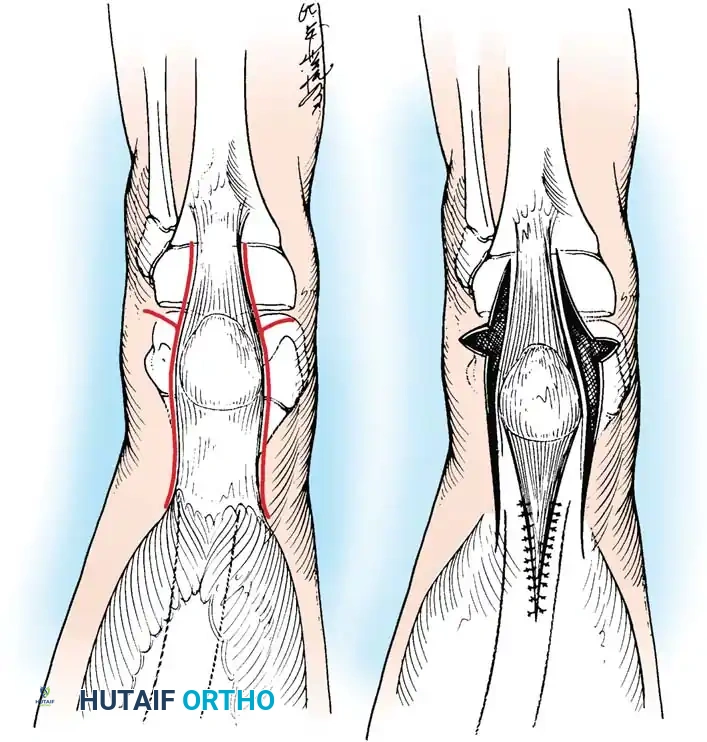
Following exsanguination and tourniquet inflation, a long anterior midline incision is utilized. The incision begins superomedially at the level of the middle third of the femur, courses distally over the midline of the joint, and extends inferolaterally to terminate just distal to the tibial tuberosity. Full-thickness fasciocutaneous flaps are meticulously developed medially and laterally to expose the anterior thigh muscles, the contracted anterior capsule, and the entire extensor mechanism. Extreme care must be taken to maintain thick skin flaps, as the anterior skin vascularity will be severely challenged when the knee is subsequently flexed.
Quadriceps Lengthening
The paramount step is the lengthening of the profoundly contracted quadriceps mechanism. This is typically achieved using an inverted V-shaped (V-Y) incision or a step-cut Z-plasty superior to the patella. The inverted V-shaped incision is generally preferred as it provides a robust, broad tongue of tendinous tissue superior to the patella, which is highly suitable for the secure, tension-free attachment of the proximal muscle mass after the extensor mechanism has been lengthened and the knee flexed. The incision is carried through the rectus femoris and vastus intermedius, carefully protecting the underlying suprapatellar pouch (if patent) or dissecting the fibrotic adhesions if the pouch is obliterated.
Capsular Release and Ligamentous Mobilization
Once the extensor mechanism is divided, attention is turned to the joint capsule. A wide, transverse division of the anterior capsule is performed. This capsulotomy must be extended posteriorly along both the medial and lateral joint lines to the anterior borders of the tibial (medial) and fibular (lateral) collateral ligaments. As the knee is gently, incrementally flexed, the surgeon must carefully mobilize and displace these collateral ligaments posteriorly. This critical maneuver relocates the axis of rotation from its pathological anterior position back to its true anatomic center, neutralizing the tethering effect of the collaterals.
Patellar Realignment and Intraarticular Debridement
The patella is almost universally subluxated laterally. To correct this, a radical release of the lateral retinaculum, the lateral aspect of the patellar tendon, and the fibrotic vastus lateralis is performed. Any tight iliotibial band structures inserting onto Gerdy's tubercle are fractionally lengthened or released. Inside the joint, the surgeon must lyse any intraarticular adhesions between the femur and tibia. The intercondylar notch is inspected; if remnants of the cruciate ligaments are present and blocking reduction, they must be carefully debrided.
Extensor Mechanism Repair and Closure
With the knee now capable of passive flexion to at least 90 degrees and concentrically reduced, the extensor mechanism is repaired. All normal-appearing quadriceps muscle tissue is mobilized. The muscle mass is aligned in the long axis of the femur to ensure it exerts a direct, centralized pull on the patella. The lengthened quadriceps mechanism is sutured using heavy, non-absorbable or slow-absorbing braided sutures. The vastus medialis obliquus (VMO) must be meticulously advanced and repaired to the medial border of the lengthened rectus femoris to provide a dynamic medial stabilizing force, preventing recurrent lateral patellar subluxation.
The tourniquet is deflated prior to closure to ensure meticulous hemostasis, minimizing the risk of a post-operative hematoma that could compromise the already tenuous anterior skin flap. The wound is closed in layers. Crucially, the knee is casted in only 30 to 45 degrees of flexion. Attempting to cast the knee in maximum flexion immediately post-operatively places the chronically contracted anterior skin under extreme, intolerable tension, leading to a catastrophic risk of skin necrosis and wound dehiscence.
Complications, Incidence Rates, and Salvage Management
Surgical reconstruction for congenital knee dislocation is a major undertaking fraught with potential complications. The most dreaded early post-operative complication is anterior skin necrosis. Because the anterior skin has been chronically contracted in the hyperextended position, flexing the knee acutely places immense tension on the incision line. If the skin blanches and capillary refill is lost during closure, the knee must be extended until perfusion returns. Skin necrosis can lead to deep infection, exposure of the extensor mechanism repair, and catastrophic failure of the procedure.
Arthrofibrosis and loss of flexion are common late complications, particularly in syndromic patients (e.g., arthrogryposis) who possess an intrinsic propensity for severe scar formation. Despite a perfect intraoperative release, these patients may rapidly stiffen, losing the flexion gained during surgery. Recurrent hyperextension or anterior subluxation can occur if the quadriceps lengthening was insufficient, if the collateral ligaments were not adequately mobilized posteriorly, or if the patient is non-compliant with post-operative bracing protocols.
In rare, neglected cases in older children (typically >3 years of age), the soft tissue contractures are so severe, and the neurovascular bundle so shortened, that soft tissue release alone is insufficient to achieve reduction without causing ischemic injury to the limb. In these severe salvage scenarios, a femoral shortening osteotomy or a distal femoral flexion osteotomy is required. By shortening the bony skeleton, relative length is granted to the contracted soft tissues and neurovascular structures, allowing for a concentric joint reduction without excessive tension.
| Complication | Estimated Incidence | Prevention and Salvage Management |
|---|---|---|
| Anterior Skin Necrosis | 5% - 15% | Prevention: Cast in only 30-45° flexion initially; meticulous hemostasis before closure. Management: Immediate cast removal and extension of the knee; wound debridement; possible rotational flap coverage for exposed tendon. |
| Arthrofibrosis / Stiffness | 20% - 40% (Higher in AMC) | Prevention: Early mobilization (CPM) if wound allows; aggressive physical therapy. Management: Manipulation under anesthesia (MUA); arthroscopic or open lysis of adhesions; continuous splinting. |
| Recurrent Subluxation | 10% - 20% | Prevention: Adequate posterior mobilization of collateral ligaments; prolonged KAFO bracing (6-12 months). Management: Revision soft tissue release; distal femoral flexion osteotomy for fixed bony deformity. |
| Patellar Instability | 15% - 25% | Prevention: Meticulous lateral release and VMO advancement during initial surgery. Management: MPFL reconstruction; tibial tubercle osteotomy (Roux-Goldthwait or Fulkerson) in older children. |
| Neurovascular Compromise | < 2% | Prevention: Avoid excessive traction during reduction; consider femoral shortening osteotomy in older/neglected cases. Management: Immediate removal of cast/splint; vascular surgery consultation; emergent exploration if ischemia persists. |
Phased Post-Operative Rehabilitation Protocols
The post-operative management following a Curtis and Fisher release or similar extensive soft-tissue reconstruction requires a highly structured, phased approach. The rehabilitation protocol must delicately balance two competing interests: protecting the tenuous soft tissue repair (both the quadriceps lengthening and the anterior skin incision) and preventing the rapid onset of intraarticular arthrofibrosis.
Phase 1: Initial Immobilization and Wound Protection (0 to 2 Weeks)
Immediately following surgery, the patient is placed in a well-padded, long leg bivalved cast or rigid splint with the knee flexed to a safe angle, typically between 30 and 45 degrees. The primary goal of this phase is wound healing and the prevention of skin necrosis. The limb is strictly elevated to minimize edema. If the anterior skin was noted to be under excessive tension during surgical closure, the cast may be bivalved in the recovery room. At 10 to 14 days post-operatively, the cast is removed under mild sedation or outpatient anesthesia to meticulously inspect the wound. If the incision is healing well, the sutures are removed, and the knee is gently manipulated to incrementally increase flexion before a new cast is applied.
Phase 2: Controlled Mobilization (2 to 6 Weeks)
Once the anterior incision is fully healed and stable (typically around 2 to 3 weeks), the focus shifts to regaining range of motion. The rigid cast is completely removed. In older, cooperative patients, continuous passive motion (CPM) machines are highly beneficial during this phase to regain motion and prevent the reformation of dense intraarticular adhesions. Active-assisted and passive range-of-motion exercises are initiated under the strict guidance of a pediatric physical therapist. The goal during this phase is to achieve at least 90 degrees of flexion while protecting against active, forceful quadriceps contraction that could rupture the V-Y or Z-plasty repair. A hinged knee brace is worn between therapy sessions, locked at 30 degrees of flexion to prevent the recurrence of hyperextension.
Phase 3: Long-Term Bracing and Strengthening (6 Months to 1 Year)
To protect the lengthened quadriceps and definitively prevent a recurrence of the hyperextension deformity, a custom-molded knee-ankle-foot orthosis (KAFO) or a long leg brace is prescribed. This brace is typically locked with an extension block to prevent terminal extension (blocking the last 10-15 degrees of extension) while allowing free flexion. The brace is worn full-time for the first 3 to 6 months, then transitioned to nighttime and naptime wear for up to a year. Physical therapy focuses on progressive quadriceps and hamstring strengthening, gait training, and proprioceptive re-education. Regular clinical and radiographic follow-up is mandatory at 3, 6, and 12 months post-operatively to monitor joint congruity, patellar tracking, and the symmetric development of the femoral condyles and tibial plateau.
Summary of Landmark Literature and Clinical Guidelines
The evolution of the surgical and non-surgical management of congenital knee dislocation is deeply rooted in several landmark studies that continue to dictate modern clinical guidelines. The epidemiological understanding of the disease was fundamentally shaped by the landmark study of Katz, Grogono, and Soper, who reviewed 155 children with CDK. They definitively established the high correlation between CDK and other musculoskeletal packaging disorders, notably finding that 45 of these children presented with concurrent developmental dysplasia of the hip (DDH). This study cemented the clinical guideline that a thorough secondary survey for hip and foot anomalies is absolutely mandatory upon the diagnosis of CDK.
The surgical gold standard was established by Curtis and Fisher, who detailed the comprehensive anterior soft-tissue release, quadriceps lengthening, and collateral ligament mobilization technique. Their focused study of 15 knees with congenital hyperextension and anterior subluxation demonstrated that isolated capsular release was insufficient, and that addressing the profound quadriceps contracture and lateral patellar tethering was essential for durable success. Their step-by-step methodology remains the foundation of the operative technique utilized by pediatric orthopedic surgeons today.
Regarding non-operative management, Ko, Shih, and Wenger provided the definitive evidence for the efficacy of early intervention. In their series of 24 congenital knee dislocations treated within the first month of life, they demonstrated that immediate reduction, serial casting, and traction yielded excellent or good results in all patients devoid of syndromic anomalies. Their work established the guideline that conservative management is the absolute first line of treatment for idiopathic cases presenting in the neonatal period.
Finally, Roach and Richards proposed the strict, universally accepted criteria for defining the success of non-operative treatment: radiographic evidence of concentric joint reduction and the clinical achievement of knee flexion to 90 degrees or more. These criteria serve as the definitive threshold; failure to meet these benchmarks after 3 to 6 months of conservative management is the universally recognized trigger for transitioning to the operative interventions detailed in this chapter.
