9 Pediatrics Cases: Essential Insights on Rotation of the Foot

Key Takeaway
Looking for accurate information on 9 Pediatrics Cases: Essential Insights on Rotation of the Foot? Tibial tubercle fractures are more common in adolescents with Osgood–Schlatter disease, an overuse injury. A significant risk with this fracture is anterior compartment syndrome, potentially involving the recurrent anterior tibial artery. These injuries often occur during sports activities requiring sudden, forceful knee extension or impacts, which can sometimes involve quick acceleration combined with rotation of the foot.
A 14-year-old male arrives in the emergency department with a swollen, painful knee following a jump during a basketball game. He is unable to perform a straight leg raise. Describe your initial assessment priorities and the most critical neurovascular threat you are screening for.
Candidate: I would assess for a tibial tubercle avulsion. I'd perform a primary survey, then a neurovascular exam. The main risk is an extensor mechanism failure. I would check pulses, sensation, and the compartments of the leg to look for compartment syndrome.
Failing to emphasize the insidious nature of compartment syndrome in this specific injury. Candidates often list "check pulses" as sufficient, failing to recognize that pulses remain intact in compartment syndrome until very late stages. Neglecting to mention the mechanism of injury (eccentric load) or the prodromal history of Osgood-Schlatter suggests a lack of clinical depth.
I would prioritize evaluating the integrity of the extensor mechanism and ruling out a displacement injury. Given the mechanism—an explosive eccentric contraction—I suspect an Ogden Type III tibial tubercle avulsion. My highest priority is assessing for acute anterior compartment syndrome. I would perform serial neurovascular exams, specifically checking the sensation of the first web space (deep peroneal nerve) and pain on passive extension of the hallux. I must recognize that the recurrent anterior tibial artery is at high risk, and because the fascial compartment is tight, the patient may develop compartment syndrome despite having palpable distal pulses.
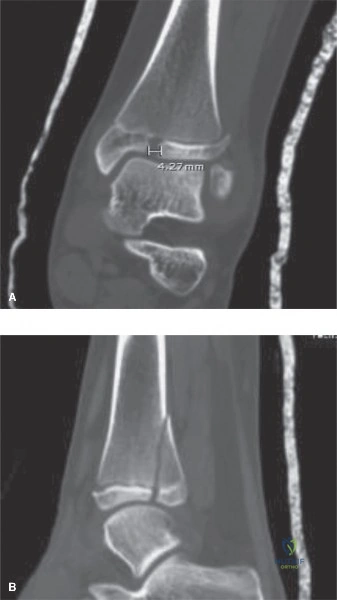
You have confirmed an avulsion fracture. Look at the provided imaging. How do you classify this injury, and what are the implications for your surgical management?

Candidate: This is an Ogden Type III fracture. It extends into the joint. I would fix it with screws to restore the articular surface and ensure the patient can perform a straight leg raise.
Ignoring the "articular" nature of Type III injuries. A candidate who fails to mention the need for joint inspection risks leaving the patient with post-traumatic osteoarthritis. Also, failing to discuss the management of the periosteal sleeve or the potential for meniscal entrapment shows a narrow focus on bone fixation only.
This is an Ogden Type III-B injury. Because it violates the articular surface of the tibial plateau, ORIF is mandatory. My surgical plan includes: 1) Arthrotomy to inspect the joint and rule out entrapment of the anterior horn of the lateral meniscus, which is a known block to reduction. 2) Anatomical reduction and lag screw fixation (usually 4.0 or 4.5mm). 3) Repair of the medial and lateral periosteal sleeve, as this provides crucial secondary stability to the extensor mechanism. 4) I would also discuss the strong indication for a prophylactic anterior compartment fasciotomy given the trauma to the recurrent anterior tibial vessels.
The surgery went well, and you achieved stable fixation. How do you approach the rehabilitation, and when do you plan to address the hardware?

Candidate: I'd keep them in a brace locked in extension for six weeks. Then I'd start moving it. If they have pain from the screws, I will take the hardware out after a year.
Prescribing a "one-size-fits-all" six-week immobilization period without addressing the importance of controlled range of motion to prevent arthrofibrosis. Additionally, failing to mention the contraindication of active quadriceps exercises in the early phase is a major safety oversight.
Rehabilitation must be staged to protect the extensor mechanism. - Weeks 0–2: Immobilization in full extension; strict NWB to protect the construct. - Weeks 2–6: Initiate controlled PROM in a hinged brace, gradually advancing flexion. Active quadriceps contraction is strictly contraindicated during this period. - Weeks 6–12: Transition to AROM and closed-chain strengthening once radiographic union is evident. - Hardware: I would counsel the patient that the screw heads are prominent and may require removal. This is never performed before 6–9 months, once the bone has fully remodeled, to avoid refracture through the screw tracks.
