Masterclass: Comprehensive Surgical Management of Congenital Femoral Deficiency

Key Takeaway
Welcome, fellows, to a deep dive into congenital femoral deficiency (CFD) management. This masterclass will guide you through the intricacies of Paley classification, meticulous preoperative planning, and the precise execution of hip and knee reconstruction procedures, including the Superhip, Dega osteotomy, and femoral lengthening. We'll cover comprehensive surgical anatomy, critical intraoperative steps, pearls, pitfalls, and postoperative care, preparing you for complex CFD cases.
Welcome, fellows, to the operating theater. Today, we are tackling one of the most intellectually demanding and technically rigorous areas in pediatric orthopaedics: the comprehensive surgical management of Congenital Femoral Deficiency (CFD). This is not merely a matter of applying an external fixator to lengthen a bone; it is a profound reconstructive undertaking. We are tasked with rebuilding a functional limb from a foundation of profound pathoanatomy, addressing complex, multi-planar deformities of the hip, knee, and the entire lower extremity. Our overarching goal is to provide these young patients with the best possible functional outcome, achieving a plantigrade, stable, and biomechanically sound limb through a series of meticulous, staged procedures.
Comprehensive Introduction and Patho-Epidemiology
Congenital Femoral Deficiency represents a complex spectrum of lower extremity anomalies characterized by a shortened femur, altered hip and knee biomechanics, and a constellation of associated soft tissue contractures. Historically referred to as Proximal Femoral Focal Deficiency (PFFD), the contemporary nomenclature of CFD, championed by Paley, is vastly preferred. This shift in terminology reflects a deeper understanding that the pathology is rarely confined to the proximal femur alone; rather, it encompasses the entire limb, including profound acetabular dysplasia, knee ligamentous incompetence, and significant limb length discrepancy (LLD). The paradigm of treatment has evolved dramatically from early amputation and prosthetic fitting to a philosophy of joint preservation, stabilization, and sequential lengthening.
The epidemiology of CFD reveals it to be a rare entity, with an incidence estimated at approximately 1 in 50,000 to 1 in 100,000 live births. The etiology remains largely sporadic, though teratogenic exposures (most infamously, thalidomide in the mid-20th century) and viral infections during the critical window of limb bud formation (4th to 6th weeks of gestation) have been implicated. Recent molecular research points toward disruptions in the Sonic Hedgehog (SHH) signaling pathway and errors in the apical ectodermal ridge (AER) function, which dictate proximo-distal limb outgrowth. Despite these insights, the vast majority of cases present without a clear genetic or environmental trigger, necessitating a highly individualized approach to each patient's unique morphological presentation.


The Paley classification system serves as our definitive roadmap for surgical decision-making. It is not merely descriptive; it is highly prescriptive, dictating our reconstructive strategy based on the integrity of the hip and knee joints. Type 1 represents an intact femur with mobile hip and knee joints, subdivided into Type 1a (normal ossification) and Type 1b (delayed ossification). Type 1b is characterized by a "stiff cartilaginous pseudarthrosis" in the subtrochanteric or neck region—a critical distinction, as this cartilage has the potential to ossify following appropriate biomechanical realignment. Type 2 involves a mobile pseudarthrosis with a mobile knee, where Type 2a features a mobile femoral head within the acetabulum, and Type 2b features an absent or stiff femoral head. Types 3 and 4 represent severe diaphyseal and distal deficiencies, respectively, often requiring entirely different management algorithms, including rotationplasty or early prosthetic fitting.
Beyond the osseous deficiency, we must recognize that CFD is a syndrome of profound soft tissue and joint pathomechanics. Acetabular dysplasia is nearly universal, presenting with a shallow vault and inadequate femoral head coverage, which risks catastrophic subluxation during subsequent limb lengthening. Coxa vara is typically severe, with neck-shaft angles frequently plummeting below 90 degrees, exacerbated by relentless abduction and flexion contractures of the pelvifemoral musculature. Furthermore, the knee joint is rarely spared; patients routinely exhibit hypoplasia of the lateral femoral condyle, absent cruciate ligaments leading to anteroposterior instability, and severe external rotatory subluxation of the tibia driven by a contracted iliotibial band.


Detailed Surgical Anatomy and Biomechanics
Before we make any incision, a masterful understanding of the regional pathoanatomy is paramount. We are operating in critical zones with distorted landmarks and high neurovascular risk. The osteology of the proximal femur in CFD is highly variable and often deceptive on standard radiographs. Acetabular dysplasia manifests as a steep acetabular roof, measurable by a high Acetabular Index (AI) and a severely reduced Center-Edge (CE) angle of Wiberg. The proximal femur itself is characterized by profound coxa vara and retroversion, creating a biomechanical environment where the abductor mechanism is critically disadvantaged. The greater trochanter often overrides the femoral head, leading to a profound Trendelenburg gait and functional weakness that must be corrected through a valgus-producing osteotomy.
The muscular intervals in CFD are defined by severe, unyielding contractures that distort standard surgical approaches. The abduction contracture is primarily driven by the tensor fascia lata (TFL), gluteus medius, and gluteus minimus. The TFL, originating from the anterior iliac crest, acts as a deforming tether laterally. The flexion contracture is a combined force of the rectus femoris, TFL, and the deep psoas muscle. Releasing the rectus femoris from its origin at the anterior inferior iliac spine (AIIS) and performing a fractional lengthening or tenotomy of the psoas at the pelvic brim are critical steps to achieving hip extension. Furthermore, external rotation contractures, heavily influenced by a fibrotic piriformis and the short external rotators, must be meticulously released to allow for internal rotation and proper seating of the femoral head.


Navigating the neurovascular structures in this distorted anatomy requires extreme vigilance. The superior gluteal nerve and artery, emerging from the greater sciatic notch superior to the piriformis, are at high risk during extensive posterior capsular releases and gluteal elevations. Injury here results in irreversible abductor paralysis. The sciatic nerve, exiting inferior to the piriformis, is extraordinarily vulnerable. Because the femur is shortened, the sciatic nerve often takes an anomalous, relatively superficial course and can be bowstrung during acute correction of severe flexion deformities or during aggressive lengthening. Anteriorly, the femoral nerve and artery must be protected during the release of the rectus femoris and the iliopsoas.
The distal anatomy surrounding the knee presents its own set of biomechanical hurdles. The distal femoral epiphysis is often dysplastic, with a characteristic hypoplasia of the lateral condyle that drives genu valgum and lateral patellar maltracking. Ligamentous incompetence, particularly the absence of the anterior cruciate ligament (ACL), forces the surgeon to rely on dynamic muscular stabilizers and precise alignment to prevent subluxation. The iliotibial band (ITB) acts as a dense, unyielding lateral tether; its contracture is a primary driver of external rotatory instability of the knee and fixed flexion deformities. The peroneal nerve, winding around the fibular neck, is at extreme risk during ITB releases, lateral capsulotomies, and the placement of proximal tibial half-pins for external fixation.


Exhaustive Indications and Contraindications
The philosophy of treating Congenital Femoral Deficiency is rooted in the principle that joint stability must precede limb lengthening. Attempting to lengthen a femur in the presence of an uncorrected dysplastic acetabulum or severe coxa vara will inevitably result in catastrophic hip dislocation, joint destruction, and a severe decline in patient function. Therefore, reconstructive procedures such as the "Superhip" (comprehensive soft tissue release, pelvic osteotomy, and proximal femoral osteotomy) are indicated to establish a biomechanically sound foundation. We utilize the Multiplier Method to accurately predict the ultimate Limb Length Discrepancy (LLD) at skeletal maturity. This prediction is critical; it dictates whether the patient will require one, two, or three staged lengthenings throughout childhood, or if the discrepancy is so profound that prosthetic management is the more rational choice.
Specific indications for comprehensive hip reconstruction (the Superhip procedure) include Paley Type 1b and Type 2 CFD presenting with severe coxa vara (neck-shaft angle < 110 degrees), significant acetabular dysplasia (CE angle < 20 degrees, AI > 30 degrees), and profound soft tissue contractures that preclude neutral positioning of the limb. The procedure is typically performed between 18 and 24 months of age, creating a stable osseous and soft-tissue environment that is allowed to heal and remodel for at least one year prior to the initiation of the first femoral lengthening phase. In Type 2a cases, the true mobile pseudarthrosis must be resected and bone-grafted to achieve osseous continuity, whereas in Type 1b, the cartilaginous anlage is preserved, as it will predictably ossify once the biomechanical stresses of coxa vara are neutralized via a valgus osteotomy.
Contraindications to massive reconstructive surgery must be carefully weighed, as these procedures carry significant morbidity. Absolute contraindications include severe, unmanageable neuromuscular diseases (e.g., profound cerebral palsy with global spasticity) where the patient lacks the motor control to utilize a reconstructed limb. Profound cognitive impairment that precludes participation in the grueling, months-long postoperative rehabilitation and lengthening protocols is also a strong contraindication. Anatomically, Paley Type 3c (complete absence of the femur) and severe forms of Type 3b with a rigid, non-functional knee joint are generally better served by early Syme amputation or Van Nes rotationplasty, followed by prosthetic fitting, rather than doomed attempts at heroic reconstruction.
When reconstruction is contraindicated or the predicted LLD exceeds 20-25 centimeters, alternative strategies must be employed. Contralateral epiphysiodesis can manage minor discrepancies but is insufficient for the massive LLD seen in severe CFD. Amputation—specifically knee disarticulation or Syme amputation—coupled with modern prosthetic technology often provides a highly functional, cosmetically acceptable, and significantly less morbid outcome for patients with profound deficiencies. The decision between reconstruction and amputation is the most critical juncture in CFD management and requires exhaustive, transparent counseling with the patient's family.
| Parameter | Indications for Reconstruction (Superhip/Lengthening) | Contraindications (Consider Amputation/Prosthetics) |
|---|---|---|
| Paley Classification | Type 1a, 1b, 2a, 2b; Select Type 3a | Severe Type 3b, Type 3c, Type 4 |
| Predicted LLD at Maturity | < 20-25 cm (manageable with 2-3 lengthenings) | > 25-30 cm (heroic, high complication rate) |
| Hip Joint Status | Reconstructable dysplasia, treatable coxa vara | Absent acetabulum, unyielding fixed dislocation |
| Knee Joint Status | Mobile knee (>45° arc), reconstructable ligaments | Rigid knee (<45° arc), severe uncorrectable instability |
| Patient/Family Factors | High compliance, robust psychosocial support | Non-compliant, severe cognitive/neuromuscular deficits |



Pre-Operative Planning, Templating, and Patient Positioning
Meticulous preoperative planning is the bedrock upon which successful CFD reconstruction is built; intraoperative improvisation in these cases is a recipe for disaster. The planning phase begins with high-quality, standardized imaging. Long standing anteroposterior (AP) and lateral radiographs of the entire lower extremities are mandatory. Crucially, the radiologic technician must be instructed to pull both lower limbs down into maximum extension. This maneuver negates the ubiquitous hip and knee flexion contractures, revealing the true osseous alignment and allowing for accurate measurement of femoral and tibial segments. Advanced imaging, specifically MRI, is invaluable for visualizing the unossified cartilaginous anlage in Type 1b and Type 2 deformities, helping to differentiate a delayed ossification center from a true fibrous pseudarthrosis.
The gold standard for definitive preoperative assessment is the dynamic arthrogram performed under general anesthesia. Once the child is relaxed, contrast dye is injected into the hip joint. Under live fluoroscopy, the surgeon dynamically manipulates the limb through a full range of motion. This real-time assessment definitively confirms the presence of a true mobile pseudarthrosis (Type 2a, where dye pools in the false joint space) versus delayed ossification (Type 1b, where the cartilaginous connection moves as a single unit with the shaft). The arthrogram also provides a perfect outline of the cartilaginous femoral head, allowing precise measurement of the CE angle and guiding the exact degree of correction required for the Dega pelvic osteotomy.




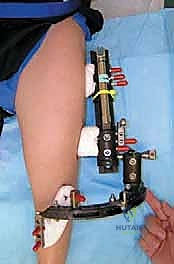
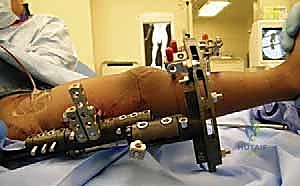
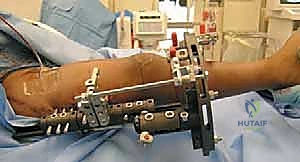
Hardware templating is an exact science in CFD management. Using digital templating software calibrated to the patient's radiologic markers, we pre-select the specific implants required. For the proximal femoral osteotomy, pediatric hip plates (e.g., 100-degree, 110-degree, or 130-degree blade plates or locking equivalents) are templated to match the planned Valgus Derotation Osteotomy (VDRO). We calculate the exact wedge resection angle required to restore a normal neck-shaft angle and correct retroversion. If an external fixator is planned for a concurrent or subsequent phase, the frame components—rings, arches, half-pins, and tensioned wires—are mapped out to ensure adequate clearance for soft tissue swelling and to avoid neurovascular bundles.
Patient positioning and operating room setup must be optimized to facilitate seamless fluoroscopic imaging without compromising the sterile field. The patient is typically positioned supine on a fully radiolucent operating table. A small bump may be placed under the ipsilateral hemipelvis to elevate the operative field. The entire affected limb is prepped and draped freely from the umbilicus to the toes, allowing unrestricted manipulation. The contralateral limb is also prepped into the field to serve as an anatomical reference for length and rotation. The C-arm fluoroscopy unit must be positioned—usually coming in from the contralateral side—so that it can easily rotate to capture true AP and lateral views of both the hip and knee without requiring the surgical team to physically lift or reposition the patient's torso.



Step-by-Step Surgical Approach and Fixation Technique
The "Superhip" procedure is a masterclass in comprehensive soft tissue and osseous reconstruction. It systematically addresses the contractures, the acetabular dysplasia, and the proximal femoral deformity in a single, extensive operative setting.
Soft Tissue Releases and Exposure
The procedure commences with an extensive soft tissue release to neutralize the deforming forces acting on the hip. We utilize a modified anterior Smith-Petersen approach, extending the incision proximally along the iliac crest and distally along the tensor fascia lata. The first critical step is the complete release of the TFL and the anterior fascia of the gluteus medius and minimus from the iliac crest, effectively eliminating the abduction contracture. We perform a subperiosteal elevation of these muscles down to the greater trochanter. The rectus femoris is identified, and its direct head is detached from the AIIS, while the reflected head is released from the superior acetabular rim. This addresses the anterior flexion tether.
Deep dissection proceeds to expose the hip capsule. The iliopsoas tendon is identified as it crosses the pelvic brim and is lengthened fractionally or tenotomized to further alleviate the flexion contracture. To address the external rotation deformity, the piriformis tendon is identified at its insertion on the greater trochanter and released. Throughout this exposure, meticulous hemostasis is maintained, and the sciatic nerve—which may be dangerously close to the posterior operative field due to the distorted anatomy—is protected by maintaining a strict subperiosteal dissection plane along the posterior femoral neck and trochanter.




Dega Osteotomy for Acetabular Dysplasia
Once the soft tissues are released and the capsule is exposed, we address the acetabular dysplasia using a Dega-type incomplete trans-iliac osteotomy. The inner table of the ilium is exposed by elevating the iliacus muscle subperiosteally. Using a fluoroscopically guided osteotome, a curvilinear cut is made starting just above the AIIS, sweeping posteriorly 1 to 1.5 centimeters above the acetabular rim, and terminating at the greater sciatic notch. Crucially, the osteotomy cuts through the outer and inner cortices but hinges on the flexible triradiate cartilage medially and the intact sciatic notch posteriorly.
The osteotomy is then carefully levered open using lamina spreaders. This maneuver hinges the acetabular roof downward and laterally, dramatically increasing the CE angle and providing robust anterolateral coverage of the femoral head. We confirm the adequacy of coverage fluoroscopically with an arthrogram. Once optimal coverage is achieved, the triangular gap created in the ilium is packed with structural allograft or autograft harvested from the subsequent femoral wedge resection. This graft maintains the correction and facilitates rapid osseous consolidation of the pelvic osteotomy.



Proximal Femoral Osteotomy and Fixation
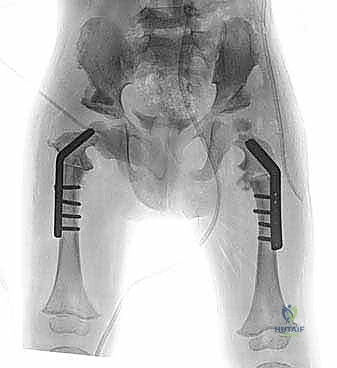
With the acetabulum reconstructed, attention turns to the proximal femur. A Valgus Derotation Osteotomy (VDRO) is performed at the subtrochanteric level. A guide wire is placed into the femoral neck and head—or into the cartilaginous anlage in Type 1b cases—at the precise angle calculated during templating. A pediatric blade plate or a specialized locking plate is driven over this wire. The osteotomy is then completed transversely. A medially based closing wedge of bone is often resected to correct the severe coxa vara, elevating the neck-shaft angle to approximately 130-140 degrees.
The distal femoral fragment is then externally rotated (derotated) to correct the inherent retroversion, and abducted to meet the proximal fragment. The plate is secured to the distal shaft with cortical screws. In Type 2a cases, where a true pseudarthrosis exists, the fibrous tissue must be meticulously resected back to healthy, bleeding bone on both the capital and trochanteric sides before fixation, and the site is heavily grafted with autologous bone to stimulate union. Rigid internal fixation is the absolute requirement here, as the biomechanical forces acting on this osteotomy during the healing phase are immense.



Knee Joint Stabilization and Distal Procedures
While the "Superhip" focuses proximally, concurrent distal procedures are frequently required to address knee pathology, often termed the "Superknee" procedure. If a severe knee flexion contracture is present, a radical release of the posterior structures is undertaken. This includes fractional lengthening of the hamstring tendons (biceps femoris, semimembranosus, semitendinosus) and a meticulous posterior capsulotomy of the knee joint. The popliteal neurovascular bundle must be identified and protected throughout this deep posterior dissection.
Furthermore, the contracted iliotibial band, which drives external rotatory subluxation of the tibia and lateral patellar maltracking, must be addressed. A complete transverse release or Z-lengthening of the ITB is performed just proximal to the knee joint. In cases of severe anteroposterior instability due to absent cruciate ligaments, extra-articular tenodesis procedures or, in older children, intra-articular ligamentous reconstructions may be indicated to provide a stable platform for eventual limb lengthening. The goal is to achieve a knee that can fully extend and track centrally, preventing catastrophic subluxation when the massive distracting forces of a fixator are eventually applied.