Introduction and Epidemiology
The posterior approach to the shoulder joint, while less frequently employed than its anterior counterparts, offers critical exposure to the posterior glenoid, humeral head, and surrounding structures. Its application is typically reserved for specific, often complex, pathological conditions that demand direct visualization and manipulation of these posterior aspects. Historically, open posterior approaches were a mainstay for addressing recurrent posterior instability. However, advancements in arthroscopic techniques have refined the indications, largely limiting the open approach to scenarios requiring extensive bone work, tumor excision, complex fracture management, or revision arthroplasty.
Epidemiologically, conditions necessitating a posterior open approach are uncommon. Posterior glenohumeral dislocations represent approximately 2 to 5 percent of all shoulder dislocations. These injuries are classically associated with violent muscle contractions, such as those occurring during epileptic seizures, electrocution, or high-energy motor vehicle collisions. While a significant proportion of acute posterior dislocations are amenable to closed reduction or arthroscopic intervention, complex posterior fracture-dislocations, chronic locked dislocations, or cases with substantial posterior glenoid bone loss often mandate an open posterior approach for optimal reduction and rigid internal fixation.
Similarly, neoplastic processes or deep space infections localized to the posterior scapula, posterior glenoid neck, or posterior capsular structures are rare but demand direct, wide access for biopsy, en bloc excision, or aggressive debridement. Understanding the nuanced indications and meticulous surgical technique for this approach is paramount for any orthopedic surgeon managing complex shoulder pathology. The ability to safely navigate the posterior shoulder musculature while protecting the axillary and suprascapular nerves distinguishes the advanced shoulder surgeon.
Surgical Anatomy and Biomechanics
A thorough understanding of the regional anatomy is foundational to safely and effectively utilizing the posterior approach. The surgical exposure relies on navigating precise internervous planes or performing safe muscle splits while avoiding iatrogenic injury to the neurovascular bundles that supply the posterior rotator cuff and deltoid.
Bony Landmarks of the Posterior Shoulder
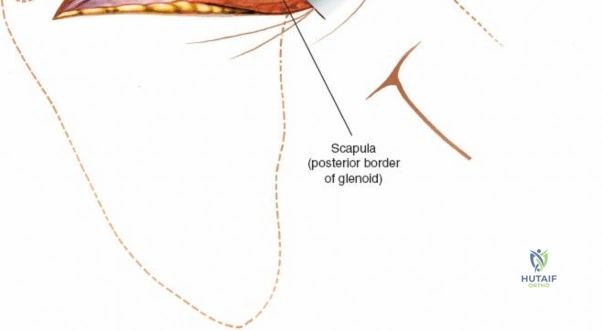
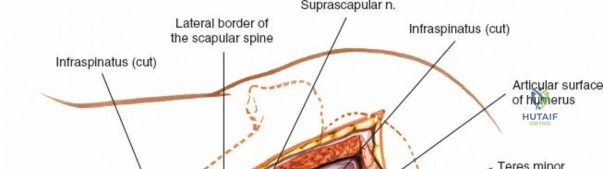
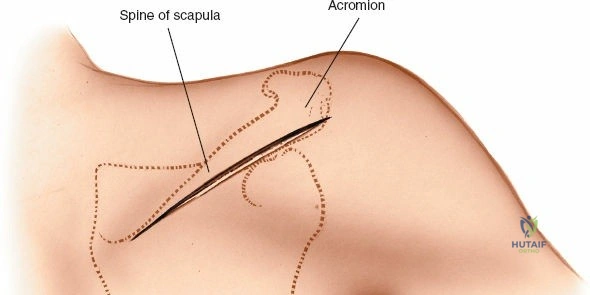
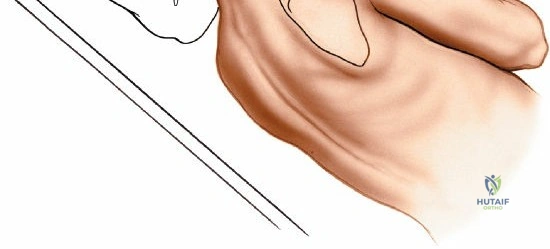
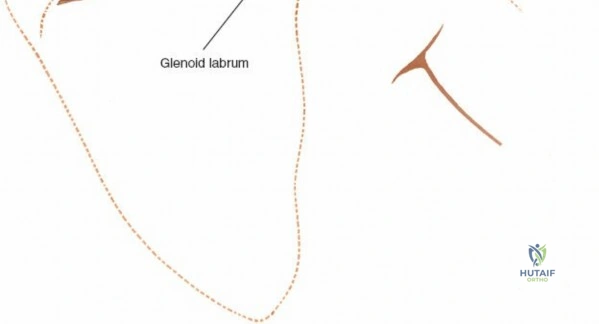
The primary bony landmarks defining the posterior shoulder are the acromion, the spine of the scapula, the medial border of the scapula, and the posterolateral corner of the acromion. The spine of the scapula extends obliquely from the medial border laterally to form the acromion, providing a crucial landmark for the surgical incision and potential deltoid detachment. The glenoid itself, a shallow piriform fossa, is key, with its posterior aspect being the target of many indications for this approach.
The proximal humerus, specifically the humeral head, anatomical neck, and greater tuberosity, are intimately involved, particularly in fracture-dislocation scenarios. The posterior glenoid rim is relatively deficient compared to the anterior rim, making it susceptible to shear fractures during posterior dislocation events.
Muscular Layers and Dissection Planes
The posterior shoulder is covered by several distinct muscle layers that must be sequentially addressed.
The superficial layer is formed by the deltoid muscle. Its posterior fibers originate from the inferior lip of the crest of the scapular spine and converge to insert on the deltoid tuberosity of the lateral humerus. The standard posterior approach involves splitting the posterior deltoid fibers in line with their orientation.
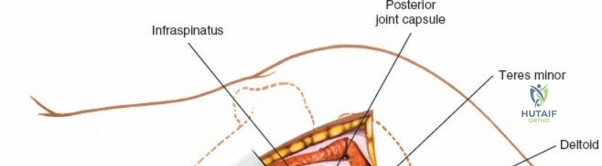
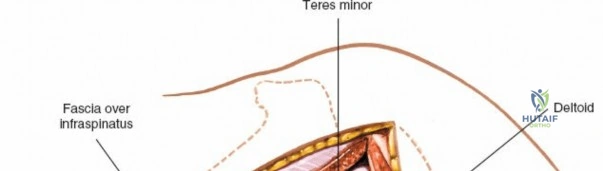
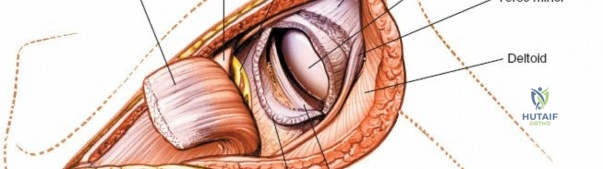
Beneath the deltoid, the deep layer consists of the posterior rotator cuff muscles. For the posterior approach, the infraspinatus and teres minor are of primary importance. The infraspinatus originates from the infraspinous fossa and inserts onto the middle facet of the greater tuberosity. The teres minor originates from the superior two-thirds of the lateral border of the scapula and inserts onto the inferior facet of the greater tuberosity. These two muscles contribute to external rotation and lie directly over the posterior capsule.

The interval between the infraspinatus and teres minor can be a useful plane for capsular access. However, a trans-tendinous split of the infraspinatus or a tenotomy is more commonly employed for wider exposure of the glenoid face.
Critical Neurovascular Structures
Precise knowledge of neurovascular structures is critical to avoid catastrophic iatrogenic injury during deep dissection and retraction.
The axillary nerve originates from the posterior cord of the brachial plexus (C5-C6) and courses anterior to the subscapularis before passing posteriorly through the quadrangular space. The boundaries of the quadrangular space are the teres minor (superior), teres major (inferior), long head of the triceps (medial), and the surgical neck of the humerus (lateral). The nerve lies approximately 5 centimeters distal to the posterolateral corner of the acromion. Splitting the deltoid further distal than this 5-centimeter safe zone risks denervating the posterior and middle heads of the deltoid.

The suprascapular nerve (C5-C6) passes through the suprascapular notch, innervates the supraspinatus, and then courses around the base of the scapular spine through the spinoglenoid notch to innervate the infraspinatus. The nerve is tethered at the spinoglenoid notch and is highly vulnerable to traction injuries during vigorous medial retraction of the infraspinatus muscle belly. Safe dissection requires remaining lateral to the spinoglenoid notch, typically staying within 1 to 1.5 centimeters of the glenoid rim when releasing the posterior capsule.
Indications and Contraindications
The decision to utilize an open posterior approach must be carefully weighed against the capabilities of modern arthroscopy. The open approach is reserved for pathology that physically cannot be managed through arthroscopic portals due to the need for large structural grafts, extensive hardware placement, or en bloc resections.
Primary indications include the management of chronic, locked posterior shoulder dislocations, particularly those associated with large reverse Hill-Sachs lesions (anteromedial humeral head impaction fractures). When the reverse Hill-Sachs lesion involves more than 20 to 25 percent of the articular surface, a McLaughlin procedure (transfer of the subscapularis tendon into the defect) or a Neer modification (transfer of the lesser tuberosity with the subscapularis) is indicated. While the anterior approach is used for the transfer itself, a posterior approach is often required simultaneously to disimpact the humeral head from the posterior glenoid rim and address posterior capsulolabral structures.
Posterior glenoid bone loss exceeding 20 percent, often seen in recurrent posterior instability or dysplasia, requires structural bone grafting. Open posterior bone block procedures, utilizing iliac crest or distal tibial allograft, provide rigid fixation and anatomical restoration of the articular arc. Furthermore, intra-articular fractures of the posterior glenoid with significant displacement require open reduction and internal fixation via this approach.

Contraindications are generally relative but include medically unstable patients, active localized soft tissue infection (unless the approach is specifically for irrigation and debridement), and pathology that is readily addressable via arthroscopy.
Operative vs Non Operative Indications Matrix
| Clinical Scenario | Operative Indication (Posterior Approach) | Non-Operative Management |
|---|---|---|
| Acute Posterior Dislocation | Irreducible by closed means; associated displaced posterior glenoid fracture > 5mm. | Successful closed reduction; stable shoulder post-reduction. |
| Chronic Locked Posterior Dislocation | Joint locked > 3 weeks; Reverse Hill-Sachs > 20% articular surface. | Elderly, low-demand patient with minimal pain and acceptable functional ROM. |
| Posterior Glenoid Bone Loss | > 20% bone loss with recurrent instability (Bone block required). | < 15% bone loss (amenable to arthroscopic labral repair). |
| Scapular Tumors | Neoplasm involving posterior glenoid neck or body requiring excision. | Benign, asymptomatic, non-progressive lesions (e.g., small osteochondroma). |
| Posterior Glenoid Fracture | Displaced > 5mm or involving > 20% of articular surface. | Minimally displaced fractures with a congruous joint. |
Pre Operative Planning and Patient Positioning
Thorough preoperative planning is essential for a successful posterior approach. Standard radiographic evaluation must include a true anteroposterior (Grashey) view, a scapular Y view, and an axillary lateral view. The axillary view is paramount for assessing the concentricity of the glenohumeral joint and identifying posterior subluxation, dislocation, or posterior glenoid rim fractures.
Advanced imaging is routinely required. Computed Tomography (CT) with 3D reconstructions is the gold standard for quantifying glenoid bone loss, assessing fracture morphology, and measuring the exact size and depth of a reverse Hill-Sachs lesion. Magnetic Resonance Imaging (MRI) is utilized to evaluate the integrity of the posterior rotator cuff, the posterior labrocapsular complex, and the presence of paralabral cysts compressing the suprascapular nerve at the spinoglenoid notch.

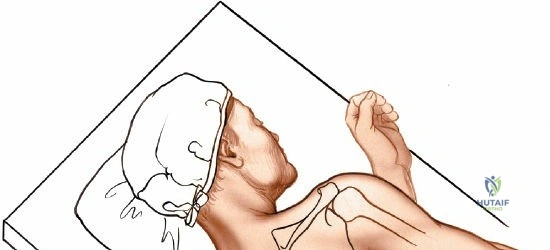
Patient positioning is a critical step that dictates the ease of exposure. The lateral decubitus position is almost universally preferred for the open posterior approach. The patient is placed on a bean bag with an axillary roll placed under the contralateral axilla to protect the dependent brachial plexus. All bony prominences must be meticulously padded.
The operative arm is draped free to allow for full manipulation during the procedure. An articulated arm positioner (e.g., Spider arm or TRIMANO) can be highly beneficial for maintaining specific degrees of abduction and internal/external rotation, which dynamically alter the tension on the posterior structures and assist in exposure. Alternatively, the arm can be rested over a sterile Mayo stand. The surgeon typically stands posterior to the patient, with the assistant positioned anteriorly or superiorly.

Detailed Surgical Approach and Technique
The classic posterior approach (often referred to as the Judet approach or variations thereof) provides extensile access to the posterior shoulder.
Superficial Dissection and Deltoid Split
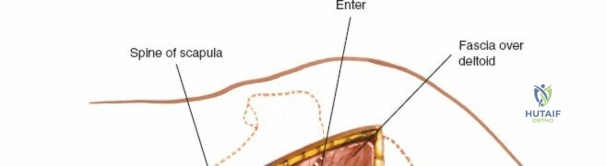
The skin incision is typically made in a vertical or slightly oblique fashion. It begins at the posterolateral corner of the acromion and extends distally toward the posterior axillary fold for approximately 8 to 10 centimeters. Subcutaneous tissues are dissected to expose the deep fascia overlying the posterior deltoid.

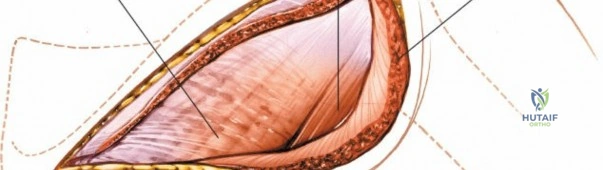
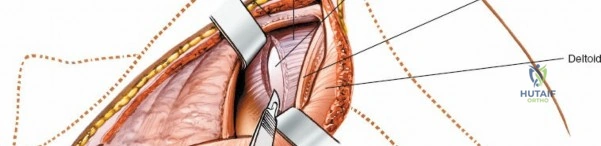
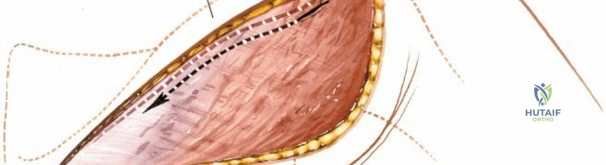
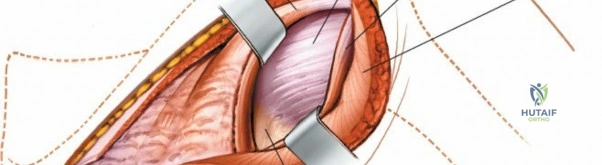
The posterior deltoid fibers are identified by their distinct longitudinal orientation. A split is made in the deltoid fascia, and the muscle fibers are bluntly separated using a periosteal elevator or the surgeon's fingers. It is imperative that this split does not extend further than 5 centimeters distal to the acromial edge to prevent injury to the axillary nerve, which traverses horizontally on the deep surface of the deltoid.
Once the split is developed, a self-retaining retractor (such as a Charnley or Gelpi) is placed. The subdeltoid bursa is then excised to clearly visualize the underlying posterior rotator cuff musculature.
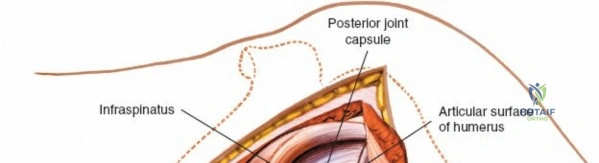
Deep Dissection and Rotator Cuff Management
With the deltoid retracted, the infraspinatus and teres minor muscles are exposed. The internervous plane between the infraspinatus (suprascapular nerve) and teres minor (axillary nerve) can be utilized. This plane is identified by a fat stripe and the differing fiber orientations. However, this interval is often narrow and can limit access to the superior aspect of the posterior glenoid.
More commonly, a trans-tendinous approach is utilized. The infraspinatus tendon is identified. A vertical tenotomy is performed approximately 1.5 to 2 centimeters medial to its insertion on the greater tuberosity. Alternatively, a horizontal split in line with the infraspinatus fibers can be performed, followed by subperiosteal elevation of the muscle belly from the posterior capsule.
When retracting the infraspinatus medially, the surgeon must be acutely aware of the suprascapular nerve at the spinoglenoid notch. Retractors must be placed carefully, avoiding deep, medial placement on the scapular neck.
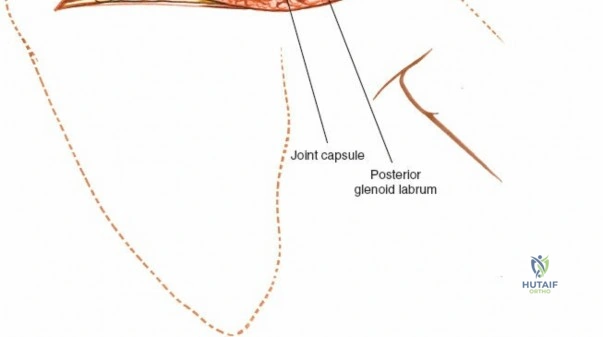
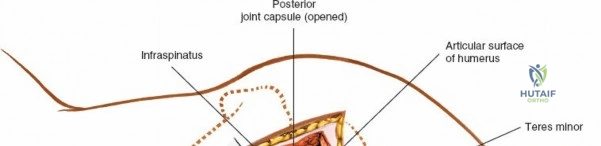
Capsulotomy and Joint Exposure
Once the posterior capsule is exposed, a capsulotomy is performed. The type of capsulotomy depends on the pathology. For a posterior bone block or capsulorrhaphy, a vertical capsulotomy is made parallel to the glenoid rim, approximately 5 to 10 millimeters lateral to the labrum.
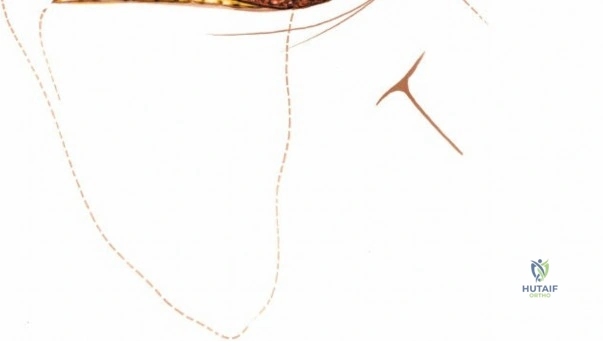
If extensive exposure of the humeral head is required (e.g., for addressing a large reverse Hill-Sachs lesion), a T-shaped capsulotomy can be utilized, with the horizontal limb extending laterally along the inferior margin of the infraspinatus. Stay sutures are immediately placed in the capsular flaps to maintain control and facilitate later repair.

A Fukuda retractor or a blunt Hohmann retractor is placed into the joint to subluxate the humeral head anteriorly, thereby providing a direct, en face view of the posterior glenoid articulation.
Osseous Management and Fixation
For posterior glenoid fractures, the fracture site is debrided of hematoma and interposed tissue. Anatomic reduction is achieved using dental picks and provisional Kirschner wires. Fixation is typically accomplished with 2.7mm or 3.5mm lag screws, or a specialized posterior glenoid buttress plate if comminution is present.
For posterior instability with bone loss, the posterior glenoid neck is decorticated to a bleeding bed. The structural bone graft (iliac crest or distal tibia) is contoured to match the defect and restore the articular arc. The graft is positioned flush with the articular cartilage and secured with two cannulated screws (typically 3.5mm or 4.0mm) placed parallel to the articular surface.

Closure Techniques
Following the osseous procedures, meticulous closure is mandatory to restore posterior stability. The posterior capsule is repaired using non-absorbable sutures. If a capsular shift is required, the inferior flap is advanced superiorly and medially.
The infraspinatus tenotomy or split is repaired using heavy non-absorbable sutures in a figure-of-eight or Krakow fashion. The deltoid split is loosely approximated to prevent muscle herniation, but tight closure of the fascia is avoided to prevent compartment syndrome of the deltoid. Subcutaneous tissues and skin are closed in a standard layered fashion.
Complications and Management
The posterior approach carries specific risks due to the proximity of critical neurovascular structures and the inherent challenges of posterior shoulder stabilization.
Neurologic injury is the most feared complication. The axillary nerve is at risk during the distal extent of the deltoid split and during inferior capsular release. The suprascapular nerve is at risk during medial retraction of the infraspinatus and during placement of drills or screws into the posterior glenoid neck. If a screw is directed too medially or superiorly, it can penetrate the spinoglenoid notch.
Hardware complications include screw prominence leading to articular cartilage damage or graft osteolysis. Recurrent instability can occur if the bone graft resorbs, if the capsular repair fails, or if an unrecognized anterior pathology (such as an anterior labral tear) was not addressed. Postoperative stiffness, particularly a loss of internal rotation, is common due to scarring of the posterior capsule and infraspinatus.
Common Complications and Salvage Strategies
| Complication | Estimated Incidence | Prevention and Salvage Strategies |
|---|---|---|
| Axillary Nerve Injury | 1% - 3% | Prevention: Limit deltoid split to <5cm from acromion. Stay superior to teres minor lower border. Salvage: Observation with EMG at 3 months; nerve exploration/grafting if no recovery. |
| Suprascapular Nerve Injury | 2% - 5% | Prevention: Avoid vigorous medial retraction of infraspinatus. Direct drills/screws parallel to joint line, not medially. Salvage: Hardware removal if impingement is confirmed on imaging. |
| Recurrent Posterior Instability | 5% - 15% | Prevention: Accurate assessment of bone loss; rigid graft fixation; robust capsulorrhaphy. Salvage: Revision bone block; consider revision to arthroplasty in older patients. |
| Postoperative Stiffness (Loss of IR) | 10% - 20% | Prevention: Avoid over-tensioning the posterior capsule during repair. Early supervised passive ROM. Salvage: Aggressive physical therapy; arthroscopic capsular release if refractory >6 months. |
| Hardware Prominence / Chondrolysis | 2% - 5% | Prevention: Countersink screw heads into the bone graft. Ensure screws are extra-articular under direct vision and fluoroscopy. Salvage: Prompt hardware removal; chondroplasty. |
Post Operative Rehabilitation Protocols
Rehabilitation following an open posterior approach is highly dependent on the specific procedure performed (e.g., fracture fixation vs. bone block stabilization). However, a general phased approach is universally applied to protect the posterior soft tissue repair while preventing catastrophic stiffness.

Phase 1: Protection Phase (Weeks 0 to 6)
The shoulder is immobilized in a specialized orthosis. Unlike anterior stabilization which utilizes an internal rotation sling, posterior stabilization requires immobilization in neutral to slight external rotation (10 to 15 degrees) and slight abduction. A "gunslinger" brace or a modified airplane splint is often utilized.
Passive range of motion (PROM) is initiated early to prevent adhesions, but strict limits are enforced. Forward elevation is typically allowed up to 90 degrees. Internal rotation is strictly prohibited or limited to neutral to protect the posterior capsular repair and infraspinatus reattachment.
Phase 2: Intermediate Phase (Weeks 6 to 12)
Immobilization is discontinued. Active-assisted range of motion (AAROM) transitions to active range
Clinical & Radiographic Imaging

