Arthroscopic Management of Shoulder Throwing Injuries: A Masterclass in Glenohumeral Biomechanics and Repair

Key Takeaway
Join us in the OR for an immersive masterclass on arthroscopic management of throwing shoulder injuries. We'll meticulously address PIGHL contracture, SLAP tears, and rotator cuff pathology. This session covers comprehensive anatomy, precise intraoperative techniques, and critical pearls for restoring function in elite athletes. Learn patient positioning, portal placement, diagnostic arthroscopy, and advanced repair strategies for optimal outcomes.
Comprehensive Introduction and Patho-Epidemiology
The management of the overhead throwing athlete’s shoulder represents one of the most formidable challenges in modern orthopaedic sports medicine. The throwing motion is a biomechanical enigma—a violent, highly coordinated kinetic chain event that generates extreme angular velocities exceeding 7,000 degrees per second. This chapter delves into the intricate and biomechanically demanding arena of the throwing shoulder. Treating these athletes is rarely about repairing a single, isolated torn structure; rather, it requires a profound understanding of a complex kinematic sequence, the repetitive, high-magnitude forces involved, and how these unique stresses precipitate a highly predictable constellation of injuries. Our ultimate objective is not mere anatomical restoration, but the functional resurrection of the athlete’s ability to compete at their premorbid level of elite performance.
Throwers—whether baseball pitchers, javelin throwers, or elite volleyball attackers—subject their shoulder girdles to immense, repetitive cyclical loading. This chronic stress, particularly during the violent deceleration phase immediately following ball release, routinely leads to fatigue, microtrauma, and eventual weakening of the posterior shoulder musculature. Over time, this chronic muscular imbalance and repetitive microtrauma precipitate two primary, intimately related, and often insidious pathologic entities: scapular dyskinesis and posteroinferior glenohumeral ligament (PIGHL) contracture. The epidemiology of these injuries skews heavily toward the adolescent and young adult overhead athlete, with prevalence rates of labral and rotator cuff pathology approaching 50-70% in asymptomatic professional pitchers, underscoring the concept that structural alteration is an expected adaptation to throwing.
The clinical manifestation of this biomechanical cascade is frequently termed the "dead arm syndrome." In this state, the athlete experiences vague, deep posterosuperior shoulder discomfort associated with the act of throwing, leading to a precipitous loss of pitch velocity, diminished command of the strike zone, and an inability to warm up effectively. Unlike traumatic anterior instability seen in contact athletes, the throwing shoulder suffers from acquired microinstability. The delicate balance between the extreme external rotation required to generate velocity and the static/dynamic stability required to maintain joint congruity is lost.
Understanding the patho-epidemiology of the thrower's shoulder necessitates a paradigm shift from traditional orthopaedic thinking. We are not treating a discrete traumatic event, but rather the failure of a biological system to adapt to supraphysiologic stress. The structural lesions we identify on magnetic resonance imaging (MRI) or during diagnostic arthroscopy—such as Superior Labrum Anterior and Posterior (SLAP) tears or articular-sided partial rotator cuff tears—are frequently the end-stage victims of this altered biomechanical environment, not the primary culprits. Therefore, surgical intervention must be meticulously tailored to address both the structural damage and the underlying biomechanical deficits.
Detailed Surgical Anatomy and Biomechanics
A rigorous comprehension of the surgical anatomy and the altered biomechanics of the thrower's shoulder is the bedrock of successful management. Eighteen distinct muscles attach to the scapula, orchestrating its position and movement on the thoracic wall. These periscapular stabilizers—chiefly the trapezius, rhomboids, levator scapulae, serratus anterior, and pectoralis minor—are the foundation of normal glenohumeral rhythm. Alterations in their activation patterns or strength deficits lead to scapular dyskinesis, which functionally alters the orientation of the glenoid during the throwing motion, thereby increasing the shear forces across the anterior capsule and superior labrum.
The dynamic stability of the glenohumeral joint is governed by the rotator cuff (supraspinatus, infraspinatus, teres minor, and subscapularis) and the long head of the biceps (LHB) tendon. In the thrower, the posterior cuff (infraspinatus and teres minor) is subjected to massive eccentric loads during the deceleration phase, often leading to reactive hypertrophy, stiffness, and eventual failure. The LHB tendon, originating from the supraglenoid tubercle and the superior labrum, acts as a critical dynamic depressor of the humeral head and a decelerator of the arm. Its structural integrity and the stability of its anchor are central to the pathogenesis of SLAP lesions in this demographic.
The static stability of the joint is provided by the glenohumeral joint capsule, reinforced by the superior, middle, and inferior glenohumeral ligaments (SGHL, MGHL, IGHL). The Inferior Glenohumeral Ligament Complex (IGHL) is of paramount importance in the thrower. It comprises an anterior band (AIGHL), a posterior band (PIGHL), and an interposed axillary pouch. As the arm is brought into maximum abduction and external rotation (ABER)—the late cocking phase of throwing—the PIGHL dynamically shifts from its posteroinferior resting position to a directly inferior (6 o’clock) position relative to the glenoid.
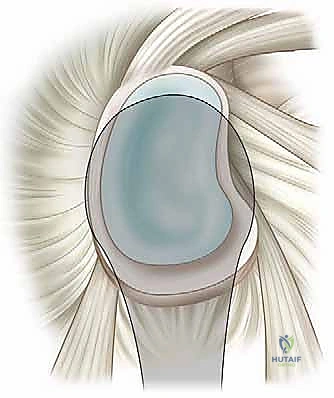
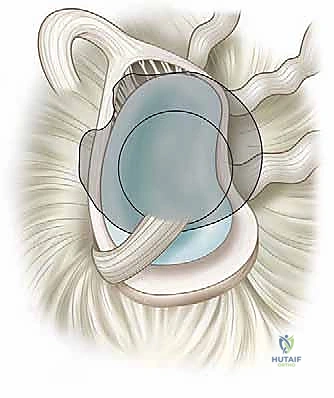
In a shoulder afflicted by PIGHL contracture—a maladaptive fibroblastic thickening in response to chronic tensile stress (Wolf’s law of collagen)—this contracted ligament occupies the space directly inferior to the humeral head in the ABER position. This effectively acts as a fulcrum, tethering the humeral head posteriorly and forcing it superiorly. This posterosuperior shift alters the normal, centered glenohumeral contact point, initiating a catastrophic biomechanical cascade.


This shift creates an abnormal, posteriorly directed force vector and severe torsional stress on the biceps anchor, leading to the classic "peel-back" mechanism. The biceps anchor fails and peels back medially over the posterosuperior glenoid rim, creating a Type II SLAP tear (specifically the posterior or anterior-posterior subtypes). Concurrently, the posterosuperior translation causes the articular surface of the supraspinatus and infraspinatus to abut against the posterosuperior glenoid rim (internal impingement), leading to partial articular-sided tendon avulsion (PASTA) lesions. Finally, because the humeral head is shifted posterosuperiorly, the anterior capsule becomes relatively slack. Repeated hyperexternal rotation stretches this attenuated tissue, leading to "pseudo-laxity" and, eventually, tertiary anterior microinstability.
Exhaustive Indications and Contraindications
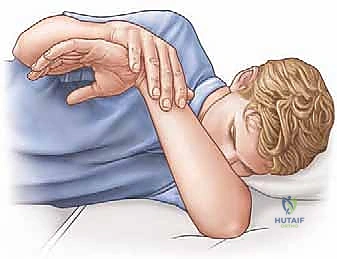
The decision to proceed with operative intervention in the overhead throwing athlete is one of the most nuanced in sports medicine. Surgery should never be the first line of treatment for the thrower's shoulder, barring an acute, catastrophic traumatic event. A mandatory, highly supervised, and thrower-specific non-operative rehabilitation program must be exhausted prior to considering arthroscopy. This program must focus meticulously on restoring the total mobility arc, stretching the contracted posterior capsule (via sleeper stretches and cross-body adduction), and aggressively rehabilitating periscapular muscular imbalances.
Indications for surgical intervention are strictly reserved for athletes who have failed a comprehensive, compliance-verified non-operative program lasting a minimum of 3 to 6 months. The athlete must demonstrate persistent, unacceptable pain during the throwing motion, a documented and sustained loss of pitch velocity or control, and an inability to compete at their desired level. Furthermore, these subjective complaints must correlate precisely with objective clinical findings (such as a persistent Glenohumeral Internal Rotation Deficit [GIRD] > 20 degrees that is refractory to stretching) and advanced imaging confirming structural pathology like a SLAP tear or a high-grade partial rotator cuff tear. Mechanical symptoms, such as painful catching or popping during the acceleration phase, further strengthen the indication for arthroscopic evaluation and repair.
Contraindications to surgery are equally critical to recognize. The most absolute contraindication is the presence of asymptomatic structural abnormalities on MRI. As previously noted, adaptive changes (including labral fraying and partial cuff tearing) are ubiquitous in elite throwers; operating on an MRI finding rather than a clinical syndrome is a guaranteed path to a poor outcome. Furthermore, patients who have not fully complied with or attempted a rigorous physical therapy protocol are poor surgical candidates. Severe glenohumeral osteoarthritis, though rare in young throwers, is a contraindication to isolated soft-tissue repair. Finally, a lack of patient understanding regarding the guarded prognosis and the grueling, year-long postoperative rehabilitation required to return to elite throwing should preclude surgical intervention.
| Parameter | Indications for Arthroscopic Intervention | Contraindications to Surgery |
|---|---|---|
| Clinical History | Failure of 3-6 months of targeted physical therapy; persistent "dead arm" syndrome; inability to throw at premorbid velocity. | Lack of dedicated conservative trial; non-compliant patient; asymptomatic patient with incidental MRI findings. |
| Physical Exam | Refractory GIRD > 20 degrees; positive Modified Jobe Relocation or O'Brien's test; profound, uncorrectable scapular dyskinesis. | Painless, full range of motion; lack of localized posterosuperior joint line tenderness in ABER. |
| Imaging (MRA) | Distinct Type II SLAP tear (peel-back); >50% articular-sided rotator cuff tear; discrete Bankart lesion (if secondary instability is present). | Mild labral fraying; low-grade (<25%) partial cuff tears; severe glenohumeral osteoarthritis. |
| Patient Factors | Elite athlete with realistic expectations and commitment to a 9-12 month postoperative rehabilitation protocol. | Recreational athlete unwilling to complete rehab; patients seeking a "quick fix" for throwing mechanics. |
Pre-Operative Planning, Templating, and Patient Positioning
Meticulous preoperative planning is the distinguishing factor between a master surgeon and a technician. The evaluation begins with a granular patient history. Pitchers will frequently describe a progressive loss of control and decreased velocity that initially occurs without significant pain. As the pathology progresses, pain becomes prominent during the late cocking and early acceleration phases, localized deep within the posterosuperior shoulder.
Physical examination must be exhaustive. Scapular dyskinesis is evaluated by observing the patient from behind during active elevation and descent of the arms. We look for the "SICK" scapula syndrome (Scapular malposition, Inferior medial border prominence, Coracoid pain and malposition, and dysKinesis of scapular movement). Glenohumeral range of motion must be measured with the scapula rigidly stabilized to isolate true glenohumeral motion. We calculate GIRD by subtracting the internal rotation of the throwing shoulder from the non-throwing shoulder. A GIRD exceeding 20 degrees, combined with a loss of the Total Mobility Arc (TMA), indicates a shoulder at significant risk. Specific provocative maneuvers, such as the Modified Jobe Relocation Test (which reproduces deep posterior pain in the ABER position that is relieved by a posteriorly directed force on the humerus) and O’Brien’s Active Compression Test, are utilized to isolate superior labral pathology.

High-resolution Magnetic Resonance Arthrography (MRA) is the imaging modality of choice. The intra-articular contrast distends the capsule, allowing for superior visualization of undersurface rotator cuff tears, capsular attenuation, and the precise morphology of SLAP lesions. Imaging the shoulder in the ABER position can dynamically demonstrate the peel-back of the labrum and the internal impingement of the rotator cuff against the glenoid rim.
For surgical execution, the beach chair position is overwhelmingly preferred for the throwing athlete. This orientation provides unparalleled access to both the anterior and posterior compartments, facilitates an anatomical understanding of the joint in an upright posture, and allows for unimpeded dynamic assessment of the arm during the procedure. The patient is positioned at a 60-70 degree incline. Crucially, the head and neck must be secured in a neutral posture using a well-padded headrest. Excessive lateral flexion or rotation of the cervical spine can place catastrophic traction on the upper trunk of the brachial plexus, leading to devastating postoperative neuropraxia. The operative arm is draped free to allow for full, unconstrained movement through abduction, external rotation, and internal rotation, permitting the surgeon to dynamically recreate the peel-back mechanism intraoperatively.


Step-by-Step Surgical Approach and Fixation Technique
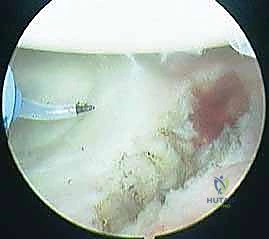
The arthroscopic management of the thrower's shoulder requires technical precision and a profound respect for tissue tension. Over-constraining the joint is a career-ending error. The procedure commences with the establishment of a standard posterior viewing portal, placed slightly more superior and lateral than usual to optimize the trajectory for evaluating the superior labrum and posterior cuff. An anterior mid-glenoid portal is established via an outside-in technique using a spinal needle, ensuring the trajectory passes safely through the rotator interval, superior to the subscapularis tendon and lateral to the conjoined tendon.
A systematic 15-point diagnostic arthroscopy is performed. The surgeon must dynamically evaluate the biceps anchor by taking the arm out of traction and placing it into the ABER position. This maneuver will visually reproduce the "peel-back" sign, confirming the functional instability of the Type II SLAP lesion. The articular surface of the rotator cuff is meticulously probed for PASTA lesions, and the capsule is evaluated for anterior pseudo-laxity and posterior contracture.




If a refractory PIGHL contracture is identified and correlates with preoperative GIRD, an arthroscopic posterior capsular release is indicated. Using a radiofrequency ablation wand or arthroscopic scissors, the capsule is carefully divided from the 6 o'clock to the 9 o'clock position (in a right shoulder). The release must be performed approximately 1 cm lateral to the glenoid labrum to avoid catastrophic injury to the axillary nerve, which runs intimately close to the inferior capsule.


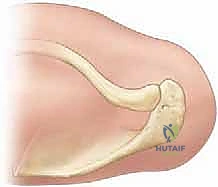

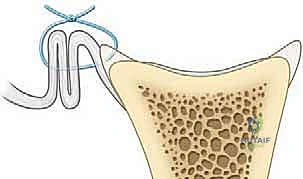
For the SLAP repair, the superior glenoid neck is debrided of fibrous tissue down to a bleeding bony bed using an arthroscopic elevator and a motorized burr. Care is taken not to decorticate excessively, which could compromise anchor purchase. Typically, one or two small-diameter (e.g., 2.4mm or 2.9mm) biocomposite or all-suture anchors are placed at the 11 o'clock and 1 o'clock positions. The trajectory of the drill is critical; it must be directed medially and slightly inferiorly to safely engage the dense bone of the supraglenoid tubercle without penetrating the articular cartilage.







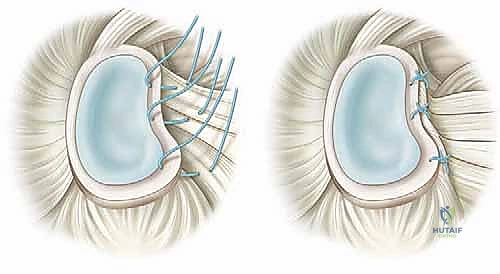
Suture management is performed using a shuttle relay technique. Simple sutures are generally preferred over mattress configurations to avoid strangulating the labral tissue and over-constraining the biceps root. The knots are tied securely, ensuring the labrum is anatomically reduced against the glenoid rim, effectively neutralizing the peel-back mechanism.







Management of concomitant partial articular-sided rotator cuff tears adheres to the "50% rule." Tears involving less than 50% of the tendon thickness are typically treated with aggressive arthroscopic debridement to stimulate a healing response. High-grade tears (>50%) in the elite thrower present a profound dilemma. Takedown and formal repair often result in unacceptable stiffness. Therefore, a transtendon, in situ repair technique using a knotless anchor is frequently employed to secure the articular leaf without violating the intact bursal fibers, thereby preserving the native biomechanical length-tension relationship of the cuff.



Complications, Incidence Rates, and Salvage Management
Surgical intervention in the throwing shoulder is fraught with potential complications, the most devastating of which is postoperative stiffness. The loss of even 5 to 10 degrees of extreme external rotation can completely ablate a pitcher's ability to generate elite-level velocity, effectively ending their career. Over-tensioning the SLAP repair, over-plicating the anterior capsule, or failing to address the PIGHL contracture are the primary iatrogenic causes of this stiffness.
Failure to return to premorbid levels of play is a highly recognized "complication" in this demographic. Historically, return-to-play (RTP) rates for elite pitchers following isolated SLAP repairs have been guarded, hovering between 50% and 65%. This underscores the reality that structural repair does not guarantee functional restoration if the underlying kinetic chain deficits remain uncorrected. Recurrent pain, often due to failure of the anchor construct, persistent internal impingement, or progressive rotator cuff tearing, requires a comprehensive re-evaluation of the athlete's mechanics and structural integrity.
Neurologic injuries, while rare, are catastrophic. The axillary nerve is at extreme risk during a posterior capsular release. The surgeon must maintain a strict 1 cm margin lateral to the labrum and utilize radiofrequency devices with extreme caution, as thermal spread can induce neuropraxia. Brachial plexus injuries, typically involving the upper trunk, are almost exclusively related to improper
