

Comprehensive Introduction and Patho-Epidemiology
Welcome, fellows, to the operating theater. Today, we are addressing a challenging yet profoundly rewarding pathology: posterior shoulder instability. While significantly less common than its anterior counterpart—comprising roughly 2% to 10% of all documented shoulder instability presentations—posterior instability, if left untreated or misdiagnosed, can lead to debilitating pain, profound functional impairment, and the premature onset of glenohumeral osteoarthritis. Our overarching objective is to meticulously restore the static stabilizers of the shoulder using an advanced all-arthroscopic approach, ensuring both biomechanical stability and a definitive return to high-level function for our patient.
Historically, posterior instability was frequently missed on initial clinical evaluation, often masquerading as generalized shoulder pain or rotator cuff pathology. The pathophysiology typically bifurcates into two distinct mechanisms: macrotrauma and repetitive microtrauma. Macrotraumatic events, such as high-energy motor vehicle collisions, electrocution, or violent seizures, generate massive axial loads on an internally rotated, adducted arm, frequently resulting in frank posterior dislocation and profound capsulolabral tearing. Conversely, the microtraumatic etiology is insidious, predominantly affecting athletes such as offensive linemen, weightlifters, and overhead throwers. In throwers, the extreme deceleration forces encountered during the follow-through phase of the throwing motion place immense repetitive stress on the posterior capsuloligamentous complex.
Over time, this repetitive microtrauma induces plastic deformation and attenuation of the posterior capsule, culminating in recurrent posterior subluxation rather than frank dislocation. Patients typically present with a deep, poorly localized posterior shoulder pain that is dramatically exacerbated in provocative positions. It is crucial to differentiate between a true locked posterior dislocation, which may necessitate open reduction or structural bone grafting, and chronic recurrent subluxation, which is highly amenable to arthroscopic capsulolabral reconstruction.
While arthroscopic treatment has revolutionized our ability to alleviate symptoms and restore native joint kinematics, it is incumbent upon us as surgeons to recognize the limitations of our interventions. Current long-term longitudinal data do not definitively prove that soft-tissue stabilization completely arrests the development of osteoarthritis, particularly if chondral damage or significant glenoid retroversion is already present. Therefore, early recognition, precise diagnosis, and meticulous surgical execution are paramount to altering the natural history of this complex condition.
Detailed Surgical Anatomy and Biomechanics
Fellows, a profound, three-dimensional understanding of glenohumeral anatomy is absolutely non-negotiable for successful arthroscopic surgery. The shoulder joint is an inherently unstable articulation, relying on a delicate interplay between static and dynamic stabilizers to maintain the humeral head centered within the shallow glenoid fossa. The primary static stabilizers include the articular congruity of the osseous structures, the capsuloligamentous complex, and the glenoid labrum. The dynamic stabilizers encompass the rotator cuff musculature, the periscapular stabilizers, and the intra-articular portion of the long head of the biceps tendon.
The posterior capsule and its associated labral complex are the primary anatomical structures implicated in posterior instability. Histologically and macroscopically, the posterior capsule is relatively thin and diaphanous compared to the robust anterior capsule. It is composed primarily of radial and circular collagen fibers with minimal cross-linking, rendering it inherently less resistant to immense shear forces. The glenohumeral ligaments play a synergistic role depending on arm position. With the arm forward-flexed to 90 degrees, the subscapularis tendon and the superior glenohumeral ligament provide significant stability against posterior translation. As the arm moves into a neutral position, the coracohumeral ligament assumes a greater stabilizing role.
However, it is in the position of internal rotation, flexion, and adduction—the classic mechanism of injury—that the inferior glenohumeral ligament (IGHL) complex becomes paramount. Specifically, the posterior band of the IGHL acts as the primary restraint to posterior humeral head translation. During our arthroscopic repair, our primary biomechanical objective will be to restore anatomic tension to this critical structure, often requiring a substantial capsular shift to eliminate pathologic capsular redundancy. The labrum itself functions as a vital "chock-block," deepening the glenoid socket by up to 50%. Avulsion of the posterior labrum (a reverse Bankart lesion) catastrophically compromises this chock-block effect.
Osteology and neurovascular anatomy must be meticulously respected. Pathologic glenoid retroversion (greater than 10 degrees) or glenoid hypoplasia severely predisposes a patient to posterior instability and may precipitate failure of isolated soft-tissue repairs. On the humeral side, a reverse Hill-Sachs lesion—an anteromedial humeral head impression fracture—indicates significant macroinstability. Critically, the axillary nerve and the posterior humeral circumflex artery are at extreme risk during posterior portal placement and inferior capsular release. The axillary nerve traverses the quadrangular space, intimately wrapping around the surgical neck of the humerus typically 5 to 7 centimeters inferior to the posterolateral acromion. The suprascapular nerve, coursing through the spinoglenoid notch approximately 1 to 2 centimeters medial to the posterior glenoid rim, can be injured by overly aggressive medial anchor placement or excessive traction.
Comprehensive Clinical Evaluation and Diagnostic Imaging
A meticulous, deeply investigative history is the cornerstone of diagnosis. We must ascertain whether the patient has experienced a definitive, locked dislocation requiring closed reduction in an emergency setting, or if their primary complaint is insidious pain exacerbated by specific kinematic chains. The classic provocative position involves shoulder flexion, adduction, and internal rotation—often described by patients as the "driving a car" position, pushing open a heavy door, or performing a bench press. We must rigorously document the onset, chronicity, severity, and functional impact of the symptoms. Crucially, surgical intervention is strictly reserved for patients who have demonstrably failed an exhaustive, well-structured trial of conservative management, specifically focusing on physical therapy to strengthen the periscapular stabilizers and the posterior rotator cuff.
On physical examination, we meticulously inspect for muscle atrophy, palpate for localized posterior joint line tenderness, and rigorously document both active and passive range of motion. Any restriction in internal rotation may indicate posterior capsular contracture, which paradoxically can coexist with instability. We must also perform a comprehensive assessment of impingement signs to rule out concomitant rotator cuff tendinopathy or internal impingement, which frequently confound the clinical picture in overhead athletes.
Specific provocative tests for posterior instability are mandatory. The Load and Shift Test assesses the absolute degree of pathologic translation; the humeral head is axially loaded into the glenoid and translated posteriorly, grading the subluxation. The Jerk Test involves applying an axial load to the humerus in 90 degrees of flexion and internal rotation, then horizontally adducting the arm; a positive test yields a palpable "clunk" as the subluxated humeral head reduces over the posterior glenoid rim. The Kim Test, performed by applying a posteroinferior directed force to the elevated and internally rotated arm, is highly sensitive for concealed posteroinferior labral tears. Finally, a rigorous Sulcus Sign Evaluation is critical; a positive sulcus sign indicating inferior humeral head translation suggests underlying multidirectional instability (MDI), which fundamentally alters our surgical algorithm.
Plain radiography remains the initial imaging modality of choice. A standard trauma series, including a true anteroposterior (Grashey), scapular Y, and axillary lateral view, is essential. The axillary lateral view is particularly critical for identifying posterior humeral head subluxation, glenoid dysplasia, or excessive retroversion.
FIG 1 • A. Axillary lateral radiograph demonstrating glenoid hypoplasia.
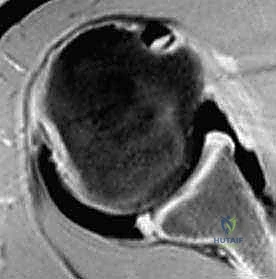
FIG 1 • A. Axillary lateral radiograph that demonstrates glenoid hypoplasia, which predisposes to posterior instability of the shoulder.
Despite the utility of plain films, Magnetic Resonance Arthrography (MRA) is the undisputed gold standard for visualizing the intricate posterior capsulolabral architecture. MRA allows for precise identification of posterior labral avulsions (reverse Bankart lesions), concealed intrasubstance labral tears (Kim lesions), and capsular stripping (POLPSA - Posterior Ligamentous Articular Sleeve Avulsion). Furthermore, MRA is highly sensitive for detecting Humeral Avulsion of the Glenohumeral Ligament (HAGL) lesions, which require a specific surgical approach.
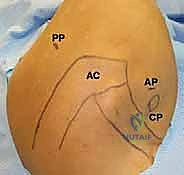
FIG 1 • B. Axial image from an MR arthrogram demonstrating a posterior labral lesion. Contrast can be seen between the posterior labrum and the articular margin of the glenoid, indicating a labral tear or avulsion.
Exhaustive Indications and Contraindications
The decision to proceed with operative intervention must be highly individualized, balancing the patient's functional demands, pathoanatomy, and psychological readiness. Arthroscopic posterior stabilization is a technically demanding procedure that requires strict adherence to indications to ensure optimal outcomes.
| Category | Specific Parameters |
|---|---|
| Absolute Indications | Recurrent, symptomatic posterior subluxation or dislocation refractory to a minimum of 3-6 months of targeted physical therapy. |
| Acute traumatic posterior dislocation with a massive, displaced posterior labral tear or concomitant osseous injury in a high-demand athlete. | |
| Symptomatic HAGL (Humeral Avulsion of Glenohumeral Ligament) lesion failing conservative care. | |
| Relative Indications | Chronic posterior shoulder pain in an overhead athlete with MRI-confirmed posteroinferior labral pathology (Kim lesion) and failed non-operative management. |
| Posterior instability with mild to moderate glenoid retroversion (<10 degrees) where soft tissue balancing may still suffice. | |
| Absolute Contraindications | Voluntary, habitual dislocators with underlying psychiatric overlay or secondary gain motives. |
| Active, untreated seizure disorders (high risk of catastrophic immediate post-operative failure). | |
| Massive posterior glenoid bone loss (>15-20%) or severe glenoid retroversion (>15 degrees) necessitating an open bone block procedure (e.g., posterior Latarjet or iliac crest graft). | |
| Relative Contraindications | Untreated, profound multidirectional instability (requires a global capsular shift, often open, rather than isolated posterior repair). |
| Poor patient compliance, rendering them unable to adhere to strict post-operative immobilization and rehabilitation protocols. |
Patients presenting with multidirectional instability must be approached with extreme caution. If a patient demonstrates a profound sulcus sign and global laxity, an isolated posterior repair will inevitably fail, as it does not address the underlying pan-capsular redundancy. In such cases, a comprehensive 270-degree or 360-degree arthroscopic capsular shift is mandated.
Pre-Operative Planning, Templating, and Patient Positioning
Before the patient ever breaches the threshold of the operating room, a meticulous review of all imaging studies is conducted. We determine the exact spatial orientation of the pathology, meticulously quantify any glenoid or humeral bone deficiency, identify intra-articular loose bodies, and map out our anchor trajectories.
Once the patient is successfully induced under general anesthesia, but strictly before any positioning or sterile prep, we perform a comprehensive Examination Under Anesthesia (EUA). This is an absolutely critical, non-skippable step. Without the confounding variable of patient muscle guarding, we can accurately assess the true magnitude and direction of instability. We perform a bilateral sulcus test, a rigorous load and shift test in multiple planes of elevation, and a manual circumduction test. The findings are meticulously compared to the awake examination and the contralateral, asymptomatic shoulder. This real-time biomechanical feedback directly dictates the volume of our capsular shift.
For arthroscopic posterior instability repair, we strongly advocate for the lateral decubitus position. While the beach-chair position is utilized by some, the lateral decubitus orientation provides vastly superior, unobstructed access to the posterior and inferior glenohumeral recesses. It allows for optimal visualization of the posterior labrum and facilitates the complex trajectory required for posteroinferior anchor placement.
Our setup is highly standardized to prevent catastrophic nerve palsies:
1. OR Table and Stabilization: The patient is carefully rolled onto an inflatable beanbag. The beanbag is molded to the patient's contours and rigidified via suction. Heavy-duty kidney rests are applied anteriorly and posteriorly at the level of the pelvis to prevent any rotational shifting during the procedure.
2. Meticulous Padding: This is the most critical step in positioning. A thick, specialized axillary roll is placed just caudal to the dependent axilla to offload the brachial plexus and prevent compression of the axillary neurovascular bundle. All bony prominences—specifically the dependent fibular head (common peroneal nerve), greater trochanter, and ulnar nerve—are heavily padded.
3. Traction Application: The operative arm is placed into a sterile traction sleeve and connected to a boom apparatus. We typically apply 10 to 15 pounds of traction, positioning the arm in 45 degrees of abduction and 20 degrees of forward flexion. This specific vector achieves optimal joint distraction, opening the posterior joint space and allowing our instruments to navigate without iatrogenic scuffing of the articular cartilage.
Step-by-Step Surgical Approach and Fixation Technique
We utilize a sophisticated all-arthroscopic technique, relying heavily on precise portal placement. Errant portals will exponentially increase the difficulty of the procedure and jeopardize the axillary nerve.
Portal Establishment and Diagnostic Arthroscopy
To facilitate initial trocar insertion, we distend the glenohumeral joint with 50 mL of sterile saline via an 18-gauge spinal needle directed posteriorly. This pushes the humeral head anteriorly, expanding the posterior recess.
Our standard viewing portal is the posterior portal. However, for posterior instability, we modify our landmarking. The portal is established 1 cm distal and 1 cm lateral to the traditional "soft spot" posterior portal. This slightly inferior and lateral trajectory is vital; it provides a superior angle of approach to the posterior glenoid rim, running parallel to the articular surface rather than perpendicular to it.

TECH FIG 1 • A. The posterior portal ( PP ) is marked in line with the lateral border of the acromion ( AC ).

TECH FIG 1 • B. Surface landmarks identify the posterior portal ( PP ), acromion ( AC ), anterior portal ( AP ), and coracoid process ( CP ).
Once the posterior cannula is established, we introduce the 30-degree arthroscope and perform a rapid, systematic diagnostic sweep of the joint. We evaluate the biceps root, the superior labrum, the anterior structures, and the rotator cuff. We then establish an anterior working portal via an inside-out technique, passing a switching stick through the rotator interval, strictly superior to the subscapularis tendon to avoid the musculocutaneous nerve.

With the anterior portal established, we transition our arthroscope anteriorly to view the posterior pathology directly. This anterior viewing perspective is mandatory for posterior repairs, as it provides an en face view of the posterior labrum and capsule.

Tissue Preparation and Mobilization
The success of a soft-tissue repair is entirely contingent upon biology—specifically, achieving robust healing of the capsulolabral complex to the bony glenoid. We introduce an arthroscopic elevator and a motorized shaver through the posterior portal.

We meticulously elevate the torn posterior labrum and the attenuated posterior capsule off the glenoid neck. This dissection must proceed inferiorly to the 6 o'clock position to ensure adequate mobilization of the inferior glenohumeral ligament complex. Failure to adequately release the capsule inferiorly will prevent a sufficient superior shift, leading to recurrent instability. Once mobilized, we use a motorized burr to lightly decorticate the posterior glenoid neck, creating a bleeding bone bed to optimize biological healing.

Anchor Placement and Capsular Shift
Anchor placement requires extreme precision. We typically utilize an accessory posteroinferior portal (often referred to as the 7 o'clock portal) to achieve the correct trajectory. This portal is established under direct intra-articular visualization using a spinal needle. The trajectory must be low enough to address the inferior pathology but must strictly avoid plunging inferiorly into the axillary nerve.

We place our first suture anchor at the 6 o'clock or 7 o'clock position on the glenoid face, precisely at the articular margin. The drill guide must be angled slightly medially to avoid penetrating the articular cartilage, but not so medially as to risk the suprascapular nerve.

Once the anchor is seated, we utilize a specialized suture passing device (such as a curved suture lasso or a penetrator) to capture the capsulolabral tissue. The critical step here is the capsular shift. We do not merely reattach the labrum; we must address the capsular redundancy. The suture passer is driven through the capsule inferior and lateral to the anchor site. By grabbing tissue inferiorly and shifting it superiorly toward the anchor, we tension the posterior band of the IGHL and effectively reduce the capsular volume.

This "pinch-tuck" technique is repeated sequentially, moving superiorly along the posterior glenoid rim. We typically place 3 to 4 anchors, spacing them approximately 5 to 7 millimeters apart, working from inferior to superior.

Knot Tying and Final Assessment
We meticulously tie our sutures using a sliding, locking knot configuration, backed up by at least three alternating half-hitches. The knots must be positioned away from the articular surface to prevent iatrogenic chondral abrasion.

As the knots are tensioned, the surgeon should directly visualize the creation of a robust posterior capsulolabral "bumper." This bumper restores the chock-block effect and effectively tensions the posterior capsule.

After all anchors are tied, the traction is released, and the arm is taken through a gentle range of motion while visualizing the repair. The posterior joint space should appear significantly tighter, and the humeral head should remain concentrically reduced throughout internal rotation and posterior translation maneuvers.
Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique, arthroscopic posterior stabilization carries inherent risks. A thorough understanding of potential complications is vital for both preoperative patient counseling and postoperative management.
| Complication | Estimated Incidence | Etiology & Salvage Management |
|---|---|---|
| Recurrent Instability | 5% - 15% | Etiology: Unrecognized glenoid retroversion, failure to address profound capsular laxity, premature return to sport, or unrecognized concomitant anterior pathology. Management: Revision arthroscopy vs. open posterior bone block (e.g., Latarjet equivalent or distal tibial allograft) if significant bone loss is identified. |
| Postoperative Stiffness | 3% - 8% | Etiology: Overtightening of the posterior capsule, prolonged immobilization, or excessive capsulorrhaphy. Results in severe loss of internal rotation and cross-body adduction. Management: Aggressive physical therapy. If refractory beyond 6-9 months, arthroscopic posterior capsular release may be necessary. |
| Nerve Injury (Axillary/Suprascapular) | < 1% | Etiology: Errant inferior portal placement (axillary nerve) or overly medial anchor penetration (suprascapular nerve). Management: Immediate neurology consult, EMG at 3-4 weeks. Most are neuropraxias that resolve spontaneously. Structural damage requires microsurgical exploration. |
| Hardware Complications / Chondrolysis | 1% - 3% | Etiology: Prominent suture knots abrading cartilage, intra-articular anchor placement, or historical use of intra-articular pain pumps (bupivacaine toxicity). Management: Immediate arthroscopic hardware removal and chondroplasty. Severe chondrolysis may ultimately necessitate arthroplasty. |
Recurrence remains the most frustrating complication. It is imperative to re-evaluate the patient comprehensively if recurrence occurs, obtaining advanced CT imaging with 3D reconstruction to rule out osseous defects that may have been underappreciated on the initial MRI.
Phased Post-Operative Rehabilitation Protocols
The success of the surgical repair is intimately tied to the patient's strict adherence to a rigorously phased rehabilitation protocol. The posterior labrum requires time to biologically integrate into the glenoid bone bed, and premature stress will inevitably lead to structural failure.
Phase I: Maximum Protection (Weeks 0-4)
Immediately postoperatively, the patient is placed in an abduction sling or a "gunslinger" brace, maintaining the arm in neutral to 10 degrees of external rotation and 15 degrees of abduction. This position places the posterior capsulolabral repair in a completely relaxed, stress-free state. Absolute restrictions during this phase include zero internal rotation, zero cross-body adduction, and no active lifting. Therapy is limited to strictly passive forward elevation to 90 degrees and passive external rotation to 30 degrees to prevent profound adhesive capsulitis, alongside distal elbow, wrist, and hand active range of motion.
Phase II: Moderate Protection and Early Motion (Weeks 4-8)
At 4 weeks, the brace is discontinued. We transition from passive to active-assisted range of motion (AAROM), and gradually into active range of motion (AROM). Internal rotation is slowly introduced, initially restricted to the scapular plane. We begin gentle submaximal isometric strengthening of the rotator cuff and deltoid, strictly avoiding any provocative loading in the flexed and internally rotated position.
Phase III: Strengthening and Neuromuscular Control (Weeks 8-16)
Once full, symmetrical, and pain-free AROM is achieved, the focus shifts to aggressive strengthening. Isotonic strengthening of the periscapular stabilizers (rhomboids, trapezius, serratus anterior) is paramount to ensure proper scapulohumeral rhythm. Posterior rotator cuff strengthening is intensified. Closed kinetic chain exercises are introduced to enhance joint proprioception and dynamic stability.
Phase IV: Return to Sport (Months 4-6)
Return to play is highly individualized and is permitted only when the patient demonstrates full, pain-free range of motion, normal scapular kinematics, and isokinetic strength testing that is at least 90% of the contralateral, uninjured extremity. Sport-specific drills, such as throwing programs or contact-sport simulations, are gradually phased in. Linemen and weightlifters may require up to
Detailed Chapters & Topics
Dive deeper into specialized chapters regarding arthroscopic-treatment-of-posterior-shoulder-instability