Arthroscopic Posterior Shoulder Stabilization: An Intraoperative Masterclass

Key Takeaway
Welcome, fellows, to an immersive masterclass on arthroscopic posterior shoulder stabilization. We'll meticulously cover anatomy, preoperative planning, and the step-by-step intraoperative execution of this challenging procedure. Learn precise portal placement, labral repair techniques, and capsular plication for recurrent posterior instability. We'll delve into critical pearls, pitfalls, and postoperative management, ensuring comprehensive understanding for optimal patient outcomes.
Comprehensive Introduction and Patho-Epidemiology
Welcome to the operating theater. Today, we are tackling a challenging yet immensely rewarding pathology: recurrent posterior shoulder instability. This is a condition that, while historically considered less common than its anterior counterpart—accounting for approximately 5% to 12% of all shoulder instability cases—demands meticulous attention to detail, a profound understanding of posterior glenohumeral anatomy, and precise surgical execution. Our overarching goal is to restore stability, kinematics, and function for our patient while minimizing the risk of recurrence and avoiding iatrogenic stiffness.
Before we even consider making an incision, we must have a crystal-clear understanding of the pathology we are addressing. It is crucial to differentiate between two distinct clinical entities, as their management algorithms diverge significantly. The first is the true posterior dislocation. This is often acute, traumatic, and typically managed with closed reduction in the emergency setting. If not associated with a large engaging humeral head defect (a reverse Hill-Sachs lesion) or an uncontrolled seizure disorder, an isolated acute event generally carries a low recurrence rate. However, if missed during the initial presentation, it can progress to a chronic locked posterior dislocation, presenting with a pathognomonic internally rotated resting position and a profound loss of active and passive external rotation.
The second entity, recurrent unidirectional posterior subluxation, is the more challenging diagnostic and therapeutic dilemma and serves as our primary focus today. This condition can be traumatic, often seen in high-demand athletes aged 18 to 30 involved in contact sports. The mechanism typically involves an axial load applied to the arm in a straight and locked position—such as a weightlifter performing a bench press or an offensive lineman run-blocking—or a fall onto an outstretched hand with the shoulder in forward elevation, adduction, and internal rotation.
More frequently, however, we encounter cases with a poorly defined, insidious, atraumatic onset, predominantly in overhead athletes such as swimmers, gymnasts, baseball pitchers, and volleyball players. These cases involve repetitive microtrauma leading to progressive plastic deformation and stretching of the posterior capsular restraints. Patients typically complain of deep posterior pain and weakness, with frank subluxation episodes occurring later in the disease process. They may even learn to voluntarily demonstrate their instability with specific muscular contractions and arm positions, typically forward elevation, adduction, and internal rotation.
Detailed Surgical Anatomy and Biomechanics
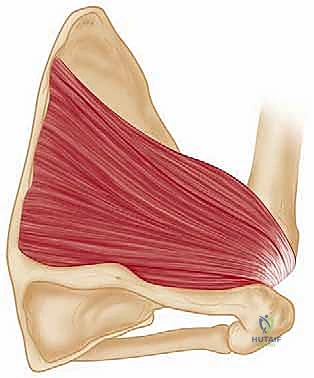
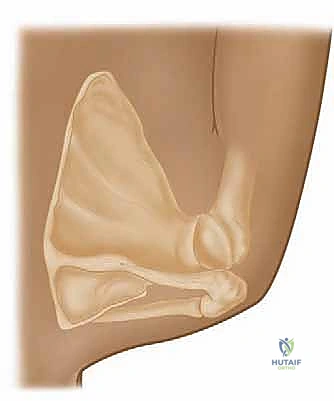
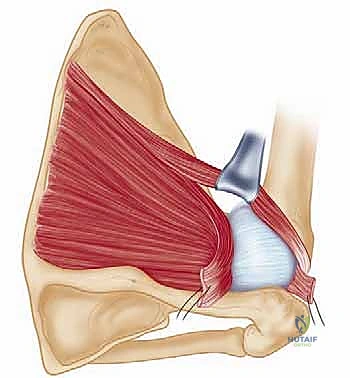
A profound mastery of the posterior glenohumeral capsulolabral complex is non-negotiable for the arthroscopic shoulder surgeon. The posterior stability of the shoulder relies on a delicate interplay between static and dynamic restraints. The primary static restraints include the bony architecture of the glenoid and humeral head, the posterior labrum, and the posterior capsule, specifically the posterior band of the inferior glenohumeral ligament (PB-IGHL).
The glenoid is typically retroverted between 0 and 7 degrees. Excessive retroversion (dysplasia) significantly diminishes the bony restraint to posterior translation and is a critical factor to identify preoperatively. The posterior labrum serves to deepen the glenoid concavity, increasing the surface area for articulation and providing a robust anchor point for the capsular ligaments. The PB-IGHL, originating from the posterior labrum and inserting onto the anatomical neck of the humerus, is the primary static restraint to posterior translation when the arm is flexed, adducted, and internally rotated—the classic "at-risk" position.
Dynamic stability is primarily provided by the rotator cuff musculature. The subscapularis anteriorly and the infraspinatus and teres minor posteriorly act as a force couple, compressing the humeral head into the glenoid concavity throughout the arc of motion. The long head of the biceps and the periscapular musculature also play vital supporting roles in maintaining normal glenohumeral kinematics. Scapular dyskinesia, often seen in these patients, can exacerbate posterior instability by functionally increasing glenoid retroversion during arm elevation.

Pathologically, we must recognize several distinct lesions. The Posterior Labrocapsular Periosteal Sleeve Avulsion (POLPSA) involves a detachment of the labrum and intact capsule from the posterior glenoid, stripping the periosteum medially. The Kim Lesion, described by Dr. Seung-Ho Kim, is a concealed, incomplete avulsion of the posteroinferior labrum, often presenting as a marginal crack or loss of normal labral contour without frank detachment. We must also be vigilant for the Posterior Humeral Avulsion of the Glenohumeral Ligament (Posterior HAGL lesion) and generalized patulous posterior capsular redundancy, which is common in atraumatic overhead athletes.
Exhaustive Indications and Contraindications
The decision to proceed with operative intervention must be carefully weighed against the patient's functional demands, pathoanatomy, and response to conservative measures. It is a well-established tenet that nonoperative treatment for posterior unidirectional instability is successful in up to 80% of patients, particularly those with atraumatic etiologies. Our surgical candidates are those who have failed an exhaustive, well-supervised trial of physical therapy and remain significantly symptomatic, unable to return to their desired level of sport or occupation.
The ideal surgical candidates are those with recurrent posterior unidirectional subluxation secondary to a discrete traumatic episode, presenting with an associated traumatic posterior labral tear (e.g., a reverse Bankart or Kim lesion). These structural lesions are highly amenable to arthroscopic repair. Patients with atraumatic subluxation due to isolated capsular redundancy can also be managed arthroscopically with a capsular shift or plication, provided they do not have underlying connective tissue disorders.
| Category | Indications for Arthroscopic Posterior Stabilization | Contraindications for Arthroscopic Stabilization |
|---|---|---|
| Clinical | Failure of 3-6 months of targeted physical therapy | Voluntary instability with underlying psychiatric overlay |
| Pathoanatomic | Traumatic posterior labral tear (Reverse Bankart, POLPSA) | Uncontrolled seizure disorders |
| Pathoanatomic | Symptomatic Kim Lesion | Massive posterior glenoid bone loss (>20%) requiring bone block |
| Pathoanatomic | Patulous posterior capsule with recurrent subluxation | Large, engaging reverse Hill-Sachs lesion requiring McLaughlin procedure |
| Patient Factors | High-demand athlete unable to return to play | Non-compliant patient unable to adhere to postoperative restrictions |
Pre-Operative Planning, Templating, and Patient Positioning
Our preparation begins long before the patient enters the OR. An exhaustive history and physical examination are paramount. Instability episodes typically occur in the "at-risk" position (forward elevation, adduction, internal rotation). Overhead athletes may report a loss of velocity, early fatigue, or a deep posterior shoulder ache rather than frank instability.
Diagnostic maneuvers are critical. The Load Shift Test documents the direction and degree of instability. The Jerk Test, performed by abducting the arm to 90 degrees, internally rotating, and axially loading the humerus while horizontally adducting, is highly sensitive. A sudden "jerk" or clunk as the humeral head subluxes posteriorly over the glenoid rim indicates instability. A painful jerk test is highly suggestive of a posteroinferior labral lesion. The Kim Test further isolates the posteroinferior labrum.
Imaging is the cornerstone of our preoperative templating. Plain radiographs must include a true AP, scapular lateral, and axillary views. For patients with voluntary instability, we can take axillary radiographs while they reproduce and maintain the subluxation to clearly document the direction and severity.
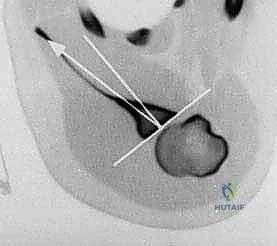
Magnetic Resonance Imaging (MRI), preferably an MRI Arthrogram, is the imaging modality of choice. It is essential for evaluating the posterior capsule, labrum, and associated pathology. We look for the absence of the normal posterior labral triangle, paralabral cysts, or contrast extravasation indicative of a capsulolabral disruption.

Computed Tomography (CT) is invaluable for assessing bony pathology. We must quantify posterior glenoid retroversion and evaluate for posterior glenoid rim fractures or erosions. A 3D CT reconstruction provides a topographic map of the glenoid bone stock, which dictates whether a soft tissue repair will suffice or if a posterior bone block augmentation is required.

Patient Setup and Examination Under Anesthesia
On the day of surgery, before positioning, we perform a crucial examination under anesthesia (EUA). This confirms the direction and degree of instability without muscular guarding, providing the most accurate assessment of capsular laxity and labral integrity.
The patient is then carefully positioned in the lateral decubitus position on the operating table using a beanbag positioner. The operative arm is placed in approximately 40 degrees of abduction and subjected to no more than 10 to 15 pounds of longitudinal traction using a specialized arm holder.


We strictly avoid double traction setups, which are common in anterior instability. Increased adduction tends to close down visualization of the posteroinferior joint line. We have found that 40 degrees of abduction provides optimal visualization when viewing from the anterior portal. The patient's body is placed close to the operating surgeon and tipped posteriorly 15 to 20 degrees. This posterior tilt helps open up the posterior aspect of the glenohumeral joint, improving our angle of attack for posterior portal placement.

Step-by-Step Surgical Approach and Fixation Technique
Portal Placement and Diagnostic Arthroscopy
Precision in portal placement is the foundation of a successful arthroscopic posterior stabilization. We typically perform most posterior reconstructions using two primary portals and occasionally a third accessory portal for optimal triangulation.
The Posterior Portal (Working Portal) is established just lateral to the posterolateral corner of the acromion. This differs from the traditional posterior viewing portal, which is typically 1 cm medial and 2 cm inferior. This lateralized and slightly superior placement provides an optimal angle of attack to the posterior and inferior portion of the glenoid, allowing us to instrument the entire posteroinferior labral complex parallel to the joint surface.

An Anterior Superior Portal is established within the rotator interval to serve as our primary viewing portal. Once the arthroscope is introduced anteriorly, we perform a comprehensive diagnostic sweep. We evaluate the anterior labrum, the superior labrum (SLAP lesions), the rotator cuff, and the articular surfaces. We then turn our attention posteriorly, probing the posterior labrum to identify Kim lesions, frank detachments, and the degree of capsular redundancy.


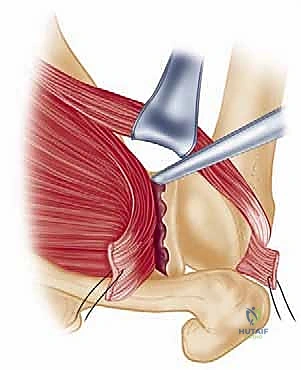
Tissue Preparation and Mobilization
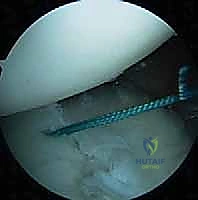
The success of the repair hinges on adequate tissue mobilization and biologic preparation of the healing bed. Using an arthroscopic elevator or a rasp introduced through the posterior portal, we meticulously elevate the posterior labrum and capsule away from the glenoid neck. It is imperative to release any adhesions down to the 6 o'clock position to allow for a superior and medial shift of the capsulolabral complex.

Once the tissue is freely mobile, we use a motorized burr or a rasp to decorticate the posterior glenoid neck. We aim to create a bleeding cancellous bone bed to optimize biologic healing of the shifted capsule and labrum. Care must be taken not to alter the native glenoid version by over-resecting the posterior rim.


Anchor Insertion and Capsulolabral Plication
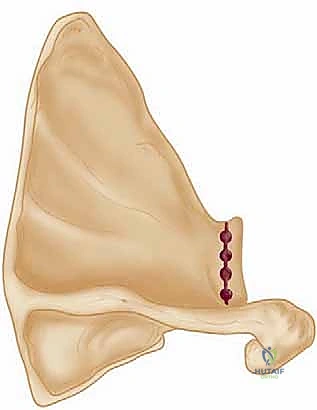
With the bed prepared, we proceed with anchor placement. We utilize modern biocomposite or all-suture anchors, typically 2.4mm to 3.0mm in diameter, double-loaded with high-strength non-absorbable suture. The first anchor is placed at the most inferior aspect of the lesion, usually at the 6:30 or 7 o'clock position (for a right shoulder). The drill guide is introduced through the posterior portal, and the anchor is inserted at a 45-degree angle to the articular surface to ensure adequate bone purchase and avoid articular cartilage penetration.
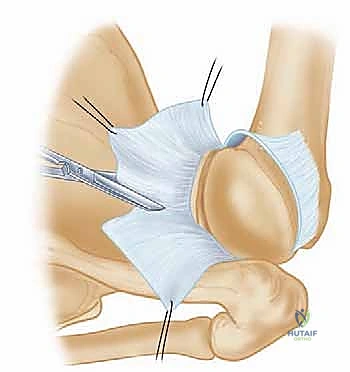
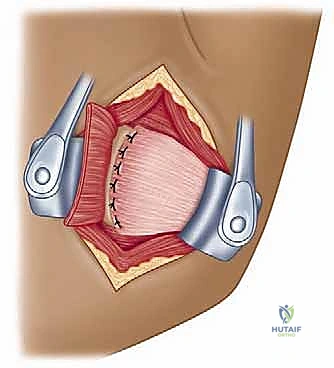
Suture passing is the most critical step for achieving the desired capsular shift. We utilize a curved suture passing device (e.g., a spectrum or a crescent hook) introduced through the posterior portal. We pierce the capsule inferior and lateral to the anchor site, typically taking a 1 cm bite of capsule, and then pass the instrument through the labrum. This "south-to-north" and "lateral-to-medial" bite ensures that when the knot is tied, the redundant inferior capsule is shifted superiorly and medially, recreating the posterior bumper.
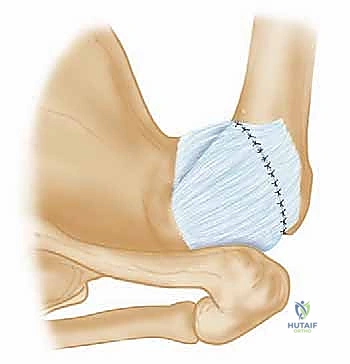
We retrieve the sutures and tie them using a sliding, locking knot followed by alternating half-hitches. The knot should be positioned away from the articular surface to prevent iatrogenic chondral injury. As the knot is tensioned, the surgeon visually confirms the obliteration of the posterior capsular recess and the restoration of a robust labral bumper.

This process is repeated sequentially, moving superiorly along the posterior glenoid rim. Typically, 2 to 4 anchors are required depending on the extent of the lesion and the degree of capsular laxity. Each subsequent anchor is placed approximately 1 cm superior to the previous one, working towards the 9 o'clock or 10 o'clock position.
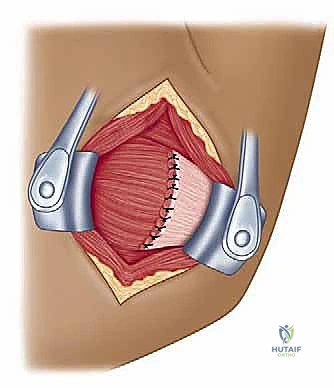
In cases of profound capsular redundancy without a discrete labral tear, we perform a capsular plication. This involves passing sutures through the capsule and the intact labrum to "reef" the tissue, effectively shortening the posterior capsular restraints.
Upon completion of the repair, a final diagnostic sweep is performed from both the anterior and posterior portals. We confirm that the humeral head is centralized, the posterior capsular drive-through sign is eliminated, and a substantial, tensioned posterior labral bumper has been reconstructed.
Complications, Incidence Rates, and Salvage Management
While arthroscopic posterior stabilization is highly effective, it is not without risks. A thorough understanding of potential complications is mandatory for appropriate patient counseling and intraoperative vigilance. Historically, open posterior stabilization was fraught with high recurrence rates and stiffness. Modern arthroscopic techniques have significantly improved outcomes, yet challenges remain.
Recurrent instability is the most common complication, with modern literature citing recurrence rates between 5% and 10%. Recurrence is strongly correlated with unrecognized bony deficiency (glenoid retroversion or reverse Hill-Sachs lesions), inadequate capsular plication, or premature return to heavy contact sports.
Postoperative stiffness, particularly a loss of internal rotation, can occur if the posterior capsule is over-tensioned during plication. While some loss of internal rotation is expected and necessary for stability, severe restriction can impair function, particularly in overhead athletes.
| Complication | Estimated Incidence | Prevention and Salvage Management |
|---|---|---|
| Recurrent Instability | 5% - 10% | Prevention: Accurately assess bone loss pre-op; perform adequate capsular shift. Salvage: Revision arthroscopy, open capsular shift, or posterior bone block (iliac crest/distal tibia). |
| Postoperative Stiffness | 3% - 5% | Prevention: Avoid over-plication; implement structured, phased rehabilitation. Salvage: Aggressive physical therapy; rarely requires arthroscopic capsular release. |
| Hardware Failure / Migration | < 1% | Prevention: Use modern all-suture or biocomposite anchors; ensure proper insertion angle. Salvage: Arthroscopic hardware removal and revision stabilization. |
| Nerve Injury (Axillary/Suprascapular) | < 1% |
