Arthroscopic Reduction and Fixation of Distal Radius and Ulnar Styloid Fractures

Comprehensive Introduction and Patho-Epidemiology
Fractures of the distal radius represent one of the most ubiquitous and clinically significant skeletal injuries managed by orthopaedic surgeons globally. Epidemiological data underscore the sheer volume of these injuries, revealing that they account for approximately one-sixth of all fracture evaluations within the acute Emergency Department setting. The demographic distribution of distal radius fractures follows a classic bimodal curve, reflecting two distinct patient populations with divergent mechanisms of injury. In young, active adults, these fractures are predominantly the result of high-energy trauma, such as motor vehicle collisions or falls from significant heights, which impart massive axial and shearing forces across the radiocarpal joint. Conversely, in the elderly population, these injuries are typically low-energy fragility fractures resulting from falls from a standing height, exacerbated by underlying osteopenia or frank osteoporosis.

The incidence of distal radius fractures in the geriatric population is staggering. Patients 65 years of age or older demonstrate an annual incidence of 8 to 10 fractures per 1,000 person-years. The gender disparity is particularly pronounced in this demographic, with the incidence being seven times higher in women than in men. Current projections indicate that 16% of white women and 23% of white men will sustain a fracture of the distal radius after the age of 50 years. This demographic reality necessitates a nuanced approach to treatment, as the fragile soft tissue envelope and compromised bone mineral density in elderly patients present unique challenges to both closed reduction and surgical osteosynthesis.

To systematically approach these injuries, Fernandez and Geissler developed a comprehensive classification system predicated on the mechanism of injury, which directly correlates the degree of energy absorbed by the distal radius with associated ligamentous lesions, carpal subluxations, and concomitant carpal fractures. Type I fractures are extra-articular bending fractures of the metaphysis (e.g., classic Colles’ or Smith’s fractures) where one cortex fails under tensile stress while the opposite undergoes comminution. Type II fractures are shearing injuries of the joint surface, classically represented by radial styloid (Chauffeur's) or Barton’s fractures. Type III injuries are intra-articular compression fractures characterized by the impaction of subchondral and metaphyseal cancellous bone, often resulting in complex die-punch fragments. Type IV fractures involve avulsion of ligamentous attachments, including radial and ulnar styloid fractures, frequently associated with devastating radiocarpal fracture-dislocations. Finally, Type V fractures are high-energy injuries encompassing a catastrophic combination of bending, compression, shearing, and avulsion mechanisms, often with significant bone loss.
Displaced intra-articular fractures of the distal radius (Types III, IV, and V) constitute a uniquely challenging subset of injuries. These high-energy fracture patterns are inherently less amenable to traditional closed manipulation and cast immobilization due to severe comminution and inherent instability. Furthermore, intra-articular fractures of the distal radius possess two distinct but equally critical pathologies: the complex injury to the osseous architecture and the global, often occult, injury to the surrounding soft tissues. Arthroscopic studies have definitively demonstrated a remarkably high incidence of associated soft tissue injuries in displaced intra-articular distal radius fractures. The triangular fibrocartilage complex (TFCC) is the most frequently injured structure, followed closely by the scapholunate (SL) interosseous ligament, and less commonly, the lunotriquetral (LT) interosseous ligament. The ultimate prognosis for these fractures is inextricably linked not only to the restoration of radiocarpal and radioulnar articular congruity and the correction of residual radial shortening but also to the meticulous identification and management of these critical soft tissue stabilizers.
Detailed Surgical Anatomy and Biomechanics
The distal radius serves as the foundational osseous plateau that supports the entire carpus, facilitating the complex, multi-planar kinematics of the human wrist. The distal articular surface is anatomically sophisticated, comprising three distinct concave articular surfaces: the scaphoid fossa, the lunate fossa, and the sigmoid notch. The scaphoid and lunate fossae are separated by a subtle anteroposterior ridge of articular cartilage, which corresponds to the scapholunate interval. The volar rim of the lunate facet, radiographically represented as the anterior teardrop, is a critical osseous buttress; failure to restore and stabilize this fragment can lead to catastrophic volar carpal subluxation.

Standard radiographic parameters of the native distal radius are essential benchmarks for anatomic restoration. The distal articular surface exhibits a radial inclination averaging 22 to 23 degrees (range 13–30 degrees) in the coronal plane. In the sagittal plane, the articular surface possesses a palmar (volar) tilt averaging 11 to 12 degrees (range 1–21 degrees). Normal radial length, or height, averages 12 mm (range 8–18 mm) when measured from the tip of the radial styloid to the level of the ulnar head articular surface. Ulnar variance, the relative length of the distal ulna compared to the distal radius, must be meticulously evaluated, ideally with the patient's shoulder in 90 degrees of abduction, the elbow at 90 degrees of flexion, and the wrist in neutral pronation-supination to account for dynamic variance changes.
The biomechanical implications of failing to restore these anatomic parameters are profound. The distal radius normally transmits approximately 80% of the axial load across the wrist, with the distal ulna bearing the remaining 20%. A loss in radial length of merely 2.5 mm will drastically alter this kinematic relationship, shifting the load transmitted across the ulna from 20% to 42%. This abnormal load distribution invariably leads to varying stages of ulnar impaction syndrome, characterized by accelerated degenerative changes at the ulnocarpal articulation, TFCC attrition, and chronic, debilitating ulnar-sided wrist pain. Furthermore, residual dorsal tilt alters the contact mechanics of the radiocarpal joint, concentrating forces dorsally and predisposing the patient to midcarpal instability and early radiocarpal arthrosis.
Ligamentous support of the distal radius and carpus is highly complex. Radial-based volar and dorsal extrinsic ligaments arise from the metaphyseal and epiphyseal regions of the distal radius to suspend and support the carpal rows. The distal radioulnar joint (DRUJ) is primarily stabilized by the TFCC, which originates from the ulnar margin of the lunate fossa and inserts onto the base of the ulnar styloid. The sigmoid notch of the distal radius, which angles distally and medially at an average of 22 degrees, articulates with the ulnar head. During forearm pronation and supination, the radius rotates around the fixed ulnar head, guided by the articular contour of the sigmoid notch and constrained by the volar and dorsal radioulnar ligaments of the TFCC. Any incongruity of the sigmoid notch or disruption of the TFCC can lead to profound DRUJ instability and restricted forearm rotation.
Exhaustive Indications and Contraindications
The evolution of distal radius fracture management has increasingly favored operative intervention, particularly for intra-articular and unstable fracture patterns. Arthroscopic-assisted reduction and internal fixation (ORIF) represents the pinnacle of this evolution, allowing for direct visualization of the articular surface and concomitant assessment of intrinsic ligamentous integrity without the morbidity of extensive arthrotomies. The primary indication for surgical intervention is a fracture pattern that is inherently unstable and for which closed reduction is either impossible to achieve or impossible to maintain.

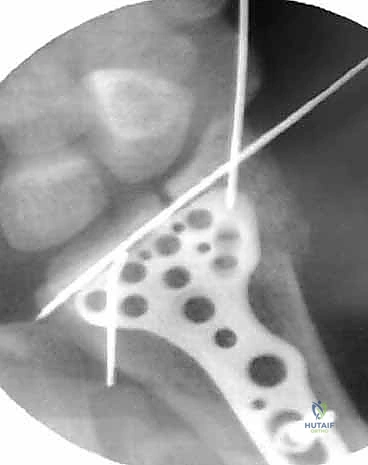
Radiographic signs that definitively indicate instability and necessitate surgical stabilization include: initial fragment displacement greater than 1 cm, volar translation greater than 2 mm, initial radial shortening exceeding 5 mm, lateral/dorsal tilt greater than 20 degrees, and dorsal comminution encompassing more than 50% of the metaphyseal width. Furthermore, specific fracture morphologies such as radial styloid fractures, impacted die-punch fractures, three-part T-type fractures, and four-part fractures with extensive metaphyseal comminution are prime candidates for operative fixation, typically utilizing a combination of volar locking plates and arthroscopic adjuncts. The presence of an associated ulnar fracture, severe osteoporosis, or patient age greater than 60 years further tips the scales toward surgical stabilization to permit early mobilization.

Arthroscopic assistance is specifically indicated to achieve anatomic articular restoration. Knirk and Jupiter documented the paramount importance of articular restoration over extra-articular orientation in predicting long-term outcomes, demonstrating solid evidence that the absolute maximum tolerable articular step-off is 2 mm. However, modern arthroscopic techniques aim for near-zero step-off, as even 1 mm of incongruity can alter contact stresses by up to 40%. Additionally, fractures with strongly suspected associated soft tissue injuries—such as TFCC tears, complete scapholunate ligament ruptures, or DRUJ disruptions—are absolute indications for arthroscopy. Wrist arthroscopy provides the definitive rationale for when and how to stabilize an associated ulnar styloid fragment by allowing direct dynamic assessment of DRUJ stability from within the radiocarpal and radioulnar spaces.

Contraindications to arthroscopic-assisted fixation must be carefully respected to avoid catastrophic complications. Active local or systemic infection is an absolute contraindication to any internal fixation or arthroscopic procedure. Massive soft tissue compromise, severe degloving injuries, or impending compartment syndrome may preclude the safe establishment of arthroscopic portals due to the risk of fluid extravasation exacerbating tissue tension. Furthermore, patients with severe medical comorbidities, including unstable cardiac or neurologic conditions, may not be candidates for the required anesthesia.
| Indication Category | Specific Clinical/Radiographic Criteria |
|---|---|
| Absolute Radiographic Instability | Dorsal tilt >20°, Shortening >5mm, Volar translation >2mm, Initial displacement >1cm, Dorsal comminution >50%. |
| Articular Incongruity | Intra-articular step-off or gap >2mm (aiming for absolute anatomic reduction via arthroscopy). |
| Specific Fracture Patterns | Radial styloid shear (Chauffeur's), Impacted die-punch, 3-part T-type, 4-part highly comminuted. |
| Soft Tissue Suspicion | Suspected TFCC avulsion, DRUJ instability, Scapholunate/Lunotriquetral interosseous ligament tears. |
| Absolute Contraindications | Active local infection, massive soft tissue compromise/degloving, uncorrected coagulopathy. |
| Relative Contraindications | Severe impending compartment syndrome (risk of fluid extravasation), medically unstable patient. |


Pre-Operative Planning, Templating, and Patient Positioning
Thorough preoperative planning begins with an exhaustive patient history and meticulous physical examination. The surgeon must ascertain the exact circumstances surrounding the injury, the mechanism of trauma, and the presence of any additional polytraumatic injuries. It is critical to determine the patient’s level of independence, dominant hand, occupational demands, baseline activity level, and available psychosocial support structure, as these factors heavily influence the choice of implants and the aggressiveness of the postoperative rehabilitation protocol.

The physical examination must extend beyond the wrist to include the entire hand, elbow, and shoulder to rule out concomitant injuries such as an Essex-Lopresti lesion or ipsilateral upper extremity fractures. The soft tissue envelope must be carefully inspected for open wounds, abrasions, or severe contusions; any open injury necessitates immediate tetanus prophylaxis, intravenous antibiotics, and urgent surgical debridement. A thorough and organized distal sensory and motor function examination is mandatory. Vascular assessment must include palpation of both radial and ulnar pulses and determination of capillary refill time. Crucially, the surgeon must maintain a high index of suspicion for compartment syndrome; clinical signs such as diminished sensibility, pallor, altered capillary refill, increased tenseness of the forearm compartments, and, most importantly, pain out of proportion to the injury or pain with passive digital extension require immediate intervention.

Imaging is the cornerstone of preoperative templating. The primary radiographic workup consists of high-quality posteroanterior (PA), oblique, and true lateral radiographs. PA projections evaluate radial inclination, radial height, ulnar variance, widening of the DRUJ, intracarpal spacing, and gross intra-articular involvement. The lateral projection is indispensable for assessing volar or dorsal tilt of the distal fragment, subluxation of the carpus, lunate angulation (DISI or VISI deformity), and the extent of dorsal comminution. Oblique radiographs are highly valuable as major fracture fragments, particularly radial styloid or dorsal ulnar corner fragments, may be rotated out of standard anatomic planes.

Advanced imaging techniques are frequently employed for complex intra-articular patterns. A modified lateral radiograph with the beam angulating 10 to 30 degrees proximally improves visualization of the articular surface and the critical volar rim of the lunate facet. An additional 30-degree anteroposterior (AP) cephalic projection is useful to evaluate the dorsal ulnar margin. Computed Tomography (CT), particularly three-dimensional (3D) CT reconstruction, is the gold standard for delineating exact fragment location, the degree of joint compression (die-punch depth), and fragment rotation. Magnetic Resonance Imaging (MRI) is highly sensitive for assessing associated soft tissue injuries, including TFCC tears, SL/LT interosseous ligament injuries, and occult carpal bone fractures, though it is less commonly utilized in the acute trauma setting compared to CT and direct arthroscopic evaluation. Contralateral radiographs of the uninvolved extremity provide an invaluable patient-specific template for restoring native radial inclination, ulnar variance, and sigmoid notch anatomy.


For the surgical setup, the patient is typically positioned supine on the operating table with the affected arm extended on a radiolucent hand table. Regional anesthesia (supraclavicular or axillary block) combined with intravenous sedation is preferred, though general anesthesia may be utilized based on patient factors or anticipated surgical duration. A well-padded pneumatic tourniquet is applied to the proximal arm. For the arthroscopic portion, the arm is placed in specialized finger traps utilizing the index and long fingers, and 10 to 15 pounds of longitudinal traction is applied via a traction tower or counterweight system. This traction is essential to disimpact the fracture fragments and open the radiocarpal and midcarpal joint spaces for instrument insertion. Equipment preparation must include small joint instrumentation; a 2.7 mm arthroscope (or smaller, such as 1.9 mm) is essential, alongside a small joint shaver (3.5 mm or less) to aggressively clear fracture debris, organized hematoma, and fibrinous exudate that rapidly obscures the visual field.
Step-by-Step Surgical Approach and Fixation Technique
The surgical procedure commences with an initial closed reduction maneuver to restore gross anatomic alignment and relieve tension on the neurovascular structures. Knowledge of the specific mechanism of injury dictates the reduction technique; force is applied in the vector opposite to that which caused the fracture. Gentle, sustained longitudinal traction is necessary to disimpact the metaphyseal fracture fragments. This is followed by palmar translation of the hand and carpus relative to the radius. The radial articular surface will rotate around the intact volar cortical lip to restore volar inclination. Extreme care must be taken to avoid secondary trauma to the skin during these maneuvers, particularly in elderly patients with fragile, parchment-like integument.

Once gross alignment is achieved and the arm is
Clinical & Radiographic Imaging Archive