Arthroscopic Capsular Release for Shoulder Stiffness: An Intraoperative Masterclass

Key Takeaway
This masterclass details arthroscopic capsular release for shoulder stiffness, guiding fellows through comprehensive surgical anatomy, meticulous preoperative planning, and precise intraoperative execution. We cover essential techniques for releasing contracted capsular structures, emphasizing neurovascular protection and optimal patient outcomes. Learn pearls, pitfalls, and postoperative management strategies to restore motion effectively.
Comprehensive Introduction and Patho-Epidemiology
Welcome to the operating theater and to this definitive masterclass on the surgical management of the stiff shoulder. Today, we are tackling a condition that is as challenging to treat as it is debilitating for the patient: recalcitrant shoulder stiffness. Specifically, we will focus on the nuanced, highly technical execution of the arthroscopic capsular release. This procedure is far more sophisticated than simply incising contracted tissue; it requires a profound, three-dimensional understanding of glenohumeral anatomy, a meticulous surgical strategy to restore physiologic kinematics, and an unwavering respect for the adjacent neurovascular structures. Our ultimate objective is the complete restoration of function and the alleviation of chronic pain, returning patients to their pre-morbid quality of life.
The pathophysiology of shoulder stiffness, historically grouped under the umbrella term "adhesive capsulitis" or "frozen shoulder," is fundamentally a process of intense fibroblastic proliferation and subsequent capsular contracture. At the cellular level, the condition is characterized by a dense matrix of type I and type III collagen, heavily populated by myofibroblasts, which actively contract the capsuloligamentous tissue. This fibroplasia is driven by a complex cytokine cascade, notably involving transforming growth factor-beta (TGF-β) and platelet-derived growth factor (PDGF), which orchestrate the relentless inflammatory and fibrotic response. Unlike simple scar tissue, the capsule in a frozen shoulder undergoes active, dynamic contraction, fundamentally altering the joint's volume and biomechanics.
Clinically, we categorize adhesive capsulitis into primary and secondary forms, a distinction that critically informs our surgical expectations and prognostic discussions. Primary adhesive capsulitis is idiopathic, presenting as an insidious onset of severe pain followed by a progressive, global loss of both active and passive range of motion. Secondary adhesive capsulitis, conversely, possesses an identifiable etiology. This includes metabolic triggers—most notably diabetes mellitus and thyroid dysfunction, which often yield a more protracted, severe, and bilateral disease course. Furthermore, secondary stiffness frequently arises post-traumatically or post-operatively. Post-operative stiffness is a particularly common and frustrating sequela, often resulting from an exaggerated inflammatory response, prolonged immobilization, or technical errors such as over-tensioning during a concomitant stabilization or rotator cuff repair procedure.
The natural history of idiopathic adhesive capsulitis is classically described in three overlapping stages: the "Freezing" stage (characterized by intense, rest-disrupting pain and progressive motion loss over 6 to 9 months), the "Frozen" stage (where pain begins to subside but profound stiffness persists for 4 to 12 months), and the "Thawing" stage (a gradual, albeit often incomplete, return of motion over 5 to 26 months). However, contemporary longitudinal studies have debunked the myth that this condition is universally self-limiting. Up to 40% of patients will experience persistent, clinically significant range-of-motion deficits if left entirely to natural history. Therefore, when aggressive, structured non-operative management fails, arthroscopic capsular release becomes the gold standard for restoring glenohumeral kinematics.
Detailed Surgical Anatomy and Biomechanics
The Capsuloligamentous Framework
To perform a safe and effective arthroscopic capsular release, the surgeon must possess an encyclopedic knowledge of the shoulder's capsuloligamentous structures. In their native, un-diseased state, these ligaments function as dynamic, physiological check-reins, preventing excessive translation of the humeral head at the extremes of motion. However, in the setting of adhesive capsulitis, these structures undergo profound hypertrophy and contracture, transforming from stabilizers into formidable barriers to movement. The capsule is not a uniform, homogenous sheet; rather, it is punctuated by distinct, thickened bands known as the glenohumeral ligaments, which dictate the specific directional loss of motion observed clinically.
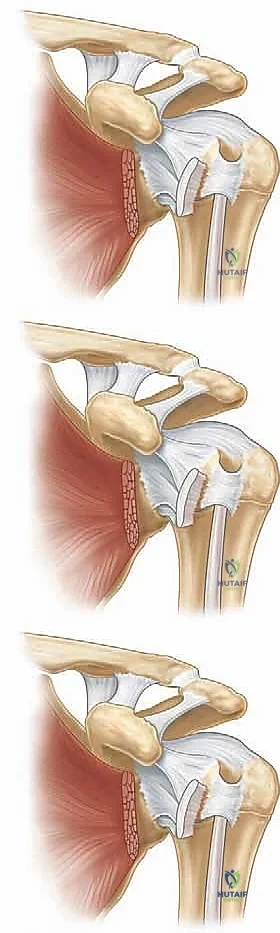
The primary structures of interest include the Superior Glenohumeral Ligament (SGHL), the Middle Glenohumeral Ligament (MGHL), and the Inferior Glenohumeral Ligament (IGHL) complex. The SGHL and the Coracohumeral Ligament (CHL) form the structural foundation of the rotator interval, a triangular space bordered by the supraspinatus superiorly, the subscapularis inferiorly, and the coracoid process medially. The MGHL courses obliquely across the deep surface of the subscapularis tendon, acting as a primary restraint to anterior translation in mid-ranges of abduction. The IGHL complex is the most robust capsular structure, consisting of an anterior band, a redundant axillary pouch, and a posterior band. This complex acts as a hammock, supporting the humeral head and serving as the primary restraint to inferior and anterior translation at 90 degrees of abduction.

Adhesive Planes and Extra-Articular Contractures
Stiffness is rarely confined solely to the intra-articular glenohumeral capsule. Profound motion loss frequently involves extra-articular adhesive planes that must be systematically addressed during surgery. The subdeltoid space, located between the deltoid muscle and the proximal humerus, is highly susceptible to scarring, particularly following trauma or open surgical approaches (such as proximal humerus fracture fixation). Obliteration of this gliding plane severely restricts both abduction and forward elevation. Similarly, the subacromial space, normally occupied by the pliant subacromial bursa, can become densely fibrotic. Scar tissue in this region binds the superior surface of the rotator cuff to the undersurface of the acromion, eliminating the necessary excursion of the cuff tendons during arm elevation.

During normal shoulder kinematics, the glenohumeral capsule and its ligaments must smoothly tighten and fold in concert with the contraction and lengthening of the rotator cuff and periscapular musculature. When adhesions tether these layers together, the harmonious interplay is destroyed. For instance, contracture of the rotator interval (specifically the CHL) acts as a dense tether against the base of the coracoid, obliterating external rotation, particularly when the arm is adducted at the side. Understanding these specific anatomical correlations allows the surgeon to perform a targeted, bespoke release rather than a blind, circumferential capsulotomy.

Neurovascular Relations: The Axillary Nerve
The most critical anatomical relationship to master during an arthroscopic capsular release is the course of the axillary nerve. Iatrogenic injury to this nerve is the most devastating complication of this procedure, leading to deltoid paralysis and profound functional loss. The axillary nerve originates from the posterior cord of the brachial plexus, courses anterior to the subscapularis muscle belly, and dives posteriorly through the quadrangular space. As it exits the quadrangular space, it lies in terrifyingly close proximity to the inferior capsule—often within 2 to 3 millimeters of the capsular reflection at the 6 o'clock position.

To navigate this danger zone safely, the surgeon must rely on consistent intraoperative landmarks. The most reliable safety margin during the anterior and anteroinferior release is the muscular belly of the subscapularis. The axillary nerve consistently runs inferior to the muscular portion of the subscapularis. Therefore, as long as the surgeon can visualize the red muscle fibers of the subscapularis during the anterior release, they are operating superior to the nerve. However, as the release progresses inferiorly past the 5 o'clock position (in a right shoulder), the muscle belly tapers, and the capsule becomes intimately juxtaposed with the nerve. Here, the release must be performed with meticulous care, utilizing blunt dissection or radiofrequency ablation strictly on the glenoid side of the capsule to avoid thermal or mechanical injury to the nerve.

Exhaustive Indications and Contraindications
The decision to proceed with an arthroscopic capsular release must be made judiciously, balancing the severity of the patient's functional deficit against the inherent risks of surgical intervention. The primary indication is a confirmed diagnosis of adhesive capsulitis (primary or secondary) that has proven entirely refractory to a comprehensive, structured non-operative regimen. This conservative phase must be exhaustive, typically lasting a minimum of 3 to 6 months, and should include aggressive physical therapy focused on stretching, NSAIDs, and intra-articular corticosteroid injections (often performed under fluoroscopic or ultrasound guidance to ensure capsular distension).

Surgical intervention is particularly indicated when the patient's quality of life is severely compromised, their ability to perform activities of daily living (ADLs) is curtailed, or their occupational demands cannot be met due to the motion deficit. In cases of post-operative stiffness—such as following a rotator cuff repair or labral stabilization—the timeline for intervention may be accelerated. If a patient fails to progress or regresses in their range of motion despite compliance with rehabilitation at the 3-to-4-month post-operative mark, early arthroscopic lysis of adhesions and capsular release can prevent permanent joint contracture and salvage the outcome of the index procedure.

Conversely, absolute contraindications include active articular or periarticular infection, which necessitates thorough debridement and targeted antimicrobial therapy rather than a primary motion-restoring procedure. Severe, end-stage glenohumeral osteoarthritis is also a contraindication for isolated capsular release, as the stiffness is primarily osseous and mechanical rather than soft-tissue in origin; these patients are better served by shoulder arthroplasty. Relative contraindications include Complex Regional Pain Syndrome (CRPS), where surgical trauma can exacerbate the dysautonomic pain cycle, and patients with profound psychiatric comorbidities or a demonstrated inability to comply with the rigorous, painful post-operative rehabilitation protocol required to maintain the surgically achieved motion.
| Category | Specific Conditions | Clinical Rationale |
|---|---|---|
| Primary Indications | Refractory Idiopathic Adhesive Capsulitis | Failure of 3-6 months of conservative management (PT, intra-articular steroids); severe ADL limitation. |
| Secondary Indications | Post-Traumatic / Post-Operative Stiffness | Arrested rehabilitation progress at 3-4 months post-op; dense subacromial or subdeltoid scarring limiting kinematics. |
| Secondary Indications | Diabetic Adhesive Capsulitis | Often requires earlier surgical intervention due to the dense, recalcitrant nature of glycation end-product cross-linked collagen. |
| Absolute Contraindications | Active Glenohumeral Infection | Risk of systemic dissemination; requires formal I&D and antibiotics. |
| Absolute Contraindications | End-Stage Osteoarthritis | Motion loss is osseous (osteophytes, joint space loss); requires arthroplasty, not soft tissue release. |
| Relative Contraindications | Complex Regional Pain Syndrome (CRPS) | Surgical trauma may trigger a severe flare of sympathetically mediated pain. |
| Relative Contraindications | Patient Non-Compliance | Inability to participate in aggressive, daily post-operative physical therapy will result in recurrent stiffness. |
Pre-Operative Planning, Templating, and Patient Positioning
Clinical Evaluation and the Lidocaine Test
Pre-operative planning begins with a meticulous clinical examination to precisely map the patient's motion deficits. The hallmark of capsular contracture is an equal loss of both active and passive range of motion. The surgeon must systematically measure forward elevation, abduction, external rotation (both with the arm adducted and at 90 degrees of abduction), and internal rotation (measured by vertebral level reached by the thumb, or cross-chest adduction). A critical diagnostic maneuver is the intra-articular Lidocaine Injection Test. By injecting 10-20cc of local anesthetic into the glenohumeral joint, the surgeon eliminates the pain component of the patient's restriction. If the range of motion remains profoundly restricted post-injection, it confirms that structural capsular contracture, rather than pain-induced muscle guarding, is the primary pathology.
Imaging Modalities
While the diagnosis of a stiff shoulder is primarily clinical, imaging is essential to rule out structural or osseous causes of motion loss. Standard radiographs (True AP, Scapular Y, and Axillary lateral views) are mandatory to evaluate for osteoarthritis, undetected posterior dislocations, calcific tendinitis, or malunited fractures. In patients with a history of prior surgery, radiographs will identify retained hardware that may be tethering soft tissues. Magnetic Resonance Imaging (MRI) or MR Arthrography is highly valuable, particularly in secondary cases. Pathognomonic MRI findings for adhesive capsulitis include profound thickening of the coracohumeral ligament, obliteration of the subcoracoid fat triangle, and thickening of the inferior glenohumeral ligament complex with a contracted, reduced-volume axillary pouch.

Anesthesia and Patient Positioning
The choice of anesthesia and patient positioning is foundational to the success of the procedure. A regional interscalene nerve block is almost universally employed, not only for intra-operative anesthesia but critically for post-operative pain management, allowing for immediate, aggressive passive motion therapy. The surgery can be performed in either the beach chair or the lateral decubitus position, depending on surgeon preference. The lateral decubitus position, utilizing 10 to 15 pounds of longitudinal traction and a lateral counter-traction boom, is highly advantageous for capsular releases. It provides superior distraction of the tight glenohumeral joint, significantly improving visualization of the inferior recess and the critical axillary nerve danger zone.

Conversely, the beach chair position offers the advantage of an upright anatomical orientation, which some surgeons find more intuitive for subacromial and subdeltoid adhesiolysis. Regardless of the position chosen, the arm must be draped free to allow the surgeon to dynamically manipulate the limb throughout the procedure, assessing the gains in motion as each specific capsular region is systematically released.

Step-by-Step Surgical Approach and Fixation Technique
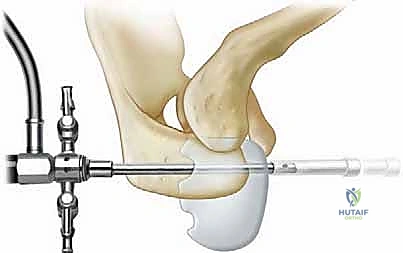
Diagnostic Arthroscopy and Joint Entry
Entering a profoundly stiff shoulder is the first major technical hurdle. The joint volume, normally 15-20cc, may be reduced to less than 5cc. The standard posterior viewing portal is established, but the surgeon must be cautious not to plunge the trocar through the contracted anterior capsule, risking injury to the subscapularis or anterior neurovascular structures. Using a blunt obturator, the joint is entered, and the arthroscope is introduced. Initial visualization is often severely limited by dense synovitis and a contracted capsule that hugs the humeral head. An anterior working portal is established via an outside-in technique using a spinal needle localized within the rotator interval, ensuring the portal is placed precisely to allow access to the anterior and inferior capsule.

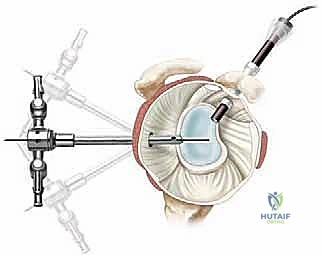
Step 1: Rotator Interval and Anterior Release
The release commences in the rotator interval, utilizing a radiofrequency (RF) ablation wand. The surgeon resects the thickened tissue bounded by the supraspinatus superiorly, the subscapularis inferiorly, and the biceps tendon. The Coracohumeral Ligament (CHL), often a dense, fibrotic band, must be completely transected to expose the base of the coracoid process. This step is paramount for restoring external rotation with the arm at the side.

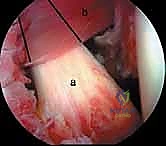
Following the interval release, the surgeon proceeds inferiorly along the anterior capsule. The Middle Glenohumeral Ligament (MGHL) is released from its glenoid origin, taking care to divide the capsule superficial to the subscapularis tendon. The critical safety maneuver here is the continuous visualization of the red, striated muscle fibers of the subscapularis belly. As long as these muscle fibers are visible deep to the capsular cut, the axillary nerve is protected. The release is carried down to the 5 o'clock position (in a right shoulder), effectively restoring external rotation in mid-abduction.

Step 2: Inferior Capsular Release (The Danger Zone)
The inferior release, addressing the IGHL complex from the 5 o'clock to the 7 o'clock position, is the most technically demanding and hazardous phase of the operation. At this juncture, the axillary nerve lies millimeters from the capsule. To mitigate risk, the surgeon must stay meticulously on the glenoid side of the capsule. The RF wand should be set to a lower power setting to minimize thermal spread, or a blunt arthroscopic scissor/basket punch can be utilized.

A highly effective technique is to use a blunt switching stick or a specialized capsular retractor introduced from the anterior portal to gently push the inferior capsule away from the underlying axillary nerve, creating a safe margin for transection. The capsule is released until the underlying fibers of the triceps tendon (long head) or the actual axillary nerve itself can be dimly visualized through the thin remaining fascial layer. Completing this inferior release is essential for restoring full forward elevation and abduction.

Step 3: Posterior Release and Subacromial Adhesiolysis
Once the inferior capsule is divided, the arthroscope is often switched to the anterior portal to view the posterior capsule. The posterior release is carried from the 7 o'clock position superiorly to the 10 o'clock position. Here, the capsule is intimately blended with the posterior rotator cuff tendons (infraspinatus and teres minor). To avoid iatrogenic injury to the cuff, the release must be performed directly adjacent to the posterior glenoid labrum. This step restores internal rotation and cross-chest adduction.

Following the intra-articular releases, the arthroscope is redirected into the subacromial space. In cases of secondary stiffness, particularly post-operative or post-traumatic, this space is often obliterated by dense, disorganized scar tissue. A thorough bursectomy and adhesiolysis are performed, clearing the plane between the acromion and the superior surface of the rotator cuff. The surgeon must also sweep laterally and anteriorly to release adhesions in the subdeltoid space, ensuring the proximal humerus can glide freely beneath the deltoid muscle during elevation.
Step 4: Judicious Manipulation Under Anesthesia (MUA)
After the arthroscopic release is complete, the arm is removed from traction, and a very gentle, controlled Manipulation Under Anesthesia (MUA) is performed to lyse any remaining, fine capsular bands. Because the primary dense structures have already been surgically divided, this manipulation requires minimal force. The surgeon gently takes the arm through forward elevation, external rotation, and internal rotation, feeling for the subtle "give" of residual adhesions. Aggressive, forceful manipulation must be strictly avoided, as it carries a high risk of iatrogenic proximal humerus fracture, glenohumeral dislocation, or severe chondral injury.

Complications, Incidence Rates, and Salvage Management
While arthroscopic capsular release is highly successful in restoring motion, it is fraught with potential complications that demand rigorous intra-operative vigilance and comprehensive pre-operative patient counseling. The complication profile varies significantly depending on whether the etiology is primary idiopathic or secondary post-traumatic/post-operative.

The most catastrophic complication is iatrogenic injury to the axillary nerve. This can occur via direct mechanical transection during the inferior release or via thermal necrosis from an RF ablation wand. Incidence rates in high-volume centers are exceedingly low (less than 1%), but the functional consequences are devastating, resulting in profound deltoid weakness and loss of active elevation. Prevention relies entirely on meticulous surgical technique: staying on the glenoid rim, visualizing the subscapularis muscle belly, and utilizing blunt dissection tools in the 6 o'clock danger zone. If a nerve injury is suspected post-operatively, an EMG should be obtained at 3-4 weeks, and early nerve exploration/grafting may be required if neurotmesis is confirmed.

Iatrogenic instability is another significant risk, particularly in patients with secondary stiffness following a prior stabilization procedure. An overzealous 360-degree capsular release can convert a stiff shoulder into a multidirectional unstable shoulder. The surgeon must carefully titrate the release, frequently assessing motion intra-operatively, and avoid releasing the anterior band of the IGHL if the patient has a history of anterior instability. Recurrent stiffness is the most common complication, occurring in 5% to 15% of patients, with the highest rates seen in insulin-dependent diabetics. Management of recurrence requires a rapid return to aggressive physical therapy, potential repeat intra-articular steroid injections, and, in refractory cases, a revision arthroscopic release.

| Complication | Estimated Incidence | Prevention & Salvage Management |
|---|---|---|
| Axillary Nerve Injury | < |
Clinical & Radiographic Imaging Archive