Arthroscopic Multidirectional Shoulder Instability Repair: A Masterclass in Capsular Plication

Key Takeaway
Join us in the OR for an immersive masterclass on arthroscopic capsular plication for multidirectional shoulder instability (MDI). We'll meticulously cover comprehensive anatomy, precise patient positioning, and a granular, step-by-step intraoperative execution of the multipleated repair technique. Learn crucial pearls and pitfalls, ensuring optimal outcomes for patients suffering from global glenohumeral laxity.
Comprehensive Introduction and Patho-Epidemiology
Multidirectional shoulder instability (MDI) represents one of the most complex and nuanced pathologies encountered by the orthopedic shoulder surgeon. Unlike unidirectional traumatic instability—often characterized by a discrete Bankart lesion and encapsulated by the TUBS acronym (Traumatic, Unidirectional, Bankart, Surgery)—MDI is defined by symptomatic glenohumeral subluxation or dislocation in more than one direction. As originally and eloquently described by Charles Neer and colleagues in 1980, MDI is fundamentally a pathology of global capsular redundancy. It represents an inherent or acquired hyperlaxity of the capsuloligamentous complex—inferiorly, posteriorly, and anteriorly—that defies simple static restraint repair. The operative philosophy here is not to merely reattach torn tissue, but to fundamentally re-engineer the capsular volume, restoring critical neuromuscular control and functional stability through precise arthroscopic plication.
The patho-epidemiology of MDI is multifaceted, often presenting as an atraumatic or microtraumatic etiology in the young, active population. The classic AMBRI acronym (Atraumatic, Multidirectional, Bilateral, Rehabilitation, Inferior capsular shift) remains a useful, albeit somewhat simplified, heuristic. Patients often possess underlying generalized ligamentous laxity, sometimes associated with connective tissue disorders such as Ehlers-Danlos or Marfan syndrome. However, a significant subset of MDI patients are overhead athletes—swimmers, gymnasts, and pitchers—who acquire global laxity through repetitive microtrauma that progressively attenuates the static restraints over time, leading to a decompensation of the dynamic stabilizers.
The natural history of untreated or poorly managed MDI can be devastating to the glenohumeral joint. Recurrent subluxations or dislocations initiate a vicious cycle of progressive chondrolabral damage. As the humeral head repeatedly translates abnormally across the glenoid face, patients develop classic Hill-Sachs lesions, progressive erosion of the anterior or posterior glenoid rim, and diffuse chondral injury. This accelerated wear pattern unfortunately predisposes these young, highly active patients to early-onset degenerative arthritis. Subjectively, these patients present with a pervasive sense of "global" shoulder instability, deep-seated pain, mechanical symptoms, and profound functional limitations in daily activities, athletics, and sleep.
Critically, surgical intervention is only considered after a comprehensive, dedicated course of nonoperative physical therapy has failed. The cornerstone of initial management must focus on periscapular strengthening and dynamic rotator cuff rehabilitation to compensate for the static ligamentous incompetence. When a patient demonstrates persistent, symptomatic instability despite a verified, high-quality rehabilitation program lasting a minimum of six months, the transition to surgical management—specifically an arthroscopic capsular plication—becomes indicated to halt the progression of joint deterioration.
Detailed Surgical Anatomy and Biomechanics
Mastery of arthroscopic capsular plication requires a profound, three-dimensional understanding of the glenohumeral joint's intricate anatomy and biomechanics. Shoulder stability relies on a highly orchestrated interplay between static ligamentous restraints and dynamic muscular stabilizers.
Static Restraints and the Ligamentous Complex
The static restraints of the shoulder form a complex capsuloligamentous network that provides end-range stability. The Inferior Glenohumeral Ligament (IGHL) complex is the most critical structure in this pathology. It functions as a hammock-like sling suspending the humeral head, consisting of an anterior band, a posterior band, and the intervening axillary pouch. The anterior band is the primary restraint against anterior translation when the arm is abducted to 90 degrees and externally rotated. Conversely, the posterior band resists posterior translation during forward flexion, adduction, and internal rotation. In the MDI patient, the hallmark anatomical finding is a profoundly patulous axillary pouch and attenuated IGHL bands, resulting in a dramatic increase in global capsular volume.
The Middle Glenohumeral Ligament (MGHL) and the superior structures play supplementary but vital roles. The MGHL primarily resists anterior translation in the mid-range of abduction (approximately 45 degrees). Superiorly, the Superior Glenohumeral Ligament (SGHL) and the Coracohumeral Ligament (CHL) form the boundaries of the rotator interval. This complex is crucial for resisting inferior translation when the arm is adducted at the side. In MDI, we frequently observe significant widening or frank defects within the rotator interval, which directly contributes to the pathognomonic inferior sulcus sign.
Understanding the osteology and articular geometry is equally vital. The glenoid fossa is relatively shallow and pear-shaped, providing a minimal articular surface area for the large humeral head—often likened to a golf ball on a tee. The labrum serves to deepen this socket by approximately 50%, enhancing the concavity-compression mechanism. While discrete Bankart lesions are less common in atraumatic MDI, diffuse labral fraying, hypoplasia, or subtle intrasubstance degeneration are frequently encountered due to chronic abnormal translation.
Dynamic Restraints and Neuromuscular Control
Dynamic stability is primarily governed by the rotator cuff musculature (supraspinatus, infraspinatus, teres minor, and subscapularis). Through coordinated, co-contractive forces, these muscles compress the humeral head directly into the center of the glenoid fossa—a biomechanical principle known as "concavity-compression." In the setting of MDI, the attenuated capsule fails to provide adequate proprioceptive feedback. This loss of mechanoreceptor function leads to delayed or discoordinated rotator cuff firing, fundamentally compromising dynamic stability.
Furthermore, the periscapular musculature (trapezius, serratus anterior, rhomboids, and levator scapulae) dictates scapulothoracic kinematics. Scapular dyskinesia is nearly ubiquitous in the MDI population. If the scapula fails to dynamically position the glenoid beneath the translating humeral head, the static capsular restraints are subjected to exponentially higher shear forces. Therefore, surgical plication must be viewed not as a standalone cure, but as a procedure that restores the baseline capsular tension required for the dynamic stabilizers and proprioceptive pathways to function normally.
Neurovascular Relationships and Surgical Danger Zones
Navigating the glenohumeral joint arthroscopically during a global capsular plication demands a healthy respect for the surrounding neurovascular structures, which are placed at significant risk during aggressive capsular shifts. The axillary nerve is the most critically vulnerable structure. Arising from the posterior cord of the brachial plexus, it courses inferior to the capsule, passing through the quadrangular space. Studies have shown the axillary nerve lies an average of only 12 to 14 millimeters from the inferior glenoid rim at the 6 o'clock position. During inferior capsular plication, taking excessively deep bites or placing portals too inferiorly can result in catastrophic iatrogenic nerve injury.
The musculocutaneous nerve, arising from the lateral cord, pierces the coracobrachialis muscle medially. While generally safe during standard posterior and superior portal placement, overly aggressive or misdirected anterior-inferior portals (such as the 5 o'clock portal) can place this nerve at risk. Additionally, the proximity of the cephalic vein and the major axillary vessels anteriorly dictates that all anterior portal tracts must be established under direct arthroscopic visualization using a spinal needle for precise localization.
Finally, the brachial plexus itself, lying medial to the coracoid process, is vulnerable to traction neuropraxia. This is primarily a positioning concern. Excessive traction weight (greater than 10-15 pounds), prolonged operative times, or improper head and neck positioning in the lateral decubitus setup can stretch the plexus. Meticulous attention to patient setup and minimizing traction weight once the joint is vented are essential preventative measures.
Exhaustive Indications and Contraindications
The decision to proceed with operative management in MDI is highly nuanced. Surgery is never the first line of treatment. The atraumatic nature of the pathology means that the underlying tissue quality is often inherently lax, making surgical outcomes less predictable than in traumatic unidirectional instability. The primary indication for surgery is persistent, symptomatic multidirectional instability that severely limits the patient's activities of daily living or athletic participation despite strict adherence to a physician-directed, physical therapist-guided rehabilitation program lasting a minimum of six months.
Differentiating true, involuntary MDI from voluntary or habitual instability is paramount. Voluntary dislocators often utilize aberrant muscle firing patterns (e.g., simultaneous latissimus dorsi and pectoralis major contraction) to subluxate the joint. These patients frequently have underlying psychological overlay or secondary gain motivations. Surgical intervention in habitual, voluntary dislocators is historically fraught with failure, high recurrence rates, and severe complications. A thorough psychological evaluation is strongly recommended if voluntary instability is suspected.
Furthermore, the presence of significant concomitant pathology may tip the scales toward surgical intervention. Patients with MDI who sustain superimposed traumatic events resulting in large bony Bankart lesions, significant glenoid bone loss (greater than 15-20%), or engaging Hill-Sachs lesions will likely fail conservative management due to the loss of the articular arc. In these cases, the surgical plan must address both the capsular redundancy and the bony defects, potentially requiring a combined arthroscopic plication and a bone-block augmentation procedure (e.g., Latarjet).
| Category | Specific Criteria |
|---|---|
| Indications for Surgery | Failure of ≥ 6 months of dedicated, high-quality physical therapy. |
| Persistent symptomatic subluxation/dislocation affecting ADLs or sports. | |
| MRI evidence of massive capsular redundancy (patulous axillary pouch). | |
| Superimposed traumatic structural lesions (Bankart, SLAP, bone loss). | |
| Disabling pain associated with documented instability episodes. | |
| Contraindications | Absolute: Voluntary/habitual instability with psychological overlay. |
| Absolute: Inability or unwillingness to comply with strict post-op rehab. | |
| Absolute: Active joint infection. | |
| Relative: Asymptomatic hyperlaxity (Beighton score > 4 without pain/instability). | |
| Relative: Severe glenoid bone loss requiring primary bony augmentation instead of soft-tissue only plication. |
Pre-Operative Planning, Templating, and Patient Positioning
Thorough preoperative planning is the absolute cornerstone of a successful arthroscopic MDI repair. This process begins with a rigorous physical examination designed to unmask the specific vectors of instability, followed by advanced imaging to precisely define the capsular volume and identify any associated intra-articular pathology.
Clinical Evaluation and Advanced Imaging
The physical examination must systematically assess generalized laxity, specific glenohumeral translation, and dynamic periscapular function. Generalized hypermobility is assessed using the Beighton criteria; a score of 4 or greater out of 9 indicates systemic laxity. The Load and Shift test is performed supine to grade anterior and posterior translation. Translation to the glenoid rim is Grade 1, over the rim with spontaneous reduction is Grade 2, and locked out over the rim is Grade 3.
The most critical test for MDI is the Sulcus Sign. With the patient's arm resting at the side in neutral rotation, inferior traction is applied. The appearance of a dimple or "sulcus" between the lateral acromion and the humeral head indicates inferior capsular laxity. Crucially, the test must be repeated with the arm in external rotation. A sulcus sign that remains Grade 2 (1-2 cm) or Grade 3 (>2 cm) in external rotation is highly pathognomonic for true multidirectional instability and indicates profound incompetence of the rotator interval and superior capsular structures.

Imaging begins with a standard radiographic series: a true Anteroposterior (Grashey) view, an axillary lateral, and a scapular Y view. Specialized views like the West Point axillary (for anterior glenoid rim deficiency) and the Stryker Notch view (for Hill-Sachs lesions) are highly recommended. However, the gold standard for soft tissue evaluation in MDI is the Magnetic Resonance (MR) Arthrogram. Intra-articular contrast distends the joint, allowing for precise quantification of the capsular volume, specifically highlighting an enlarged, redundant axillary pouch. The MR Arthrogram is also highly sensitive for detecting subtle labral pathology, rotator interval widening, and concomitant SLAP lesions that must be addressed during surgery.
Patient Positioning and Anesthesia
For arthroscopic capsular plication, the lateral decubitus position is heavily favored over the beach-chair position. The lateral decubitus setup provides unparalleled, unimpeded access to the posterior and inferior capsule, which is absolutely critical for a successful global shift.
The patient is administered a general endotracheal anesthetic, routinely supplemented with an interscalene regional nerve block to preemptively manage postoperative pain and minimize intraoperative narcotic requirements. The patient is carefully rolled onto the non-operative side. A large, inflatable beanbag is utilized to secure the torso rigidly, preventing any rolling during the procedure. The head of the bed is elevated roughly 15 to 20 degrees, and the entire table is placed in a slight reverse Trendelenburg tilt. This orientation decreases venous pressure in the shoulder, significantly reducing intraoperative bleeding and improving arthroscopic visualization.

Meticulous attention to padding is non-negotiable. An axillary roll must be placed under the dependent thorax to protect the contralateral brachial plexus. All bony prominences, particularly the common peroneal nerve at the fibular head of the down leg, must be heavily padded. The operative arm is placed into a sterile traction sleeve. Traction is applied using a specialized boom system, typically utilizing 10 to 15 pounds of weight. The arm is positioned in approximately 45 degrees of abduction and 15 to 20 degrees of forward flexion. This specific vector distracts the glenohumeral joint laterally and inferiorly, opening the subacromial space and the joint itself, creating the requisite working volume for complex suture management.
Step-by-Step Surgical Approach and Fixation Technique
The surgical execution of an arthroscopic capsular plication demands meticulous precision, advanced suture management skills, and a clear spatial understanding of the desired volumetric reduction.
Portal Placement and Diagnostic Arthroscopy
Accurate portal placement dictates the ease and safety of the entire procedure. Using a sterile marking pen, the bony landmarks are meticulously outlined: the acromion, distal clavicle, AC joint, and coracoid process. Before establishing portals, the joint is insufflated with 40 to 50 mL of sterile saline via an 18-gauge spinal needle placed posteriorly. This pushes the capsule away from the neurovascular structures and creates a fluid-filled cavity.
The standard posterior viewing portal is established approximately 2 cm inferior and 1 cm medial to the posterolateral acromial corner. An arthroscopic trocar is advanced bluntly through the deltoid and capsule. Upon entry, a thorough diagnostic sweep is performed. In MDI, the surgeon will immediately note a massive, cavernous joint space and a profoundly positive "drive-through" sign—the ability to easily pass the arthroscope from the posterior portal, across the joint, and into the anterior pouch without resistance.

Next, the anterior working portals are established under direct intra-articular visualization using spinal needle localization. An anterosuperior (AS) portal is placed just anterior to the biceps tendon, serving as a primary viewing or fluid management portal. A mid-anterior or anteroinferior (AI) portal is established just superior to the upper border of the subscapularis tendon. This AI portal must be optimized for the trajectory of suture anchors into the anterior glenoid face. Clear cannulas (typically 7.0 mm or 8.25 mm) are utilized to facilitate complex suture passage without tissue bridging.

Capsular Preparation and Tissue Mobilization
The critical first step of the plication is tissue preparation. The capsule must heal to the labrum and glenoid neck to maintain the volumetric reduction. Using an arthroscopic rasp or a motorized shaver without suction, the anterior, inferior, and posterior capsulolabral junctions are aggressively decorticated to create a robust, bleeding, biologically active bed.
If the labrum is hypoplastic or if there is a subtle Bankart variant, an arthroscopic elevator is used to mobilize the capsulolabral complex off the glenoid neck. In true atraumatic MDI, the labrum may be intact but the capsule is highly redundant. In these cases, the surgeon must ensure that the capsule is free from any adhesions that would prevent it from being shifted superiorly. A radiofrequency wand can be used carefully to release any scar tissue, but thermal shrinkage of the capsule is strongly condemned due to historical associations with high failure rates and catastrophic chondrolysis.


The Arthroscopic Capsular Plication Technique
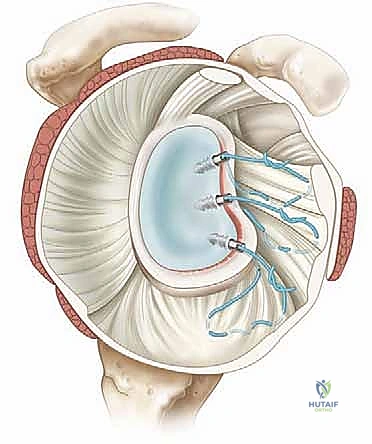
The core of the procedure is the capsulolabral plication, executing an inferior-to-superior shift. We employ a "pinch-tuck" technique. Using a 45-degree or 90-degree suture passing device (e.g., a SutureLasso or Spectrum hook) loaded with a high-strength #2 nonabsorbable suture or a shuttle relay, the surgeon pierces the capsule inferiorly and laterally, roughly 10 to 15 millimeters away from the labral edge.
The goal is to grab a substantial "bite" of the redundant axillary pouch. The suture is then passed through the intact labrum (or fixed to the glenoid rim via a suture anchor if the labrum is detached). When the knot is tied, the inferior capsule is drawn superiorly and medially, effectively obliterating the redundant recess.


This process begins at the 6 o'clock position. Extreme caution is exercised here; the suture passer must not plunge deeply into the tissue to avoid the axillary nerve. The plication proceeds sequentially up the anterior wall (5 o'clock, 4 o'clock, 3 o'clock) using either simple capsulolabral stitches or, more commonly, incorporating knotless or knotted suture anchors placed on the articular margin of the glenoid to provide rigid fixation for the shifted tissue. Each sequential stitch "chases" the laxity superiorly.

Addressing the Posterior Capsule and Rotator Interval
MDI is a global pathology; addressing only the anterior capsule guarantees failure. The arthroscope is moved to the anterior portal to view the posterior capsule. Using the posterior portal as the working channel (or establishing a 7 o'clock accessory posteroinferior portal), the posterior band of the IGHL and the posterior capsule are plicated in a similar inferior-to-superior fashion, from 6 o'clock up to 9 o'clock.


Finally, the rotator interval must be assessed and closed. If the preoperative sulcus sign was profound, interval closure is mandatory. This involves passing sutures between the SGHL/capsule superiorly and the MGHL/CHL complex inferiorly. Tying these sutures imbricates the interval, effectively shortening the superior restraints and eliminating inferior translation. Once the anterior, posterior, and interval plications are complete, the joint volume should be dramatically reduced, and the drive-through sign should be completely eliminated. The humeral head should now sit centered and compressed within the glenoid fossa.


Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique, arthroscopic management of MDI carries a distinct complication profile. The inherent poor tissue quality in this patient population makes them uniquely susceptible to both recurrent instability and iatrogenic over-constraint.
Recurrent instability is the most common complication, with literature reporting rates between 5% and 15%. Recurrence is frequently multifactorial, stemming from a failure to adequately address the posterior capsule, failure to close the rotator interval, or early non-compliance with the postoperative immobilization protocol. When recurrence happens, salvage management typically requires an open inferior capsular shift, which allows for a more aggressive, direct visualization of the tissue planes and a more robust volumetric reduction.
Conversely, over-constraint and postoperative stiffness represent the opposite end of the complication spectrum. Aggressive plication, particularly in the anterior and interval regions, can lead to a profound loss of external rotation. While a slight loss of terminal external rotation (5-10 degrees) is often an acceptable trade-off for stability, severe
