Arthroscopic Release of the Extensor Carpi Radialis Brevis for Refractory Lateral Epicondylitis: An Intraoperative Masterclass

Key Takeaway
This masterclass details arthroscopic ECRB release for chronic lateral epicondylitis. Fellows will learn patient positioning, portal placement, diagnostic arthroscopy, and meticulous débridement. We cover neurovascular risks, surgical pearls, and postoperative care, ensuring a comprehensive understanding of this effective technique for recalcitrant tennis elbow. Master the nuances for optimal patient outcomes.
Welcome, fellows and colleagues, to the operating theater. Today, we are undertaking a definitive exploration of a common yet frequently debilitating condition: recalcitrant lateral epicondylitis, colloquially known as "tennis elbow." While the vast majority of these patients respond favorably to a well-structured regimen of conservative measures, a persistent 5% to 10% will present with chronic, unrelenting symptoms that severely compromise their quality of life and occupational capacity. For this refractory subset, arthroscopic release of the extensor carpi radialis brevis (ECRB) offers a highly effective, minimally invasive, and anatomically precise solution. This intervention transcends simple debridement; it is a masterclass in applied surgical anatomy, requiring meticulous technique to eradicate pathologic tissue while rigorously preserving the critical stabilizing structures of the lateral elbow.
Comprehensive Introduction and Patho-Epidemiology
Before we proceed to the surgical theater, it is paramount to deconstruct the underlying pathology of lateral epicondylitis. Historically, the medical community mislabeled this condition as an "itis," implying a primary inflammatory cascade. However, extensive histopathological analyses, pioneered by Nirschl and Pettrone, have definitively reclassified this entity as a tendinosis—a degenerative, non-inflammatory process. The primary etiological driver is repetitive microtrauma localized to the origin of the ECRB muscle, which induces microscopic tearing of the tendinous fibers. This repetitive mechanical overload outpaces the tissue's intrinsic regenerative capacity, initiating a flawed and aborted healing response.
At the cellular level, this flawed healing manifests as the ingrowth of weakened, disorganized reparative tissue, a phenomenon pathognomonically termed angiofibroblastic hyperplasia or angiofibroblastic tendinosis. Macroscopically, normal glistening, white, longitudinally oriented collagen is replaced by gray, friable, edematous tissue. Microscopically, one observes a paucity of traditional inflammatory cells (macrophages, neutrophils) and an abundance of disorganized collagen arrays, hypercellularity with immature fibroblasts, and non-functional vascular hyperplasia. This profound histological reality explains the frequent failure of anti-inflammatory medications and corticosteroid injections to provide anything beyond transient, symptomatic relief; they do not address the underlying structural degeneration.
The clinical spectrum of ECRB tendinosis is highly variable, ranging from microscopic fraying to macroscopic, partial-thickness interstitial tearing, and ultimately, complete tendon failure if left unaddressed. While the ECRB is the undisputed primary culprit due to its unique biomechanical role and anatomic location crossing multiple joints, chronic cases can demonstrate an extension of this degenerative process. The anterior portion of the extensor digitorum communis (EDC) may become involved, compounding the patient's pain profile. It is crucial to distinguish this lateral pathology from medial epicondylitis ("golfer's elbow"), which implicates the flexor pronator mass and requires an entirely different diagnostic and therapeutic algorithm.
Detailed Surgical Anatomy and Biomechanics
A profound, three-dimensional understanding of the lateral elbow anatomy is the absolute prerequisite for safe and effective arthroscopic intervention. The lateral epicondyle serves as the critical osteological epicenter. The common extensor tendon origin, a complex confluence of four distinct myotendinous units, anchors here. Navigating this confluence requires an intimate knowledge of the layered anatomy.
The Extensor Carpi Radialis Brevis (ECRB) is our primary surgical target. Its origin is situated on the distal anterolateral aspect of the lateral epicondyle, covering a footprint of approximately 1.5 square centimeters. Crucially for the arthroscopist, the ECRB lies deep to the other components of the extensor mass. Intra-articularly, we identify the ECRB as the muscle belly and tendinous tissue lying immediately superficial to a thinned-out portion of the anterolateral joint capsule. It is bordered superficially by the Extensor Digitorum Communis (EDC), the Extensor Digiti Minimi (EDM), and the Extensor Carpi Ulnaris (ECU).
It is of paramount importance to differentiate the ECRB from the Extensor Carpi Radialis Longus (ECRL). The ECRL originates significantly more proximally, arising from the lateral humeral supracondylar ridge, approximately 2 to 3 centimeters superior to the common extensor tendon origin. It courses distally, lying anterior and superficial to the ECRB. The ECRL is the primary power extensor of the wrist; inadvertent iatrogenic damage to this structure during ECRB release will result in profound deficits in grip strength and wrist extension, a complication that is entirely avoidable with precise anatomical orientation.

Deep to the extensor tendon complex lies the most critical stabilizing structure of the lateral elbow: the Lateral Ulnar Collateral Ligament (LUCL). This primary restraint to posterolateral rotatory instability originates from the isometric point on the lateral epicondyle, blends seamlessly with the lateral joint capsule, and courses distally to insert onto the supinator crest of the proximal ulna. During arthroscopic ECRB release, the surgeon must operate meticulously anterior and superior to the LUCL equator. Any iatrogenic transection or thermal injury to the LUCL will precipitate posterolateral rotatory instability (PLRI), a devastating complication necessitating complex ligamentous reconstruction.
Neurovascular Structures at Risk
While arthroscopy of the elbow is generally safe when adhering to established portals, the proximity of major neurovascular structures demands unwavering vigilance. The Radial Nerve represents the primary structure at risk, particularly when establishing lateral working portals. The nerve pierces the lateral intermuscular septum to enter the anterior compartment, coursing anterior to the radiocapitellar joint before bifurcating into the superficial sensory branch and the deep posterior interosseous nerve (PIN). The PIN subsequently dives into the Arcade of Frohse within the supinator muscle.
Anatomical studies utilizing the proximal anterolateral portal—our preferred working portal—demonstrate that the radial nerve lies, on average, 13.7 mm from the arthroscopic cannula, compared to a mere 7.2 mm when utilizing the standard anterolateral portal. This increased distance provides a vital margin of safety. Furthermore, when establishing the proximal anteromedial viewing portal, the medial antebrachial cutaneous nerve and superficial basilic veins are vulnerable; therefore, the initial incision must strictly penetrate only the dermis, followed by blunt dissection with a hemostat to the joint capsule to displace these superficial structures safely.
Exhaustive Indications and Contraindications
The decision to proceed with arthroscopic surgical intervention must be predicated on a rigorous, evidence-based assessment of the patient's clinical trajectory. Surgery is never a first-line treatment for lateral epicondylitis. The natural history of this condition is largely self-limiting, with up to 90% of patients experiencing spontaneous resolution within 12 to 18 months through conservative measures alone. Therefore, surgical candidacy is strictly reserved for those who have failed a comprehensive, multi-modal conservative regimen.
Indications for arthroscopic release include a confirmed clinical diagnosis of lateral epicondylitis with debilitating symptoms persisting for a minimum of 6 months despite appropriate non-operative management. This management should include, but is not limited to, activity modification, non-steroidal anti-inflammatory drugs (NSAIDs), physical therapy focusing on eccentric strengthening, counterforce bracing, and potentially, corticosteroid or orthobiologic (PRP) injections. Furthermore, the patient must exhibit localized tenderness over the ECRB origin and positive provocative testing (e.g., Cozen's test, Maudsley's test).
Contraindications must be carefully evaluated to prevent catastrophic outcomes. Absolute contraindications include active local or systemic infection, severe distortion of the bony or soft tissue anatomy (such as from previous trauma or heterotopic ossification) that precludes safe portal placement, and the presence of medial hardware or previous ulnar nerve transposition that would jeopardize the safe establishment of the proximal anteromedial portal.
Table of Indications and Contraindications
| Category | Specific Criteria | Rationale |
|---|---|---|
| Primary Indications | Refractory symptoms > 6 months | Ensures adequate trial of natural healing and conservative care. |
| Failure of comprehensive conservative therapy | Confirms that non-operative modalities (PT, bracing, injections) are insufficient. | |
| Concomitant intra-articular pathology | Arthroscopy allows simultaneous treatment of loose bodies, synovitis, or chondral defects. | |
| Relative Contraindications | Prior open lateral elbow surgery | Altered anatomy increases the risk of neurovascular injury and LUCL compromise. |
| Severe elbow stiffness/arthrofibrosis | Limits joint distension and safe arthroscopic maneuverability. | |
| Absolute Contraindications | Active local cellulitis or joint infection | High risk of seeding infection throughout the joint and systemic circulation. |
| Altered medial anatomy (e.g., ulnar nerve transposition) | Precludes safe establishment of the proximal anteromedial viewing portal. |
Pre-Operative Planning, Templating, and Patient Positioning
Thorough preoperative planning is the cornerstone of a successful arthroscopic ECRB release. The diagnostic workup relies heavily on a meticulous physical examination. The hallmark finding is exquisite point tenderness directly over the lateral epicondyle and the ECRB footprint. Provocative maneuvers are essential: Cozen's test (resisted wrist extension with the elbow in extension) and Mill's test (passive wrist flexion with the elbow in extension) will reliably reproduce the patient's lateral pain. Additionally, Maudsley's test (resisted middle finger extension) is highly specific for ECRB pathology, though it must be carefully differentiated from Posterior Interosseous Nerve (PIN) entrapment (Radial Tunnel Syndrome), which typically presents with tenderness more distal in the extensor muscle belly and is primarily a compressive neuropathy rather than a tendinopathy.
Imaging, while secondary to the clinical exam, is vital for surgical planning and ruling out concomitant pathology. Standard anteroposterior (AP) and lateral radiographs of the elbow are obtained to assess for radiocapitellar osteoarthritis, loose bodies, or calcification within the extensor origin—a finding present in up to 25% of chronic cases. Magnetic Resonance Imaging (MRI), particularly T2-weighted and STIR sequences, is highly sensitive for demonstrating ECRB tendinosis, visualized as thickening, intermediate-to-high signal intensity, and peritendinous edema at the lateral epicondyle footprint. MRI is also invaluable for identifying unsuspected LUCL tears or occult osteochondral lesions of the capitellum.

Anesthesia and Patient Positioning
The procedure is routinely performed under general anesthesia. General anesthesia guarantees complete muscular paralysis, which is absolutely critical for adequate joint distension, safe portal placement, and unimpeded manipulation of arthroscopic instruments within the tight confines of the elbow joint. Regional anesthesia (interscalene or supraclavicular block) may be utilized as an adjunct for postoperative pain control, provided a thorough pre-operative neurological exam is documented.
Patient positioning is a critical variable in elbow arthroscopy. We advocate for the prone position. The patient is placed prone with the operative arm supported by a specialized arm holder or a well-padded sandbag positioned under the proximal humerus. The elbow is allowed to flex to exactly 90 degrees, hanging freely over the edge of the operating table. This prone, 90-degree flexed position is highly advantageous: it allows gravity to naturally distract the radiocapitellar joint, it allows the neurovascular structures (specifically the radial and brachial bundles) to fall anteriorly away from the joint capsule, and it provides the surgeon—who is comfortably seated—with highly ergonomic access to both the medial and lateral compartments.
Prior to sterile preparation and draping, a comprehensive Examination Under Anesthesia (EUA) is mandatory. The surgeon must assess the elbow for full, unrestricted range of motion (flexion, extension, pronation, supination) and perform a definitive lateral pivot-shift test to rule out any pre-existing posterolateral rotatory instability that may have been masked by patient guarding in the clinic.

Step-by-Step Surgical Approach and Fixation Technique
The arthroscopic release of the ECRB is a procedure of precision. Following standard sterile prep and drape, a sterile tourniquet is applied high on the brachium but is generally not inflated unless visualization becomes compromised by persistent bleeding. The joint is first maximally distended by injecting 20 to 30 cc of sterile normal saline through the soft spot (the center of the triangle formed by the lateral epicondyle, radial head, and olecranon tip) to push the neurovascular structures safely away from the capsule.
Establishing the Portals
We begin by establishing the Proximal Anteromedial Portal. The anatomical landmark is 2 cm proximal and 1 cm anterior to the medial epicondyle. A superficial skin incision is made using a #11 blade. Subcutaneous tissues are bluntly dissected with a mosquito hemostat, spreading longitudinally to protect the medial antebrachial cutaneous nerve, until the firm resistance of the anterior joint capsule is felt. The blunt trocar and arthroscopic cannula are then directed toward the radial head, entering the joint. A 4.0-mm, 30-degree arthroscope is introduced to achieve a panoramic view of the anterior compartment.
Next, under direct intra-articular visualization, the Proximal Anterolateral Portal is established. A spinal needle is introduced 2 cm proximal and 1 cm anterior to the lateral epicondyle, aiming towards the center of the joint. The needle must enter the joint anterior to the radiocapitellar articulation. Once the trajectory is confirmed to be safe and optimal for accessing the lateral capsule, a skin incision is made, and a working cannula is introduced using the same blunt dissection technique to protect the radial nerve.
Diagnostic Sweep and Capsular Resection
A thorough diagnostic arthroscopy is performed, inspecting the coronoid, the trochlea, the radial head, and the capitellum for chondromalacia or loose bodies. The arthroscope is then directed laterally to visualize the radiocapitellar joint and the overlying lateral joint capsule.
The first step in addressing the ECRB is the precise resection of the lateral joint capsule. Using a radiofrequency ablation wand or a 4.0-mm motorized shaver introduced through the proximal anterolateral portal, a window is meticulously created in the lateral capsule, directly superior to the equator of the radial head and anterior to the lateral epicondyle.

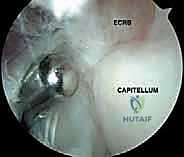
As the capsular window is expanded, the undersurface of the ECRB tendon and its muscle belly become vividly apparent. The pathologic angiofibroblastic tissue of the ECRB is easily distinguished from normal tendon; it appears gray, frayed, and friable, lacking the organized, glistening, longitudinal striations of healthy collagen.
ECRB Release and Decortication
The core of the procedure is the selective debridement and release of this pathologic ECRB origin. Utilizing the motorized shaver (oscillating mode, aggressive teeth) and the radiofrequency wand, the diseased ECRB tissue is resected from its footprint on the lateral epicondyle. The release is carried superiorly until the healthy, muscular fibers of the ECRL are visualized, and anteriorly to the border of the EDC.
Throughout this resection, the surgeon must remain hyper-vigilant of the LUCL. The LUCL is located posterior and inferior to the ECRB footprint. The golden rule of this procedure is to never allow the shaver or ablation wand to drift posterior to the equator of the radial head. Doing so risks catastrophic transection of the LUCL.
Once the pathologic ECRB tissue is completely excised, exposing the bare bone of the lateral epicondyle, we proceed to decortication. A motorized burr or a microfracture awl is used to gently decorticate the footprint, removing the sclerotic cortical bone to expose the underlying bleeding cancellous bone bed. This controlled marrow stimulation releases mesenchymal stem cells and local growth factors, theoretically promoting a robust, vascularized healing response at the extensor origin.
Following decortication, the joint is thoroughly irrigated to remove all osseous and soft tissue debris. The arthroscope is removed, the portals are closed with simple interrupted non-absorbable sutures, and a sterile, compressive soft dressing is applied.
Complications, Incidence Rates, and Salvage Management
While arthroscopic ECRB release boasts a high success rate and a low overall morbidity profile, complications, when they occur, can be severe and technically demanding to salvage. A rigorous understanding of potential pitfalls is mandatory for any surgeon performing this procedure.
The most feared and devastating complication is Iatrogenic Posterolateral Rotatory Instability (PLRI). This occurs due to inadvertent transection or thermal necrosis of the Lateral Ulnar Collateral Ligament (LUCL) during the capsular resection or ECRB debridement. The incidence is reported to be less than 1% in experienced hands, but the functional consequence is profound. Patients will present postoperatively with mechanical catching, a sense of the elbow "giving way" during terminal extension and supination, and a positive pivot-shift test. Salvage management requires an open, complex LUCL reconstruction utilizing autograft (typically palmaris longus or gracilis) or allograft tissue.
Neurological Injury is another critical concern. The radial nerve, specifically its deep branch (the PIN), is at risk during the establishment of the lateral portals and during aggressive lateral capsular release. The medial antebrachial cutaneous nerve is at risk during medial portal placement. Adherence to strict anatomical landmarks, utilizing the "proximal" portal variations, and employing blunt dissection techniques down to the capsule drastically minimizes this risk. Transient neurapraxias generally resolve with observation, but structural nerve transection necessitates microsurgical exploration and repair.

Table of Complications and Salvage Management
| Complication | Estimated Incidence | Etiology / Mechanism | Salvage Management |
|---|---|---|---|
| Iatrogenic PLRI | < 1 - 2% | Transection of the LUCL during posterior/inferior debridement. | Open LUCL reconstruction with autograft/allograft. |
| Radial Nerve / PIN Injury | < 1% | Poor lateral portal placement; excessive anterior capsular release. | EMG/NCS at 6 weeks; microsurgical exploration if structural injury suspected. |
| Incomplete Release / Recurrence | 3 - 5% | Failure to adequately resect all angiofibroblastic ECRB tissue. | Revision arthroscopy or open Nirschl procedure. |
| Arthrofibrosis / Stiffness | 2 - 4% | Prolonged immobilization; excessive intra-articular bleeding. | Aggressive physical therapy; eventual arthroscopic capsular release if refractory. |
| Superficial Portal Infection | < 1% | Standard surgical site infection. | Oral antibiotics; local wound care. |
Phased Post-Operative Rehabilitation Protocols
The surgical intervention is only the first phase of the patient's recovery; a meticulously structured, phased rehabilitation protocol is essential to optimize outcomes, prevent stiffness, and ensure a safe return to functional activities. The protocol is designed to protect the healing microenvironment while progressively restoring range of motion and load-bearing capacity.
Phase I: Protection and Early Motion (Weeks 0 to 2)
Immediately postoperatively, the elbow is placed in a soft, bulky compressive dressing to minimize hemarthrosis and edema. A rigid splint is generally avoided to prevent stiffness. The patient is encouraged to begin immediate, gentle, active-assisted range of motion (ROM) exercises for the elbow (flexion and extension) and forearm (pronation and supination) within a pain-free arc. Wrist ROM and gripping exercises are strictly prohibited during this phase to avoid placing tension on the healing extensor origin. Cryotherapy is utilized aggressively.
Phase II: Progressive Strengthening and Tissue Loading (Weeks 2 to 6)
Sutures are removed at the 10-to-14-day mark. The focus shifts to restoring full, terminal range of motion. Once full ROM is achieved, isometric strengthening of the wrist extensors and flexors is initiated. By week 4, the patient transitions to light, concentric isotonic exercises. Modalities such as soft tissue mobilization and ultrasound may be employed by the physical therapist to manage scar tissue formation and promote linear collagen alignment at the decorticated footprint.
Phase III: Return to Sport and Heavy Labor (Weeks 6 to 12+)
The final phase introduces eccentric strengthening of the wrist extensors, which is critical for remodeling the tendinous tissue and increasing its tensile strength. Plyometric exercises and sport-specific or occupation-specific functional training are gradually integrated. Patients are typically cleared to return to full, unrestricted activities, including racquet sports or heavy manual labor, between 8 and 12 weeks postoperatively, provided they have achieved symmetrical grip strength and are entirely pain-free during provocative maneuvers.
Summary of Landmark Literature and Clinical Guidelines
The evolution of surgical management for lateral epicondylitis is deeply rooted in robust clinical literature. The foundational understanding of the pathology was established by Nirschl and Pettrone (1979), whose seminal work defined the histological characteristics of angiofibroblastic hyperplasia and described the classic open surgical release, which remains the gold standard against which all minimally invasive techniques are measured.
The transition to arthroscopic management gained significant traction following the work of Baker et al. (2000), who published long-term outcomes demonstrating that arthroscopic ECRB release yielded results comparable, if not superior, to open techniques, with the added benefits of accelerated rehabilitation, decreased postoperative pain, and the ability to address concomitant intra-articular pathology. Their cohort demonstrated a 95% success rate with minimal complications.
Current clinical guidelines from the American Academy of Orthopaedic Surgeons (AAOS) and the Arthroscopy Association of North America (AANA) support arthroscopic release as a highly efficacious intervention for appropriately selected patients who have failed a minimum of 6 months of comprehensive non-operative care. The literature consistently emphasizes that the key to success lies not only in the complete resection of the pathologic ECRB tissue but in the meticulous preservation of the LUCL and the precise avoidance of neurovascular structures. By adhering to the anatomical principles and surgical techniques detailed in this chapter, the orthopedic surgeon can reliably restore function and alleviate the chronic burden of refractory lateral epicondylitis.
