Is distal clavicle resection the fix for your AC joint pain?

Key Takeaway
In this comprehensive guide, we discuss everything you need to know about Is distal clavicle resection the fix for your AC joint pain?. Distal clavicle resection is a surgical procedure removing a small portion of the distal clavicle, often indicated for chronic acromioclavicular (AC) joint pain or arthritis. AC joint injuries, which involve about 9% of shoulder girdle damage, result from direct trauma, affecting ligaments and muscles, causing pain in the AC joint, especially with cross-arm adduction.
Comprehensive Introduction and Patho-Epidemiology
Acromioclavicular (AC) joint injuries represent a significant proportion of shoulder pathology, accounting for approximately 9% of all shoulder girdle injuries encountered in orthopedic practice. These injuries predominantly affect young, active individuals, particularly athletes engaged in contact sports such as football, hockey, and rugby, as well as those involved in high-velocity activities like cycling and skiing. The fundamental question of whether distal clavicle resection serves as the definitive solution for AC joint pain requires a nuanced understanding of the injury's patho-epidemiology, differentiating between isolated degenerative arthrosis and complex biomechanical instability. The injury pattern is classically sequential, initiating with the disruption of the acromioclavicular ligaments, progressing to the robust coracoclavicular (CC) ligaments, and ultimately, in severe cases, involving the deltoid and trapezial muscle fascia.

The primary mechanism of injury is direct trauma to the lateral aspect of the shoulder with the arm in an adducted position. This force drives the acromion inferiorly and medially, while the clavicle is stabilized by the sternoclavicular joint and robust cervical musculature, resulting in a shearing force across the AC and CC ligaments. Less frequently, an indirect mechanism occurs via a fall on an outstretched hand or elbow; this transmits an axial load through the humerus, driving the humeral head superiorly into the acromion and disrupting the AC joint from inferior to superior. This indirect mechanism is often associated with concomitant intra-articular glenohumeral pathology, such as Superior Labrum Anterior and Posterior (SLAP) tears, which must be meticulously ruled out during clinical evaluation.

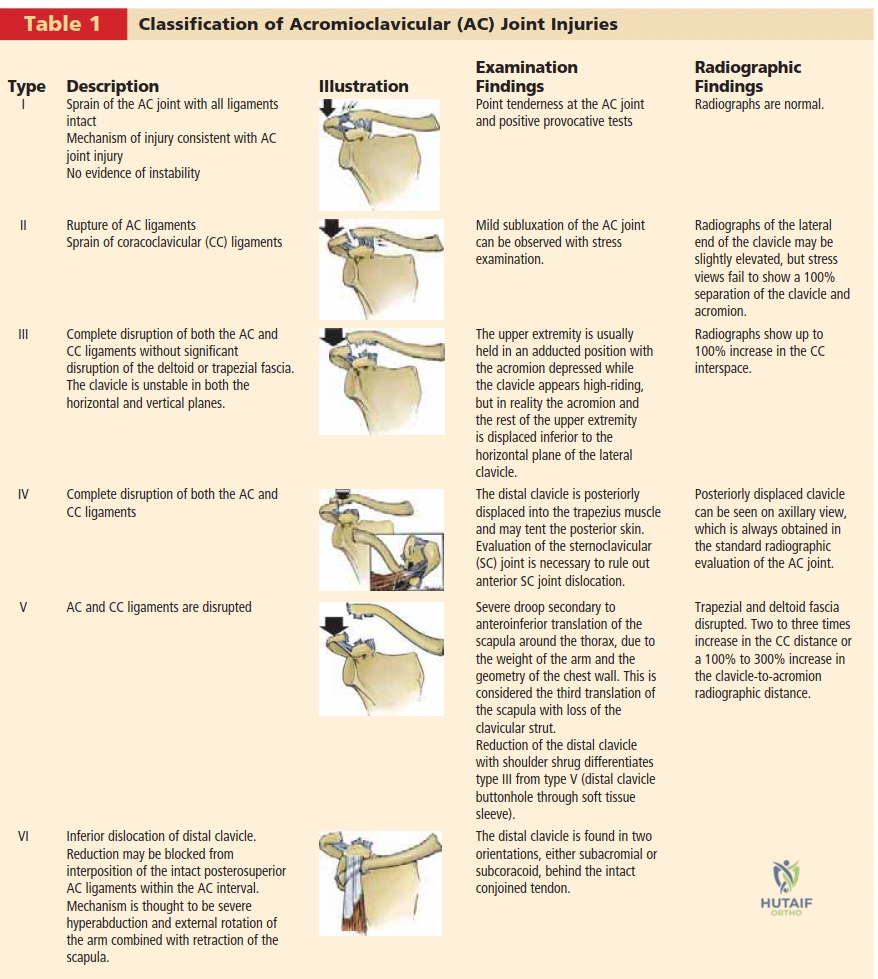
The natural history of AC joint injuries is highly dependent on the severity of the initial insult, classically categorized by the Rockwood classification system (Types I through VI). Most patients with Type I or Type II AC joint separations achieve full functional recovery with conservative management and exhibit no long-term sequelae. However, a clinically significant subset—up to 27% of patients with Type I and II injuries—develop persistent, functionally limiting pain secondary to post-traumatic arthrosis, meniscal tearing, or subtle dynamic instability, ultimately necessitating surgical intervention such as a distal clavicle resection. Conversely, high-grade injuries (Types IV, V, and VI) uniformly do poorly without operative intervention, as the chronically dislocated AC joint and severe soft tissue disruption lead to intractable pain, scapular dyskinesia, and profound upper extremity weakness.
Type III injuries remain the most controversial subset in orthopedic sports medicine. While historical consensus and surveys of Major League Baseball team physicians suggest that up to 80% of athletes treated nonoperatively achieve complete pain relief and normal function, heavy laborers and elite overhead athletes may experience up to a 17% decrease in bench press strength and persistent posterior instability. In these scenarios, the clinician must carefully determine if the patient's pain is generated by localized AC joint impingement—amenable to distal clavicle resection—or by gross CC ligamentous incompetence, which requires a comprehensive anatomic reconstruction to restore normal scapulothoracic kinematics.
Detailed Surgical Anatomy and Biomechanics
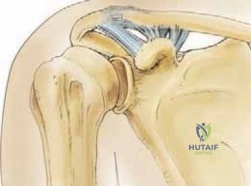
The acromioclavicular joint is a complex, diarthrodial joint that serves as the sole skeletal articulation between the axial skeleton (via the clavicle) and the upper extremity. Biomechanically, it functions not merely as a static hinge, but as a dynamic pivot point allowing the scapula to protract, retract, elevate, and depress. Normal scapular motion is heavily reliant on the AC joint, consisting of substantial rotations around three distinct axes. The articular surfaces are uniquely composed of hyaline cartilage in youth, which rapidly transitions to fibrocartilage by the second decade of life. Interposed between these surfaces is an intra-articular meniscoid structure that aids in load distribution; however, this meniscus typically undergoes rapid degenerative changes and is often functionally absent by the fourth decade, predisposing the joint to early osteoarthrosis.
Stability of the AC joint is conferred by a sophisticated interplay of static and dynamic stabilizers. The static stabilizers are primarily the AC capsule and its intrinsic ligaments (superior, inferior, anterior, and posterior), alongside the robust extracapsular coracoclavicular (CC) ligaments. The AC joint capsule and the superior/posterior AC ligaments are the primary restraints to anterior-to-posterior (horizontal) translation of the distal clavicle. Meticulous biomechanical studies have demonstrated that the superior AC ligament is the most robust, and its preservation or reconstruction is critical to preventing posterior displacement of the clavicle into the scapular spine.
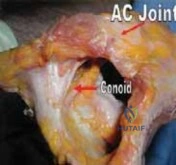
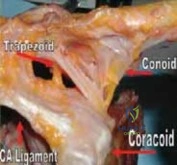
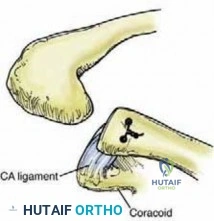
The coracoclavicular ligaments—composed of the conoid and trapezoid—span the coracoclavicular space (normally measuring 1.1 to 1.3 cm) and are the primary restraints to superior-to-inferior (vertical) translation. Appreciating their precise anatomic footprint is paramount for anatomic reconstruction. The trapezoid originates on the superior aspect of the coracoid and attaches to the undersurface of the clavicle at an anterolateral position. The conoid is a broad, stout, cone-shaped ligament located posteromedially, inserting on the conoid tubercle of the clavicle. Both ligaments are situated posterior to the pectoralis minor attachment on the coracoid. Biomechanically, the conoid ligament experiences the highest in situ forces under superior loads. If the AC ligaments are transected, the conoid becomes the primary restraint to anterior loads, while the trapezoid serves as the primary restraint to posterior loads.

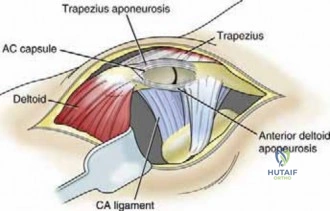
The dynamic stabilizers of the AC joint consist of the robust fascial expansions of the deltoid and trapezius muscles, which blend intimately with the superior AC joint capsule. Disruption of this deltotrapezial fascia, as seen in high-grade Rockwood injuries, dramatically exacerbates instability and requires meticulous surgical repair. Furthermore, the innervation of the AC joint is dual, supplied by branches of the lateral pectoral nerve and the suprascapular nerve. This dual innervation pattern complicates the clinical picture; while suprascapular nerve fibers transmit typical superior shoulder pain, the lateral pectoral nerve branches can refer pain to the anteromedial chest wall, mimicking primary glenohumeral or even cardiopulmonary pathology.

Exhaustive Indications and Contraindications
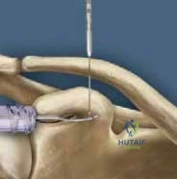
The decision to proceed with surgical intervention—specifically distal clavicle resection with or without CC ligament reconstruction—relies on a rigorous clinical evaluation and a clear understanding of the patient's functional demands. Pathology of the AC joint is classically identified by a diagnostic triad: localized point tenderness directly over the joint, provocation of deep pain with cross-arm adduction (the Scarf test), and complete relief of symptoms following a targeted intra-articular injection of a local anesthetic. Pain localized to the trapezius region and anterolateral deltoid is highly specific for AC joint injury, whereas pain radiating down the lateral deltoid to the deltoid tuberosity is more indicative of subacromial impingement or rotator cuff pathology.
Physical examination must be exhaustive. The AC joint compression (shear) test—eliciting isolated painful movement at the AC joint in conjunction with a history of direct trauma—is highly sensitive. The Paxinos test, performed by applying anterior pressure to the mid-acromion and posterior pressure to the distal clavicle, is an excellent provocative maneuver for AC joint arthrosis and subtle instability. The O’Brien active compression test can also elicit AC joint pain; however, the examiner must carefully differentiate superior joint pain (indicative of AC pathology) from deep anterior glenohumeral pain (suggestive of SLAP or biceps pathology).
Distal clavicle resection alone (the Mumford procedure) is strictly indicated for isolated, symptomatic AC joint arthrosis, post-traumatic osteolysis of the distal clavicle, or chronic Type I/II injuries that have failed exhaustive conservative management (minimum of 3 to 6 months). It is critically important to recognize that performing an isolated distal clavicle resection in the setting of CC ligament incompetence (Type III-VI injuries) is a profound biomechanical error that will exacerbate instability and lead to catastrophic surgical failure. In these unstable scenarios, distal clavicle resection must be coupled with a robust coracoclavicular ligament reconstruction (e.g., ACCR or modified Weaver-Dunn).
Contraindications to surgical intervention must be carefully weighed. Absolute contraindications include active local or systemic infection, medical comorbidities precluding anesthesia, and lack of patient compliance required for a stringent postoperative rehabilitation protocol. Relative contraindications include painless hyperlaxity, isolated scapular dyskinesia without structural AC joint pathology, and concurrent cervical spine radiculopathy that mimics shoulder pain. The differential diagnosis is broad and must systematically exclude cervical spine pathology, trapezial spasm, distal clavicle or acromion fractures, coracoid fractures, thoracic outlet syndrome, and intrinsic glenohumeral pathology.
| Indication Category | Specific Clinical Scenarios | Recommended Surgical Approach |
|---|---|---|
| Degenerative / Arthrosis | Primary osteoarthritis, Post-traumatic osteolysis, Refractory Type I/II pain | Isolated Distal Clavicle Resection (Arthroscopic or Open) |
| Acute Instability (High Grade) | Acute Type IV, V, VI separations; Type III in elite overhead athletes | CC Ligament Reconstruction +/- Distal Clavicle Resection |
| Chronic Instability | Symptomatic chronic Type III-VI with persistent pain/dyskinesia > 3 months | Distal Clavicle Resection WITH Coracoclavicular Reconstruction |
| Contraindications | Active infection, painless deformity, non-compliant patient, isolated GH pathology | Nonoperative Management / Treat underlying pathology |
Pre-Operative Planning, Templating, and Patient Positioning
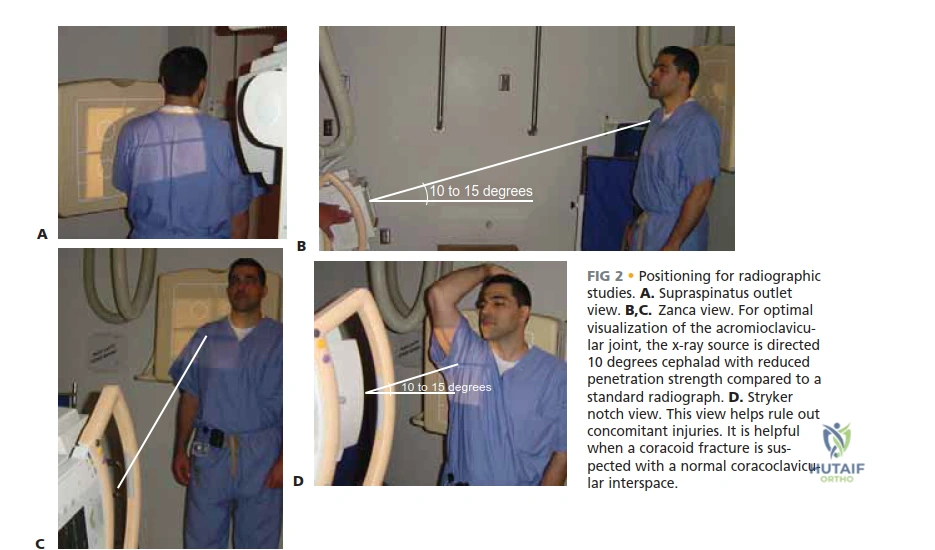
Pre-operative planning for AC joint surgery demands a meticulous radiographic evaluation to quantify the degree of instability, assess for degenerative changes, and rule out concomitant fractures. Standard shoulder radiographs, including a true anteroposterior (AP) view, a supraspinatus outlet view, and an axillary lateral view, are mandatory. However, because the AC joint is superficial and surrounded by significantly less soft tissue mass than the glenohumeral joint, standard penetration strength often overexposes the distal clavicle. Therefore, radiographs must be obtained with reduced penetration (approximately 50% less kilovoltage) to properly visualize the fine trabecular detail of the distal clavicle and acromion.
The Zanca view is the absolute gold standard for evaluating AC joint pathology. This specialized view is obtained by tilting the x-ray beam 10 to 15 degrees in a cephalic direction, effectively projecting the AC joint clear of the dense scapular spine. On this view, the normal AC joint width measures 1 to 3 mm, though this decreases naturally with age. The coracoclavicular distance (normally ~1.3 cm) must be scrutinized; an increase of 25% to 50% compared to the contralateral normal shoulder indicates complete disruption of the CC ligaments. While historical practice included weighted stress views (suspending 5 to 10 pounds from the ipsilateral wrist), this is now rarely necessary and often poorly tolerated by acute trauma patients.

Advanced imaging is frequently utilized to complete the preoperative workup. An axial view of the shoulder is critical for differentiating a Type III (vertical instability) from a Type IV injury (posterior displacement of the clavicle into or through the trapezius muscle). Furthermore, if a normal coracoclavicular interspace is observed in conjunction with a complete dislocation of the AC joint, the surgeon must maintain a high index of suspicion for a coracoid base fracture; a Stryker notch view or computed tomography (CT) scan is highly diagnostic in this scenario. Magnetic resonance imaging (MRI) is invaluable for assessing the integrity of the deltotrapezial fascia and ruling out concomitant intra-articular pathology, such as SLAP lesions, which have been frequently cited as a primary cause of failed isolated distal clavicle resections.
Patient positioning is a critical step that dictates surgical flow and visualization. Following the induction of general anesthesia, the patient is placed in the beach-chair position. While specialized shoulder tables are available, a standard operating table is often preferred as it provides excellent posterior support and stabilization of the scapula. A small bump (rolled towel or intravenous fluid bag) is strategically placed along the medial border of the scapula; this serves to stabilize the scapulothoracic articulation and protract the shoulder girdle, bringing the coracoid process more anteriorly for easier surgical access. The head must be securely positioned but remain mobile enough to allow for repositioning if necessary during clavicle reaming or drilling. The operative arm is draped free from the sternoclavicular joint laterally, allowing for full intraoperative manipulation.

Step-by-Step Surgical Approach and Fixation Technique
The surgical management of AC joint pathology has evolved significantly, transitioning from non-anatomic salvage procedures to highly sophisticated, biomechanically sound anatomic reconstructions. The primary goals of any surgical intervention at the AC joint are to achieve a pain-free shoulder, restore full range of motion and strength, and permit unrestricted return to activities. When addressing chronic AC joint pain with distal clavicle resection, the surgeon must first decide whether the procedure will be performed open or arthroscopically, and critically, whether a concomitant CC ligament reconstruction is required. Missed instability is the nemesis of the isolated Mumford procedure.

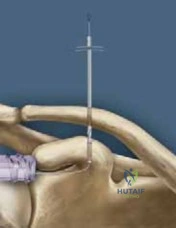
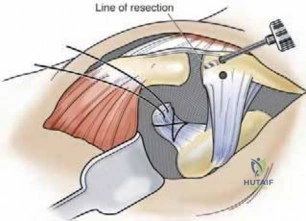
For isolated AC joint arthrosis, an arthroscopic distal clavicle resection is often the procedure of choice. This approach allows for a comprehensive diagnostic arthroscopy of the glenohumeral joint to address concomitant pathology (e.g., SLAP repairs, labral debridement). The arthroscope is introduced into the subacromial space, and the AC joint is identified via its capsular reflection. A radiofrequency wand is used to meticulously clear the inferior capsule, taking great care to preserve the superior and posterior AC ligaments, which are the primary restraints to horizontal instability. A motorized burr is then utilized to resect approximately 5 to 8 mm of the distal clavicle. Resecting more than 10 mm risks destabilizing the joint by violating the conoid and trapezoid ligament insertions, leading to iatrogenic instability.

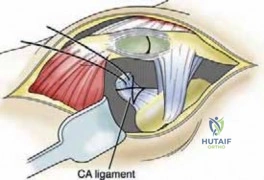
In cases of chronic instability (Types IV-VI, or symptomatic Type III), distal clavicle resection must be combined with a stabilization procedure. The modified coracoacromial (CA) ligament transfer, known as the Weaver-Dunn procedure, was historically considered the gold standard. In this open technique, the distal 1 cm of the clavicle is resected. The CA ligament is detached from its acromial insertion and transferred into the medullary canal of the distal clavicle. However, biomechanical studies have demonstrated that the transferred CA ligament possesses only 20% of the native strength of the intact CC ligaments. Consequently, the Weaver-Dunn procedure is frequently augmented with heavy non-absorbable sutures or tape passed around the coracoid and through drill holes in the clavicle to protect the ligament transfer during the biological healing phase.

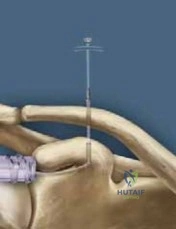
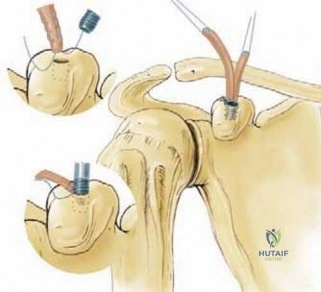
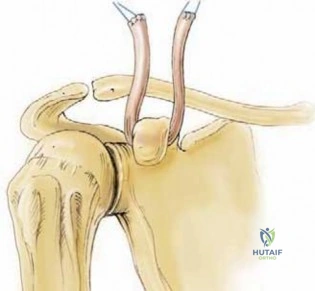
Modern orthopedics has largely shifted toward Anatomic Coracoclavicular Reconstruction (ACCR). This technique attempts to perfectly recreate the native anatomy and biomechanics of the conoid and trapezoid ligaments using a free tendon graft (typically a semitendinosus autograft or allograft). Following a conservative distal clavicle resection, bone tunnels are drilled in the clavicle at the exact anatomic footprints of the conoid (posteromedial) and trapezoid (anterolateral). The graft is looped under the base of the coracoid process and passed through the clavicular tunnels in a figure-of-eight or V-shaped configuration. Fixation is achieved with interference screws or suspensory cortical buttons. This anatomic approach has demonstrated superior biomechanical strength and stiffness in laboratory studies, closely mirroring the native intact state, and is rapidly becoming the procedure of choice for high-demand athletes.

Arthroscopic and Minimally Invasive Variations
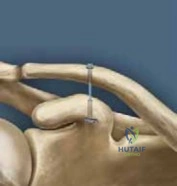
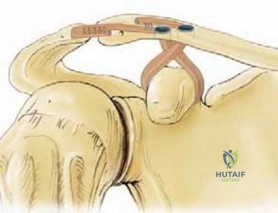
Various arthroscopic and minimally invasive techniques have been developed to minimize soft tissue morbidity. High-strength suture and endobutton devices (e.g., Dog Bone, TightRope) can be deployed arthroscopically to reduce and stabilize the AC joint. A drill hole is created through the clavicle and the base of the coracoid. A heavy suture construct is passed through these tunnels, and cortical buttons are deployed superior to the clavicle and inferior to the coracoid. While highly effective for acute injuries (where the native ligaments can heal), utilizing this technique in chronic cases often requires biological augmentation with a tendon graft, as the synthetic construct alone is prone to eventual fatigue failure or osteolysis through the clavicular bone tunnel.
Complications, Incidence Rates, and Salvage Management
Despite advancements in surgical technique, operations on the AC joint carry a distinct complication profile that the orthopedic surgeon must be prepared to manage. A successful outcome is heavily dependent on meticulous surgical execution, appropriate patient selection, and strict compliance with postoperative rehabilitation. The most frequent complication following isolated distal clavicle resection is persistent pain, which occurs in up to 10-15% of patients. This is most commonly attributed to inadequate bone resection (leading to recurrent bony impingement), aggressive over-resection (leading to iatrogenic instability), or failure to identify and treat concomitant glenohumeral pathology, particularly SLAP lesions and partial articular-sided rotator cuff tears.
When distal clavicle resection is combined with CC ligament reconstruction, the complication profile shifts toward biomechanical and hardware-related issues. Loss of reduction or recurrent deformity is observed in 10% to 20% of cases, particularly when utilizing non-anatomic techniques like the Weaver-Dunn without rigid augmentation. Biological failures, such as graft rupture or failure of graft incorporation, can lead to recurrent instability. Furthermore, rigid synthetic fixation devices (e.g., heavy sutures or synthetic ligaments) can cause osteolysis around the clavicular drill holes, leading to widening of the tunnels and secondary loss of reduction.
Fractures of the clavicle or the coracoid process represent catastrophic biomechanical failures. Coracoid fractures typically occur due to improper drill hole placement (too anterior or eccentric) or thermal necrosis during drilling. Clavicle fractures can propagate through the drill holes if they are placed too close together or if the diameter of the tunnel significantly compromises the cortical integrity of the bone. Heterotopic ossification within the CC ligament space is another common radiographic finding, occurring in up to 30% of operative cases; however, it is usually asymptomatic and rarely requires surgical excision unless it causes severe impingement or neurovascular compromise.
Salvage management for a failed AC joint reconstruction is technically demanding. Revision surgery typically requires a robust anatomic reconstruction using structural allograft, often augmented with temporary rigid fixation (such as a hook plate) to protect the construct during early healing. If a clavicle or coracoid fracture has occurred, rigid open reduction and internal fixation (ORIF) must be performed concurrently. In patients with chronic, refractory pain following multiple failed procedures, addressing scapular dyskinesia through intensive, specialized physical therapy is paramount, as altered scapulothoracic kinematics will continuously place abnormal stress on any surgical repair.
| Complication | Estimated Incidence | Etiology / Risk Factors | Salvage / Management Strategy |
|---|---|---|---|
| Persistent Pain | 10 - 15% | Inadequate resection, missed SLAP lesion, iatrogenic instability | Revision resection, diagnostic arthroscopy, CC reconstruction |
| Loss of Reduction | 10 - 20% | Graft failure, knot slippage, non-compliance with sling | Revision anatomic reconstruction (ACCR) |
Clinical & Radiographic Imaging Archive