Acute Shoulder Dislocation & AC Joint Reconstruction
Key Takeaway
Uncomplicated anterior shoulder dislocations are typically managed nonoperatively; however, young, highly active patients demonstrate significantly lower recurrence rates with early arthroscopic stabilization. Complex dislocations may involve irreducible elements such as biceps tendon interposition or concurrent rotator cuff tears, necessitating open reduction and repair. Acromioclavicular joint separations often require surgical intervention utilizing techniques such as the Weaver-Dunn procedure to restore coracoclavicular stability and shoulder biomechanics.
Comprehensive Introduction and Patho-Epidemiology
The glenohumeral joint, owing to its exceptionally shallow glenoid fossa and profound reliance on dynamic and static soft-tissue restraints, holds the distinction of being the most frequently dislocated major joint in the human body. Accounting for nearly 50% of all major joint dislocations presenting to emergency departments, anterior glenohumeral instability represents a formidable challenge to the orthopedic surgeon. While uncomplicated dislocations of the shoulder rarely require emergent open reduction, the management paradigm for first-time dislocators has evolved significantly over the past two decades. The traditional dogma of universal immobilization has been supplanted by a nuanced, patient-specific algorithm. The decision-making process must meticulously account for patient age, athletic activity level, specific pathoanatomy, and the presence of concurrent injuries to optimize long-term functional outcomes and mitigate the risk of chronic instability.
Although closed reduction under procedural sedation is successful in the vast majority of acute anterior dislocations, a critical subset of these injuries proves irreducible. A shoulder dislocation that cannot be reduced under adequate conscious sedation or general anesthesia should immediately raise the suspicion of soft-tissue interposition or an obstructing osteochondral fragment. Repeated, forceful attempts at closed reduction in these scenarios are strictly contraindicated, as they may result in catastrophic iatrogenic neurovascular injury, particularly to the axillary nerve or artery, or iatrogenic fractures of the proximal humerus. Seradge and Orme, alongside Kuhnen and Groves, have classically described acute anterior dislocations of the shoulder that were irreducible due to the interposition of the long head of the biceps tendon. In these complex cases, the biceps tendon slips posteriorly to the humeral head, creating an unyielding mechanical block to reduction. Furthermore, acute dislocations may be complicated by fracture fragments from the greater tuberosity or the anterior glenoid rim that become incarcerated within the joint space, preventing the humeral head from returning to its concentric position. These complex fracture-dislocations necessitate emergent open reduction and internal fixation (ORIF) to restore articular congruity and inherent stability.
The demographic profile of the patient is a critical determinant of associated pathology and dictates the diagnostic workup. While young patients typically sustain capsulolabral avulsions (classic Bankart lesions) with associated capsular stretching, patients over the age of 40 are at a significantly higher risk for concurrent rotator cuff tears. Neviaser et al. reported on a seminal cohort of 31 patients, the majority of whom were older than 40 years, who sustained massive rotator cuff tears in addition to acute shoulder dislocations. It is a fundamental surgical warning that rotator cuff tears must be highly suspected when profound weakness in abduction or external rotation persists after successful shoulder reduction. Surgeons must not erroneously attribute this weakness solely to axillary nerve neurapraxia without thorough advanced imaging investigation. In the Neviaser cohort, the diagnosis of a massive rotator cuff tear was confirmed via arthrography (though modern practice mandates magnetic resonance imaging). Without intervention, eight of these patients rapidly developed chronic instability. Ultimately, all 31 patients required surgical rotator cuff repair to restore function and stability, highlighting that the loss of the concavity-compression forces provided by the rotator cuff severely destabilizes the glenohumeral joint.
Concurrently, injuries to the superior shoulder girdle frequently involve the acromioclavicular (AC) joint, a distinctly different pathoanatomic entity compared to glenohumeral instability. AC joint separations are typically the result of a direct, high-energy blow to the superior aspect of the acromion with the arm adducted. This mechanism forcibly drives the acromion inferiorly and medially while the clavicle remains stabilized in its anatomic position by the sternocleidomastoid muscle. These injuries are highly prevalent among young athletes engaged in contact sports such as rugby, American football, and ice hockey, as well as in high-velocity trauma scenarios like equestrian or motorcycle accidents. Understanding the precise epidemiology and mechanisms of both glenohumeral and AC joint injuries is the foundational first step in formulating an effective, evidence-based surgical or non-operative treatment plan.
Detailed Surgical Anatomy and Biomechanics
A profound mastery of the surgical anatomy and biomechanics of the shoulder girdle is non-negotiable for the orthopedic surgeon attempting to reconstruct these intricate joints. The glenohumeral joint is a highly mobile diarthrodial joint that sacrifices intrinsic osseous stability for an expansive global range of motion. The humeral head articulates with the glenoid cavity of the scapula, which covers only approximately 25% to 30% of the humeral articular surface at any given time. This inherent osseous mismatch requires a complex interplay of static and dynamic soft-tissue restraints. The static restraints include the glenoid labrum, the articular capsule, and the glenohumeral ligaments. The labrum, a fibrocartilaginous ring, deepens the glenoid socket by up to 50% and serves as the critical attachment site for the capsuloligamentous structures. The inferior glenohumeral ligament (IGHL) complex, consisting of an anterior band, a posterior band, and an interposed axillary pouch, is the primary static restraint against anterior, posterior, and inferior translation of the humeral head when the arm is abducted and externally rotated—the classic position of apprehension and dislocation.
The dynamic stability of the glenohumeral joint is primarily governed by the rotator cuff musculature (supraspinatus, infraspinatus, teres minor, and subscapularis) and the long head of the biceps tendon. These muscles function synergistically to center the humeral head within the glenoid fossa throughout the arc of motion, a biomechanical phenomenon known as concavity compression. When an acute anterior dislocation occurs, the humeral head is forcibly translated anteriorly and inferiorly over the glenoid rim. This catastrophic translation typically results in the avulsion of the anterior-inferior labrum and the attached IGHL complex from the glenoid rim—the quintessential Bankart lesion. Understanding these specific intraarticular lesions is essential for predicting recurrence. Baker et al. identified and classified these lesions into three distinct groups based on examination under anesthesia (EUA) and diagnostic arthroscopy. Group 1 comprises isolated capsular tears without labral detachment; Group 2 involves partial labral detachment with Hill-Sachs lesions (impaction fractures of the posterolateral humeral head); and Group 3 is characterized by gross instability, complete disruption of the IGHL insertion (Bankart lesion), and deep, engaging Hill-Sachs lesions. This classification underscores that the severity of the initial capsulolabral injury directly correlates with the degree of clinical instability.
In stark contrast to the ball-and-socket mechanics of the glenohumeral joint, the acromioclavicular (AC) joint is a diarthrodial joint that links the axial skeleton to the upper extremity appendicular skeleton via the clavicle. Stability of the AC joint is meticulously maintained by two distinct ligamentous complexes. The acromioclavicular (AC) ligaments, which span directly across the joint capsule, primarily provide horizontal (anterior-posterior) stability. The superior AC ligament is the most robust and biomechanically significant of this group. The coracoclavicular (CC) ligaments, consisting of the conoid (medial) and trapezoid (lateral) ligaments, are the primary stabilizers against vertical (superior-inferior) translation. The conoid ligament originates on the posteromedial base of the coracoid and inserts on the conoid tubercle of the clavicle, approximately 4.5 cm medial to the distal clavicular articular surface. The trapezoid ligament originates anterolaterally on the coracoid and inserts on the trapezoid line of the clavicle, roughly 3.0 cm medial to the joint.
During an AC joint separation, the sequence of ligamentous failure predictably follows the magnitude of the applied force. Mild forces result in sprains of the AC ligaments (Rockwood Type I), while moderate forces cause complete disruption of the AC ligaments with spraining of the CC ligaments (Rockwood Type II). High-energy trauma leads to catastrophic failure of both the AC and CC ligament complexes, resulting in gross superior displacement of the distal clavicle relative to the acromion (Rockwood Types III through VI). Furthermore, the deltotrapezial fascia, which envelops the distal clavicle and acromion, is often violently stripped during high-grade injuries. The integrity of this fascial sleeve is a critical, yet often underappreciated, dynamic stabilizer of the AC joint. Surgical reconstruction must not only address the static ligamentous restraints but must also meticulously repair the deltotrapezial fascia to restore the complex biomechanical force couples of the superior shoulder suspensory complex.
Exhaustive Indications and Contraindications
The decision to proceed with operative intervention for acute shoulder dislocations and AC joint separations requires a synthesis of clinical evidence, patient demographics, and precise pathoanatomic diagnosis. The traditional approach of immobilizing all first-time glenohumeral dislocators has been rigorously challenged by prospective data demonstrating unacceptably high recurrence rates in young, active populations. We currently favor initial nonoperative management for first-time dislocations in older or sedentary patients, provided there is no evidence of a massive rotator cuff tear or incarcerated intraarticular fragment. However, arthroscopic stabilization procedures are now considered an appropriate, and often superior, alternative in selected young athletes. High-level studies have demonstrated that active patients under the age of 25 engaged in contact or overhead sports possess a statistical probability of recurrent dislocation exceeding 80% if treated nonoperatively. Therefore, early arthroscopic Bankart repair is strongly indicated in this demographic to prevent the devastating cumulative articular cartilage damage and progressive bone loss associated with recurrent instability episodes.
For AC joint separations, the indications for surgery are dictated by the Rockwood classification system. Rockwood Types I and II injuries represent stable or minimally displaced injuries and are universally managed nonoperatively with a brief period of sling immobilization followed by aggressive physical therapy. The management of Type III injuries remains one of the most controversial topics in orthopedic surgery. While the general population often tolerates a Type III separation well with nonoperative care, surgical reconstruction is frequently indicated for overhead athletes, manual laborers, and individuals who exhibit profound scapular dyskinesia or intolerable cosmetic deformity. Conversely, Rockwood Types IV (posterior displacement into the trapezius), V (severe superior displacement >100% with extensive fascial stripping), and VI (inferior subcoracoid displacement) are absolute indications for surgical reconstruction due to the severe displacement, fascial disruption, and predictable functional morbidity if left unreduced.
Absolute contraindications to surgical intervention in both glenohumeral and AC joint pathology include active local or systemic infection, severe medical comorbidities precluding safe anesthesia, and profound patient non-compliance or psychiatric conditions that would prevent adherence to the rigorous postoperative rehabilitation protocols. Relative contraindications include advanced physiologic age with low functional demands, chronic asymptomatic subluxations, and voluntary, multidirectional instability driven by underlying connective tissue disorders (e.g., Ehlers-Danlos syndrome), which typically respond better to prolonged, specialized physical therapy regimens.
| Pathology / Injury Type | Indications for Operative Intervention | Indications for Nonoperative Management | Absolute Contraindications to Surgery |
|---|---|---|---|
| First-Time Anterior GH Dislocation | Age < 25, contact athletes, irreducible dislocation, incarcerated fragment, concomitant massive rotator cuff tear (age > 40). | Age > 30, sedentary lifestyle, isolated capsulolabral injury without significant bone loss, compliant patient. | Active joint infection, severe medical comorbidities, voluntary/habitual dislocators. |
| Recurrent Anterior GH Instability | Multiple instability episodes, progressive glenoid bone loss, failed conservative therapy, engaging Hill-Sachs lesion. | Low-demand patient willing to modify activities, connective tissue disorders (relative). | Inability to comply with postoperative immobilization, active infection. |
| AC Joint Separation (Rockwood I-II) | Extremely rare; considered only if chronic, debilitating pain persists > 6 months post-injury. | Universal first-line treatment. Sling for comfort, early ROM, strengthening. | Standard surgical contraindications apply. |
| AC Joint Separation (Rockwood III) | Overhead athletes, heavy manual laborers, severe scapular dyskinesia, unacceptable cosmetic deformity to the patient. | General population, non-dominant arm, sedentary individuals. | Active infection, non-compliance, lack of soft-tissue coverage. |
| AC Joint Separation (Rockwood IV-VI) | Universal indication. Severe displacement requires reduction and CC ligament reconstruction. | Medically unfit for surgery, polytrauma patient in extremis (delay until stable). | Active local infection, severe overlying soft-tissue compromise/burns. |
Pre-Operative Planning, Templating, and Patient Positioning
Meticulous pre-operative planning is the cornerstone of successful shoulder reconstruction. For acute glenohumeral dislocations, the clinical evaluation must include a comprehensive neurovascular examination, with particular attention paid to the axillary nerve (assessing sensation over the lateral deltoid) and the musculocutaneous nerve. Standard radiographic evaluation must include a true anteroposterior (Grashey) view, a scapular Y view, and an axillary lateral view to confirm concentric reduction and evaluate for osseous Bankart lesions or large Hill-Sachs defects. Advanced imaging is critical; Magnetic Resonance Imaging (MRI) or MR Arthrography (MRA) is the gold standard for delineating the extent of capsulolabral injury, assessing the integrity of the rotator cuff, and identifying subtle chondral damage. If plain radiographs suggest significant glenoid bone loss, a non-contrast Computed Tomography (CT) scan with 3D reconstruction and digital subtraction of the humeral head is mandatory to quantify the percentage of glenoid deficiency. Critical bone loss exceeding 15% to 20% of the anterior glenoid width typically precludes an isolated soft-tissue Bankart repair and necessitates a bone-grafting procedure, such as the Latarjet coracoid transfer.
For AC joint separations, bilateral Zanca views (AP view with a 10- to 15-degree cephalic tilt) are essential for accurately assessing the degree of superior-inferior displacement compared to the contralateral, uninjured shoulder. Axillary lateral views are required to rule out posterior displacement of the clavicle into the trapezius musculature (Type IV injury). Historically, weighted stress views were utilized to differentiate between Type II and Type III injuries; however, these are now largely considered obsolete due to patient discomfort and lack of clinical utility in altering the modern surgical algorithm. MRI may be utilized in chronic cases to assess the quality of the distal clavicle and rule out concomitant intraarticular glenohumeral pathology, which is present in up to 15% of high-grade AC joint separations.
Patient positioning is a critical intraoperative variable that dictates surgical access and ease of fluoroscopic imaging. For arthroscopic glenohumeral stabilization, surgeons may choose between the lateral decubitus and the beach chair positions. The lateral decubitus position, utilizing longitudinal and lateral traction, affords excellent visualization of the inferior glenohumeral recess and facilitates the placement of inferior suture anchors. Conversely, the beach chair position offers the advantage of an upright anatomic orientation, easier conversion to an open procedure if necessary, and unhindered access to the anterior, superior, and posterior aspects of the shoulder. For AC joint reconstructions, the beach chair position is universally preferred. The patient is positioned with the head secured in a specialized headrest, and the operative arm is draped free to allow for dynamic assessment of reduction. A thorough interscalene regional nerve block, administered preoperatively by the anesthesia team, is highly recommended to minimize intraoperative volatile anesthetic requirements and provide profound postoperative analgesia. The C-arm fluoroscope must be positioned either parallel to the patient or coming in from the contralateral side, ensuring unobstructed orthogonal views of the AC joint and coracoid process.
Step-by-Step Surgical Approach and Fixation Technique
Arthroscopic Bankart Repair for Acute Dislocation
The surgical management of acute anterior instability in the young athlete is most commonly addressed via an arthroscopic Bankart repair. Following the establishment of standard posterior, anteroinferior, and anterosuperior portals, a thorough diagnostic arthroscopy is performed. The hallmark of the procedure is the aggressive mobilization of the torn capsulolabral complex. Using an arthroscopic elevator or raspatory, the labrum and the attached IGHL must be completely freed from the anterior glenoid neck down to the 6 o'clock position, allowing the tissue to float freely. The anterior glenoid rim is then decorticated using a motorized burr to create a bleeding bone bed, which is essential for biological healing.
Fixation is achieved using modern suture anchors, either knotted or knotless, typically composed of biocomposite materials or all-suture constructs. The first anchor is placed at the lowest possible point of the detachment, usually at the 5:30 or 6 o'clock position on the right shoulder, to ensure adequate superior shift of the inferior capsule. A suture passing device (e.g., a spectrum or suture lasso) is used to capture a robust bite of the inferior capsule and the labrum, taking care to incorporate the IGHL. The suture is then tied or tensioned, effectively shifting the capsulolabral complex superiorly and laterally, restoring the anatomic "bumper" effect and re-tensioning the inferior sling. This process is repeated sequentially superiorly, typically requiring three to four anchors, until the entire anterior labrum is securely fixed and the concavity of the glenoid is restored.
The Stewart Technique for Acute AC Dislocation
Historically, acute AC joint dislocations were managed with direct transarticular fixation to hold the joint reduced while the native ligaments healed. The Stewart technique is a classic example of this approach, utilizing rigid pin fixation across the acromioclavicular articulation.
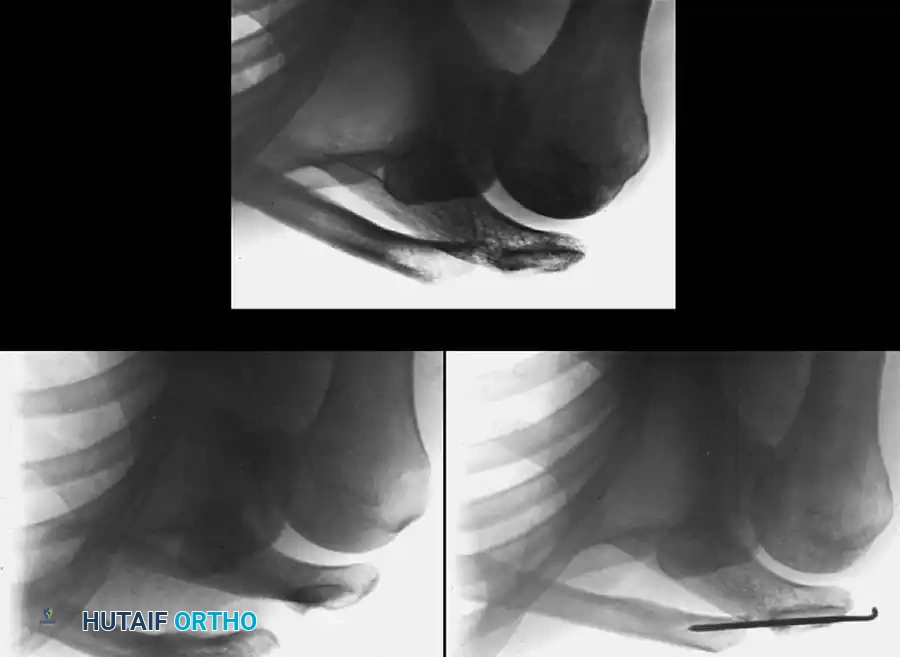
Fig. 57-19 Stewart technique for acute dislocation of acromioclavicular joint. A, Soon after injury. B, Six weeks after surgery. C, Three months after surgery.
The patient is placed in the beach chair position, and a superior approach is made directly over the distal clavicle and AC joint. The AC joint is meticulously debrided of any interposed meniscal remnants or frayed ligamentous tissue that might block anatomic reduction. The clavicle is then reduced anatomically in both the horizontal and vertical planes, often requiring downward pressure on the clavicle and upward pressure on the elbow. Once reduced, heavy Kirschner wires or Steinmann pins are driven from the lateral aspect of the acromion, across the AC joint, and deeply into the medullary canal of the distal clavicle. While biomechanically rigid, this transarticular AC joint pinning carries a well-documented and potentially catastrophic risk of pin migration. If pins migrate medially, they can penetrate the thoracic cavity, causing pneumothorax, or injure vital neurovascular structures. Consequently, the pins must be removed at 6 weeks (as seen in Fig. 57-19 B) to prevent hardware fatigue and breakage, allowing for subsequent fibrous healing of the joint (Fig. 57-19 C). Due to these risks, modern techniques heavily favor CC ligament reconstruction over isolated transarticular AC pinning.
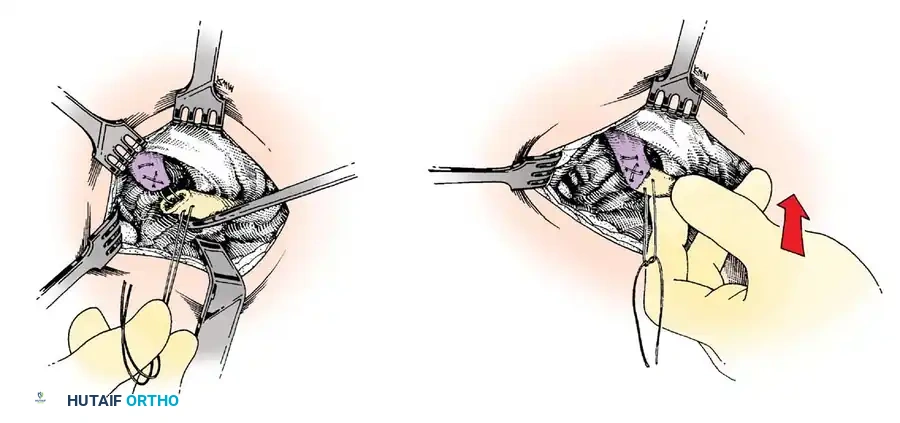
The Weaver-Dunn Procedure for AC Joint Reconstruction
For chronic AC joint separations, or severe acute separations (Types IV-VI) where primary repair of the CC ligaments is insufficient due to poor tissue quality, the Weaver-Dunn procedure remains a foundational technique. Originally described in 1972, this procedure reconstructs the CC ligament complex by transferring the native coracoacromial (CA) ligament.
Fig. 57-20 Technique of Weaver and Dunn for acromioclavicular separations (see text). (Redrawn from Weaver JK, Dunn HK: Treatment of acromioclavicular injuries, especially complete acromioclavicular separation, J Bone Joint Surg 54A:1187, 1972.)
Through a saber incision extending from the posterior clavicle to the coracoid process, the distal 1 to 1.5 cm of the clavicle is excised. This critical step prevents future AC joint arthrosis and creates the necessary space for reduction. The coracoacromial (CA) ligament is identified and detached from its insertion on the undersurface of the acromion, often harvested with a small fleck of bone to enhance osteoligamentous healing. The ligament is mobilized while its origin on the coracoid process is left meticulously intact. Heavy non-absorbable sutures (e.g., #2 FiberWire) are woven into the free end of the CA ligament using a Krackow or whipstitch technique. The clavicle is reduced inferiorly, and the free end of the CA ligament is transferred into the medullary canal of the distal clavicle and secured via the pre-placed sutures through superior drill holes.
Because the native CA ligament possesses only about 25% of the tensile strength of the native CC ligaments, the classic Weaver-Dunn procedure is almost universally augmented in modern surgical practice. This augmentation is typically achieved using heavy suture cerclage, cortical suspension buttons, or suture anchors passed around or through the base of the coracoid and the clavicle. This synthetic augmentation acts as an internal brace, protecting the CA ligament transfer from vertical loads while it undergoes biological incorporation. Finally, the deltotrapezial fascia is meticulously imbricated and repaired over the distal clavicle, providing essential dynamic stability to the construct.
Complications, Incidence Rates, and Salvage Management
Surgical intervention for both glenohumeral instability and AC joint separations carries inherent risks, and a thorough understanding of potential complications is vital for optimal patient counseling and postoperative management. Following arthroscopic Bankart repair, the most significant complication is recurrent instability. While modern techniques have reduced recurrence rates to approximately 5% to 10% in appropriately selected patients, failures still occur, most commonly due to unrecognized glenoid bone loss, inadequate capsular plication, or premature return to contact sports. Postoperative stiffness, particularly a loss of terminal external rotation, is another frequent complication, affecting up to 15% of patients. This is often the result of over-tensioning the anterior capsule or prolonged postoperative immobilization. Neurologic injury is rare but can occur; the axillary nerve is at highest risk during the placement of anteroinferior portals or during deep capsular dissection at the 6 o'clock position.
In the realm of AC joint reconstruction, complications are historically more prevalent, reflecting the immense biomechanical forces exerted on this small articulation. Following a Weaver-Dunn procedure or modern CC ligament reconstruction, loss of reduction is the most common complication, with radiographic recurrence of superior clavicular displacement reported in 10% to 30% of cases. This is often due to hardware failure, such as cortical button pull-through through the clavicle, suture breakage, or biological failure of the ligament transfer. Coracoid fractures are a devastating complication associated with techniques that require drilling large tunnels through the coracoid process. Distal clavicle osteolysis can also occur, presenting as insidious shoulder pain months after the initial surgery. The dreaded complication of pin migration, historically associated with the Stewart technique, requires emergent intervention if the hardware migrates toward the mediastinum.
Salvage management for these complications requires advanced reconstructive techniques. A failed arthroscopic Bankart repair, particularly in the setting of progressive bone loss, is typically salvaged with an open Latarjet procedure, which transfers the coracoid process and the attached conjoint tendon to the anterior glenoid rim, providing a robust osseous and dynamic sling effect. For a failed AC joint reconstruction with recurrent instability, revision surgery often involves an anatomic CC ligament reconstruction utilizing a robust free tendon allograft (e.g., semitendinosus or tibialis anterior) looped under the coracoid and secured through the clavicle, augmented with rigid cortical button fixation.
| Complication | Estimated Incidence | Prevention Strategy | Salvage Treatment / Management |
|---|---|---|---|
| Recurrent GH Instability | 5% - 15% | Accurate assessment of bone loss pre-op; adequate capsular shift; strict adherence to rehab. | Revision stabilization; Latarjet procedure if significant anterior glenoid bone loss is present. |
| Post-op Shoulder Stiffness | 10% - 20% | Avoid over-tensioning the capsule; initiate early, controlled passive ROM in Phase II. | Aggressive physical therapy; arthroscopic capsular release if refractory > 6-9 months. |
| Loss of AC Joint Reduction | 10% - 30% | Augment CA ligament transfers with rigid cortical buttons or heavy suture cerclage. | Revision AC reconstruction using free tendon allograft (anatomic CC reconstruction). |
| Coracoid Fracture (AC Repair) | 1% - 3% | Avoid drilling oversized holes in the coracoid; use sub-coracoid looping techniques when possible. | Open reduction internal fixation of coracoid; conversion to conservative management if stable. |
| Hardware Migration (Pins) | Variable (High with smooth pins) | Use threaded pins if transarticular fixation is chosen; remove pins strictly at 6 weeks. | Emergent removal; thoracic surgery consultation if medial migration into chest cavity occurs. |
Phased Post-Operative Rehabilitation Protocols
Whether the patient is undergoing an arthroscopic Bankart repair for acute glenohumeral instability or a complex Weaver-Dunn reconstruction for a high-grade AC separation, strict adherence to a meticulously phased rehabilitation protocol is mandatory. The success of these procedures is as dependent on the biological healing of the soft tissues as it is on the mechanical strength of the initial surgical fixation. The rehabilitation timeline must respect the physiological phases of tissue healing: inflammation, proliferation, and remodeling.
Phase I: Maximum Protection (0-4 Weeks)
The primary goal of Phase I is to protect the surgical repair while minimizing the deleterious effects of absolute immobilization. For glenohumeral stabilization, the patient is placed in a standard abduction sling. For AC joint reconstructions, a specialized sling that supports the elbow to push the humerus and scapula upward—thereby relieving gravitational tension on the newly reconstructed CC ligaments—is utilized. During this phase, absolute immobilization is the rule, with the exception of controlled pendulum exercises. Active elevation, cross-body adduction, and any lifting are strictly prohibited. Cryotherapy is utilized aggressively to manage postoperative edema and pain. Hand, wrist, and elbow active range of motion (AROM) are encouraged to prevent distal stiffness.
Phase II: Moderate Protection and Early Motion (4-8 Weeks)
At the 4-week mark, the sling is typically discontinued during the day, though patients may continue to wear it in crowded environments or while sleeping for protection. Passive range of motion (PROM) and active-assisted range of motion (AAROM) are formally initiated under the guidance of a physical therapist. For anterior glenohumeral stabilization, it is critical to protect the anterior caps
