Chronic AC Joint Dislocation: Coracoacromial Ligament Reconstruction
Key Takeaway
Chronic acromioclavicular (AC) joint dislocations often require surgical reconstruction when conservative management fails. The modified Weaver-Dunn procedure utilizes the coracoacromial (CA) ligament transferred into the distal clavicle to restore stability. By incorporating a bone block from the acromion, surgeons achieve superior bone-to-bone healing. Temporary coracoclavicular fixation with a Bosworth lag screw protects the reconstruction during the critical 12-week healing phase, ensuring optimal biomechanical restoration and functional recovery.
Comprehensive Introduction and Patho-Epidemiology
The management of chronic, unreduced acromioclavicular (AC) joint dislocations—specifically Rockwood Types III, IV, V, and VI—remains a complex and highly debated challenge in operative orthopaedics. While acute injuries are often amenable to primary repair or conservative management depending on the grade, chronic dislocations present a distinctly different pathophysiological entity. In these chronic settings, typically defined in the orthopaedic literature as injuries older than three to four weeks, primary repair of the coracoclavicular (CC) ligaments is no longer biologically or mechanically viable. The native ligamentous tissue undergoes rapid and irreversible retraction, scarring, and structural degeneration, rendering it entirely unsuitable for direct approximation. Consequently, the orthopaedic surgeon is mandated to employ anatomical or non-anatomical ligamentous reconstruction to restore the intricate biomechanics of the shoulder girdle.
When conservative management of high-grade AC joint dislocations fails, patients frequently present to the clinic with a constellation of debilitating symptoms. Chief among these are chronic, deep-seated anterior shoulder pain, pronounced shoulder fatigue during overhead activities, and a visually prominent, often ballotable distal clavicle. Furthermore, the loss of the suspensory mechanism of the shoulder girdle inevitably leads to scapular dyskinesia. The scapula, deprived of its superior strut, protracts, anteriorly tilts, and inferiorly translates—a kinematic disruption often referred to as SICK scapula syndrome (Scapular malposition, Inferior medial border prominence, Coracoid pain and malposition, and DysKinesis of scapular movement). This secondary scapulothoracic dysfunction places immense abnormal strain on the periscapular musculature and the rotator cuff, often exacerbating the patient's functional impairment and pain profile.
The historical evolution of chronic AC joint reconstruction is anchored by the classic Weaver-Dunn procedure, first described in 1972. This landmark technique revolutionized the treatment of chronic AC joint instability by transferring the coracoacromial (CA) ligament from its acromial insertion to the distal clavicle, effectively substituting the robust CA ligament for the ruptured, incompetent CC ligaments. However, long-term clinical and biomechanical follow-up of the original Weaver-Dunn technique revealed significant shortcomings. The original procedure relied entirely on soft-tissue-to-bone healing, requiring the detached CA ligament to integrate into the medullary canal of the clavicle. Biomechanical studies conclusively demonstrated that this ligament-to-bone interface was the weakest link in the reconstructive construct, frequently leading to graft elongation (creep), loss of reduction, and ultimate clinical failure.
To address these inherent biomechanical deficiencies, modern operative orthopaedics employs critical, evidence-based modifications to the traditional technique. The advanced reconstructive strategy detailed in this chapter incorporates the Copeland and Kessel modification, which utilizes a vascularized acromial bone block to facilitate superior, rapid bone-to-bone healing within the clavicle. Furthermore, it integrates the Rockwood and Cadenat modification to safely lengthen the CA ligament, ensuring tension-free docking. These biological enhancements are strictly augmented by rigid, temporary coracoclavicular fixation using a lag screw, which functions as an internal splint to completely offload the healing graft during the critical initial phases of biological incorporation.
Detailed Surgical Anatomy and Biomechanics
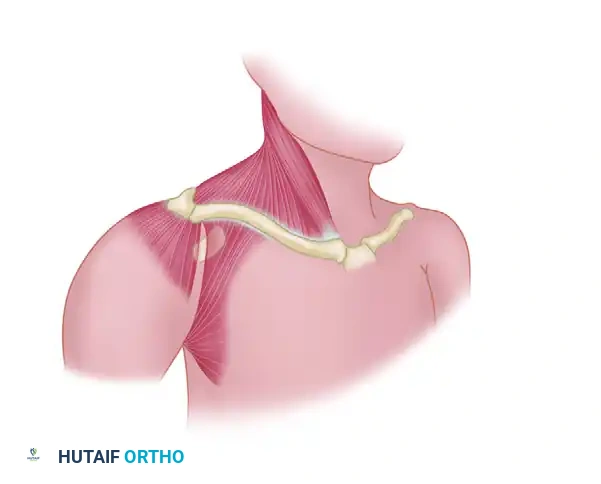
A profound, three-dimensional understanding of the dynamic and static stabilizers of the acromioclavicular joint is an absolute prerequisite for successful surgical reconstruction. The AC joint is a diarthrodial joint characterized by an intra-articular fibrocartilaginous disc and a complex capsuloligamentous network. The distal clavicle articulates with the medial facet of the acromion, and the joint's stability is governed by a synergistic interplay between the AC ligaments, the CC ligaments, and the dynamic muscular envelope provided by the deltotrapezial fascia.
The Acromioclavicular (AC) ligaments are divided into superior, inferior, anterior, and posterior fascicles. Biomechanical sectioning studies have definitively shown that these ligaments primarily control horizontal (anteroposterior) translation of the distal clavicle. The superior AC ligament is by far the most robust of the four, largely due to its intimate confluence with the aponeurotic fibers of the deltoid and trapezius muscles. During reconstruction, the meticulous preservation and subsequent imbrication of this deltotrapezial fascial sleeve are paramount, as it provides vital dynamic compression across the AC joint and serves as a secondary restraint against superior clavicular migration.
The Coracoclavicular (CC) ligaments comprise the conoid and trapezoid ligaments, which function as the primary static restraints to superior vertical translation of the clavicle relative to the scapula. The conoid ligament is positioned posteromedially; it is cone-shaped and primarily resists anterior and superior displacement of the clavicle. The trapezoid ligament is located anterolaterally; it is broader, flatter, and primarily resists axial compression, preventing the acromion from being driven medially beneath the clavicle. Together, the CC ligaments form a highly specialized suspensory complex that dictates the synchronous rotation of the clavicle during scapulothoracic motion. During full shoulder elevation, the clavicle must rotate posteriorly up to 40 to 50 degrees; any reconstructive technique that permanently locks the clavicle to the coracoid will inherently abolish this rotation, leading to restricted shoulder mechanics and inevitable hardware failure.
The Coracoacromial (CA) ligament is a strong, triangular fascial band extending from the lateral border of the coracoid process to the anteroinferior surface of the acromion. While its primary native physiological function is to serve as the structural roof of the subacromial space—preventing superior migration of the humeral head—its robust tensile strength and favorable anatomical proximity make it an ideal autograft for CC ligament reconstruction. The CA ligament is composed of two distinct functional bands: a thicker anterolateral band and a thinner posteromedial band.
Clinical Pearl: Harvesting the CA ligament removes the primary static restraint against superior humeral head escape. Therefore, this reconstructive procedure is strictly contraindicated in patients with massive, irreparable rotator cuff tears. In such patients, the loss of the CA ligament will precipitate rapid, uninhibited superior migration of the humeral head, drastically accelerating the onset of debilitating cuff tear arthropathy.
Exhaustive Indications and Contraindications
Patient selection is the cornerstone of achieving excellent outcomes in chronic AC joint reconstruction. The decision to proceed with operative intervention must be based on a comprehensive assessment of the patient's chronicity of injury, functional demands, degree of displacement, and the presence of secondary scapular dyskinesia. The modified Weaver-Dunn procedure with bone block augmentation remains a highly reliable, cost-effective, and biomechanically sound option, particularly in revision scenarios, delayed presentations, or resource-limited settings where expensive allografts or synthetic suspensory devices are unavailable.
Surgical intervention is generally reserved for patients who have failed a dedicated trial of conservative management, which should include physical therapy focused on periscapular strengthening and postural re-education. Patients with Rockwood Type III dislocations present a unique clinical dilemma; while many function well non-operatively, overhead athletes, manual laborers, and those with profound scapular dyskinesia often require reconstruction. Conversely, Rockwood Types IV, V, and VI are characterized by severe soft tissue disruption, fascial stripping, and gross instability, rendering them almost universally symptomatic and necessitating surgical reconstruction in the chronic setting.
| Category | Specific Clinical Parameters | Rationale / Clinical Context |
|---|---|---|
| Primary Indications | Chronic Rockwood Type IV, V, VI dislocations (>4 weeks old). | Gross vertical and horizontal instability with severe deltotrapezial fascial stripping; zero potential for spontaneous ligamentous healing. |
| Relative Indications | Chronic Rockwood Type III dislocations in high-demand patients. | Overhead athletes, heavy manual laborers, or patients with intractable pain and SICK scapula syndrome failing 3-6 months of targeted physical therapy. |
| Revision Indications | Failed primary acute AC joint repairs (e.g., failed hook plate, failed suture button). | The native CC ligaments are incompetent and scarred; an autograft (CA ligament) or allograft reconstruction is mandatory to restore the suspensory mechanism. |
| Absolute Contraindications | Massive, irreparable rotator cuff tears. | The CA ligament is the only remaining restraint to superior humeral head migration. Its harvest will induce rapid, catastrophic cuff tear arthropathy. |
| Absolute Contraindications | Active local or systemic infection. | High risk of deep joint infection, hardware seeding, and catastrophic failure of the bone block incorporation. |
| Relative Contraindications | Severe medical comorbidities, poor soft tissue envelope, or non-compliant patients. | The procedure requires strict adherence to a phased postoperative rehabilitation protocol and a mandatory secondary surgery for screw removal. |
Pre-Operative Planning, Templating, and Patient Positioning
Imaging Requirements and Templating
Standard radiographic evaluation is the foundation of preoperative planning and must include a meticulously obtained trauma series of the shoulder. The standard anteroposterior (AP) view of the shoulder is often insufficient for evaluating the AC joint due to overlapping osseous structures. Therefore, a dedicated Zanca view is mandatory; this is obtained by tilting the X-ray beam 10 to 15 degrees cephalad and using only 50% of the standard penetrance to prevent overexposing the relatively thin distal clavicle. The Zanca view allows for accurate measurement of the CC distance, which is compared to the contralateral normal shoulder.
An axillary lateral view is equally critical to rule out posterior displacement of the distal clavicle into the trapezius muscle, which is the hallmark of a Type IV dislocation. While bilateral stress radiographs (holding weights) were historically utilized to assess the degree of dynamic instability, their routine use has largely been abandoned. Modern high-resolution Magnetic Resonance Imaging (MRI) has supplanted stress radiography, as it provides definitive, non-invasive evaluation of the integrity of the CC ligaments, the AC joint articular disc, and the surrounding deltotrapezial aponeurosis. Furthermore, MRI is invaluable for identifying concomitant intra-articular glenohumeral pathology, such as SLAP lesions or partial rotator cuff tears, which may be present in up to 15-20% of high-grade AC joint injuries.
Positioning and Anesthesia
- Anesthesia: A synergistic combination of general endotracheal anesthesia and a regional ultrasound-guided interscalene nerve block is highly recommended. The interscalene block provides profound intraoperative muscle relaxation, which is critical for manually reducing the chronically elevated clavicle, and offers exceptional postoperative analgesia, thereby minimizing opioid consumption.
- Patient Positioning: The patient is placed in the beach-chair position, with the torso elevated to approximately 45 to 60 degrees. The head must be meticulously secured in a neutral position using a specialized headrest to prevent cervical hyperextension or lateral flexion, thereby protecting the brachial plexus.
- Surgical Preparation: The operative arm must be draped completely free to allow for unencumbered manipulation and full range of motion testing intraoperatively. A rolled towel or a specialized scapular bump is placed under the medial border of the ipsilateral scapula. This maneuver protracts the shoulder girdle, opening the anterior working space and significantly facilitating access to the posterior aspect of the AC joint and the base of the coracoid process.
Step-by-Step Surgical Approach and Fixation Technique
1. Surgical Approach and Exposure
The surgical approach must be meticulously planned to ensure adequate exposure while preserving the integrity of the deltotrapezial fascia. A saber-cut incision or a transverse incision following the Langer lines over the distal clavicle is typically utilized. The incision begins approximately 2 cm medial to the AC joint, centered over the clavicle, and extends laterally and anteriorly toward the palpable tip of the coracoid process.
Upon incising the skin and subcutaneous tissues, hemostasis is achieved. The critical step in the exposure is the management of the deltotrapezial fascia. Meticulous, sharp dissection is required to elevate this fascia as a continuous, robust, full-thickness sleeve. The anterior deltoid is subperiosteally elevated off the anterior aspect of the distal clavicle and the anterior acromion. This subperiosteal elevation is crucial because it preserves the tissue necessary for a secure, imbricated "pants-over-vest" closure at the conclusion of the procedure.
Once the fascial flaps are mobilized, the AC joint is fully exposed. In chronic cases, the joint is often filled with dense, unyielding fibrotic scar tissue. Thorough joint debridement is performed, and the degenerative intra-articular meniscus (articular disc) is completely excised. The distal clavicle is then circumferentially mobilized by releasing any remaining scarred AC capsule, taking care to protect the underlying neurovascular structures.
2. Distal Clavicle Excision and Coracoacromial Ligament Harvest
To prevent postoperative AC joint arthrosis and to create the necessary spatial clearance for the ligament transfer, a distal clavicle excision is performed. Approximately 10 to 15 mm of the distal clavicle is resected using a micro-oscillating saw. The osteotomy cut must be perfectly perpendicular to the long axis of the clavicle to ensure an even distribution of forces and to prevent asymmetric impingement against the acromion during shoulder abduction.
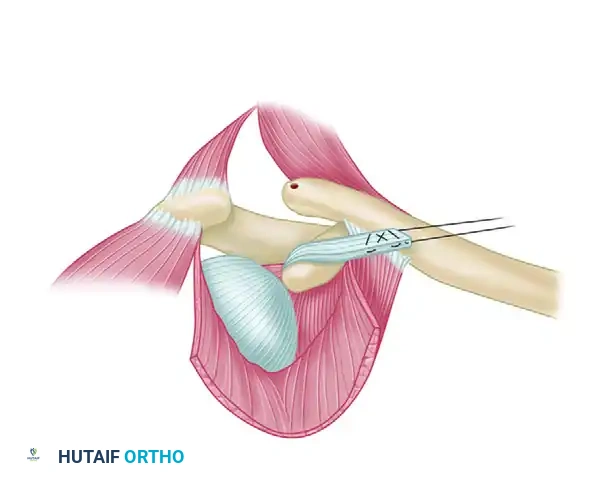
Following the clavicular resection, attention is turned to the harvest of the CA ligament. Instead of sharply detaching the ligament from the acromion—a maneuver that relies on inferior soft-tissue-to-bone healing—the Copeland and Kessel modification is strictly employed.
Using a sharp, narrow 1/4-inch osteotome or a specialized rongeur, the surgeon carefully removes a sliver of bone from the anteroinferior undersurface of the acromion, ensuring it remains in absolute continuity with the CA ligament insertion. This harvested bone block typically measures 10 mm by 15 mm. The biomechanical advantage of this bone block cannot be overstated: it allows for rigid, bone-to-bone fixation within the medullary canal of the distal clavicle, significantly accelerating biological incorporation and dramatically increasing the ultimate pull-out strength of the reconstructive construct.
Surgical Warning: The dimensions of the bone block are critical. If the block is harvested too large, it will not fit into the relatively narrow medullary canal of the distal clavicle, necessitating intraoperative trimming that risks detaching the ligament. Conversely, if the bone block is too thin, it creates a severe stress riser and risks catastrophic fracturing during suture passage and subsequent tensioning.
3. Ligament Mobilization and Suture Preparation
Once the CA ligament is successfully harvested with its attached acromial bone block, its functional length and excursion must be carefully assessed. In many chronic cases, the ligament may be insufficient in length to reach the distal clavicle without excessive, detrimental tension. In such instances, the Rockwood and Cadenat modification is utilized to gain crucial length.
This lengthening technique involves carefully identifying and detaching the anterior fasciculus of the CA ligament from its origin on the waist of the coracoid process. This precise anatomical maneuver safely provides several additional millimeters of excursion without compromising the structural integrity or the tensile strength of the primary ligamentous band.
With the ligament mobilized, preparation for docking begins. A heavy, nonabsorbable braided suture (such as #2 or #5 FiberWire, or Ethibond) is passed back and forth through the substance of the ligament and the bone block. A Krackow or locking whipstitch technique is highly recommended to ensure a secure, non-sliding grip on the tissue. The surgeon must ensure that the two free ends of the heavy suture exit precisely through the acromial bone block end of the construct, as these will be used to draw the block into the clavicle.
4. Preparation of the Clavicle and Coracoid
The medullary canal of the freshly resected distal clavicle must be meticulously prepared to receive the bone block. Using a sharp curette or a small, high-speed spherical burr, the surgeon hollows out the cancellous bone of the distal clavicle, creating a cylindrical socket approximately 15 to 20 mm deep. The cortical walls must be preserved to maintain the structural integrity of the clavicle. Following socket creation, two small drill holes (typically 2.0 mm in diameter) are placed into the superior cortex of the distal end of the clavicle, positioned approximately 1 cm medial to the resected edge. These holes must communicate directly with the newly created medullary socket.
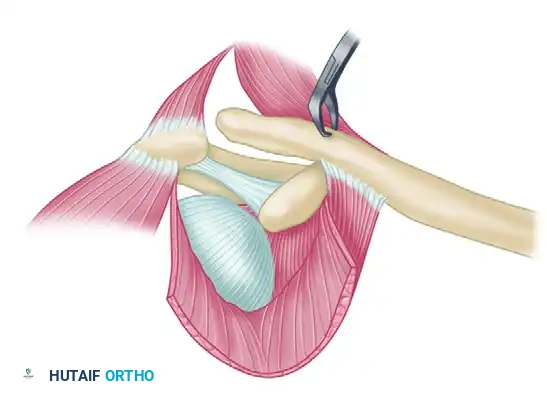
Next, the operative field is prepared for the temporary, rigid coracoclavicular fixation. A drill hole is planned through the distal clavicle, positioned directly superior to the base of the coracoid process.
The clavicle is then manually reduced to its exact anatomical position relative to the coracoid. This often requires substantial downward pressure applied to the distal clavicle while a surgical assistant simultaneously elevates the arm and applies an upward force to the elbow, lifting the scapula and coracoid into a reduced posture. With the clavicle held rigidly in this anatomically corrected position, a drill bit (sized according to the chosen screw) is inserted through the clavicular hole and directed inferiorly. The drill must pass directly through both the superior and inferior cortices of the base of the coracoid process.
Pitfall: The trajectory of the coracoid drill hole is notoriously unforgiving. Drilling the coracoid too anteriorly or medially can lead to catastrophic cortical blowout, rendering screw fixation impossible, or worse, causing devastating iatrogenic neurovascular injury to the underlying brachial plexus or axillary vessels. The drill must be aimed precisely at the central, thickest base of the coracoid process.
5. Coracoclavicular Fixation and Ligament Docking
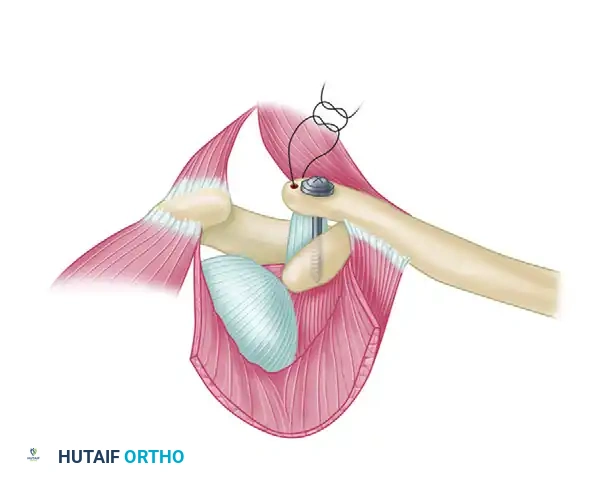
With the osseous tunnels meticulously prepared, the structural reconstruction is finalized. The two free ends of the heavy, nonabsorbable suture (which are attached to the CA ligament and bone block) are passed into the medullary canal of the clavicle and routed out through the two small 2.0 mm holes drilled in the superior cortex. These sutures are clamped but not yet tied.
The temporary internal splint is now placed. A lag screw—traditionally a specialized Bosworth screw, though modern equivalents such as a 4.5 mm fully threaded cortical screw equipped with a spiked washer are frequently utilized—is passed through the clavicle and driven into the prepared coracoid tunnel. The screw is carefully tightened to secure the clavicle in its anatomically reduced position just above the coracoid. This rigid screw acts as an uncompromising internal splint, completely offloading the CA ligament transfer during the critical 12-week biological healing phase.
With the clavicle now rigidly fixed to the coracoid, the ligament docking is completed. The surgeon applies firm, steady tension to the suture ends exiting the superior clavicle, drawing the CA ligament and its attached acromial bone block deep into the prepared medullary socket. Once the bone block is fully seated within the cancellous bed, the two ends of the suture are securely tied over the superior bony bridge of the clavicle, utilizing multiple alternating half-hitches to ensure knot security.
6. Closure and Soft Tissue Imbrication
Meticulous, layered closure is absolutely critical to prevent hardware prominence, minimize dead space, and reduce the risk of postoperative infection. The previously preserved deltotrapezial fascia must be carefully imbricated and repaired securely over the distal clavicle and the reconstruction site. A "pants-over-vest" technique using heavy, slowly absorbable sutures (e.g., #1 PDS or Vicryl) provides a robust dynamic stabilizer that reinforces the superior aspect of the AC joint. The subcutaneous tissue is closed in a standard layered fashion, followed by meticulous skin closure using a subcuticular stitch or surgical staples, depending on the surgeon's preference and the patient's soft tissue envelope.
Complications, Incidence Rates, and Salvage Management
Despite meticulous preoperative planning and flawless surgical execution, the reconstruction of chronic AC joint dislocations carries a distinct complication profile. The procedure relies heavily on biological healing and patient compliance, making it susceptible to both mechanical and biological failures.
| Complication | Estimated Incidence | Etiology / Pathomechanism | Salvage Management & Prevention |
|---|---|---|---|
| Hardware Failure (Screw Breakage) | 5% - 15% | Occurs if the patient is non-compliant with postoperative lifting restrictions, or critically, if the coracoclavicular screw is left in place beyond the mandatory 12 to 14-week removal window. The normal rotation of the clavicle will inevitably fatigue and snap the rigid screw. | Prevention: Strict adherence to the 12-week screw removal protocol. Salvage: If broken, the retained coracoid fragment is often left in situ if asymptomatic. Symptomatic fragments require technically demanding extraction. |
| Loss of Reduction / Recurrent Instability | 10% - 20% | Failure of the bone block to biologically integrate into the clavicle, suture pull-through from the ligament, or premature hardware removal before biological healing is complete. | Prevention: Utilizing the Copeland/Kessel bone block modification significantly mitigates this risk by promoting bone-to-bone healing. Salvage: Revision reconstruction utilizing a free tendon allograft (e.g., semitendinosus) woven in a figure-of-eight fashion, often augmented with synthetic suspensory buttons. |
| Clavicular Osteolysis or Iatrogenic Fracture | 2% - 5% | Over-drilling the clavicular tunnel, placing the screw eccentrically, or creating a severe stress riser during medullary preparation. | Prevention: Precise templating, utilizing a washer to distribute forces, and avoiding oversized drill bits. Salvage: Plate fixation of the clavicle if fractured; debridement and delayed reconstruction for osteolysis. |
| Superficial or Deep Infection | 1% - 3% | Poor soft tissue envelope, hematoma formation, or seeding of the hardware. | Prevention: Meticulous hemostasis, layered fascial closure, and prophylactic antibiotics. Salvage: Prompt aggressive surgical debridement, targeted intravenous antibiotics, and potentially premature hardware removal if the infection tracks deep to the coracoid. |
| Adhesive Capsulitis (Frozen Shoulder) | 5% - 10% | Prolonged immobilization and lack of early, protected passive range of motion. | Prevention: Initiating Phase I pendulum and passive motion exercises immediately post-op. Salvage: Aggressive physical therapy, intra-articular corticosteroid injections, or arthroscopic capsular release in refractory cases. |
Phased Post-Operative Rehabilitation Protocols
The postoperative rehabilitation phase is arguably as critical to the ultimate success of the procedure as the surgical execution itself. Because the modified Weaver-Dunn reconstruction relies entirely on the biological healing and incorporation of the acromial bone block within the distal clavicle, the construct must be rigorously protected from excessive tensile and rotational forces during the early healing phases.
Phase I: Maximum Protection (Weeks 0 to 6)
Immediately following surgery, the patient is placed in a standard, well-padded shoulder sling with an abduction pillow to offload the repair.
* Immobilization: The sling must be worn continuously, including during sleep.
* Activity Modifications: The patient is strictly allowed to use the operative arm only for basic, light activities of daily living (ADLs) at waist level, such as eating, writing, or typing.
* Strict Restrictions: There is an absolute prohibition against any heavy lifting, pushing, pulling, or active elevation of the arm above 90 degrees.
* Therapeutic Exercises: To prevent adhesive capsulitis, pendulum exercises, active elbow, wrist, and hand range of motion, and gentle, closed-chain scapular retractions are initiated on postoperative day one.
Phase II: Intermediate Motion and Early Strengthening (Weeks 6 to 12)
As the bone block begins to consolidate within the clavicle, rehabilitation transitions toward restoring functional motion.
* Sling Weaning: The sling is gradually discontinued in controlled, safe environments, though patients may wear it in crowds for protection.
* Range of Motion: Active-assisted range of motion (AAROM) and active range of motion (AROM) exercises are systematically progressed. Elevation above 90 degrees is cautiously introduced, guided by patient tolerance and the absence of pain.
* Strengthening: Submaximal, pain-free isometric strengthening of the deltoid and the rotator cuff musculature begins. Scapular stabilization exercises are intensified to correct any residual SICK scapula kinematics.
Phase III: Hardware Removal and Advanced Strengthening (Week 12+)
This phase is defined by a mandatory secondary surgical intervention.
* Screw Removal: At exactly 12 weeks postoperatively, the temporary coracoclavicular lag screw must be surgically removed. This is typically performed as a minor, outpatient day-case procedure under local anesthesia with light monitored anesthesia care (MAC) or a brief general anesthetic.
* Biomechanical Rationale for Removal: The normal AC joint requires significant rotation and translation during overhead elevation. Leaving a rigid metallic screw across the dynamic coracoclavicular interval permanently will inevitably lead to metal fatigue and screw breakage, clavicular osteolysis, or severely restricted, painful shoulder mechanics.
* Return to Sport/Work: Following the successful removal of the screw, aggressive, progressive strengthening and sport-specific or occupation-specific rehabilitation commence. Full return to heavy manual labor or contact sports is generally permitted at 5 to 6 months postoperatively, provided the patient has achieved symmetric periscapular strength, dynamic stability, and a full, painless range of motion.
Summary of Landmark Literature and Clinical Guidelines
The surgical management of chronic AC joint dislocations is deeply rooted in decades of evolving orthopaedic literature and biomechanical research. The foundational technique was introduced by Weaver and Dunn in 1972, who first proposed the transfer of the CA ligament to the distal clavicle. While revolutionary, early long-term follow-up studies revealed unacceptably high rates of recurrent deformity, prompting rigorous biomechanical investigations.
Subsequent landmark biomechanical studies, notably those by Rockwood, Mazzocca, and Costic, demonstrated that the native intact CC ligament complex possesses a load-to-failure strength of approximately 500 to 725 Newtons. In stark contrast, the original Weaver-Dunn soft-tissue transfer exhibited a load-to-failure of merely 150 to 200 Newtons, explaining the high clinical failure rates. This biomechanical discrepancy drove the adoption of the Copeland and Kessel modification (the acromial bone block), which studies have shown significantly increases the ultimate pull-out strength and stiffness of the construct by facilitating rapid osseous integration.
Furthermore, the Rockwood and Cadenat modification addressed the critical issue of graft tension. By detaching the anterior fasciculus of the CA ligament, surgeons could reliably achieve tension-free docking, preventing early suture pull-out and graft necrosis.
In the contemporary era, while the open modified Weaver-Dunn procedure remains a gold standard—particularly for revision surgeries—modern advancements have introduced minimally invasive alternatives. Recent literature by Boileau et al. and others has reported excellent short-term outcomes utilizing arthroscopically assisted reconstructions. These modern arthroscopic techniques frequently utilize synthetic cortical buttons and high-tensile suture tapes to recreate the CC ligaments anatomically, often augmented
