Masterclass: Comprehensive Surgical Reconstruction of Acromioclavicular Joint Injuries

Key Takeaway
This masterclass guides fellows through comprehensive AC joint reconstruction. We cover detailed surgical anatomy, meticulous preoperative planning, and step-by-step intraoperative execution of Weaver-Dunn and Anatomic Coracoclavicular Ligament Reconstruction. Learn critical pearls, avoid pitfalls, and master postoperative management. This immersive journey ensures proficiency in managing complex acromioclavicular injuries, providing a pain-free, stable shoulder.
Comprehensive Introduction and Patho-Epidemiology
The acromioclavicular (AC) joint, while anatomically diminutive, serves as the critical kinematic linkage between the axial skeleton and the appendicular upper extremity. As orthopedic surgeons, we must recognize that addressing pathology within this joint is not merely an exercise in aligning osseous structures; it is a complex endeavor aimed at restoring the intricate biomechanical symphony of the shoulder girdle. The AC joint acts as a fundamental pivot point, facilitating the scapular protraction, retraction, upward rotation, and posterior tilt required for fluid, multi-planar upper extremity function. When this joint is compromised, the entire shoulder complex suffers from dyskinesia, weakness, and debilitating pain, severely impacting a patient's quality of life and athletic performance.
Historically, the orthopedic community leaned heavily toward non-operative management for the vast majority of AC joint dislocations, often accepting significant residual deformity in exchange for avoiding surgical morbidity. However, our understanding of the long-term sequelae of high-grade instability has evolved dramatically over the past two decades. We now recognize that chronic, unreduced high-grade injuries (specifically Types IV, V, and select Type III patterns) frequently lead to persistent trapezial and deltoid fatigue, chronic pain, and scapular winging. This paradigm shift has ushered in an era of precision-based, anatomic surgical reconstructions designed to replicate native ligamentous anatomy and restore true tridimensional stability.
Epidemiologically, AC joint injuries account for nearly ten percent of all acute injuries to the shoulder girdle, with a disproportionately high incidence among young, active males participating in contact sports such as rugby, hockey, and American football. The classic mechanism of injury involves a direct, high-energy impact to the lateral aspect of the acromion with the arm in an adducted position, driving the acromion inferiorly and medially while the clavicle remains stabilized by the sternocleidomastoid and trapezius musculature. Less frequently, indirect mechanisms, such as a fall onto an outstretched hand, can transmit superiorly directed forces through the humeral head into the acromion, resulting in sequential ligamentous failure. Understanding these pathomechanical forces is paramount for the operating surgeon, as it dictates the pattern of soft tissue disruption we will encounter in the operating theater.
Evolution of Surgical Paradigms
The surgical management of AC joint instability has undergone a fascinating evolution, transitioning from rigid metallic fixation to dynamic, biologically augmented reconstructions. Early techniques utilizing smooth Kirschner wires or rigid hook plates were fraught with complications, including hardware migration, catastrophic hardware failure, and the inevitable requirement for secondary removal surgeries. Furthermore, these rigid constructs failed to respect the native, multi-axial micromotion inherent to the diarthrodial AC joint, frequently leading to premature acromioclavicular arthrosis and clavicular osteolysis.
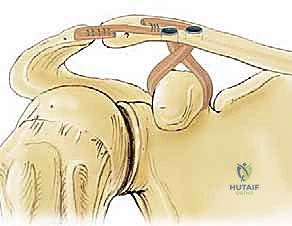
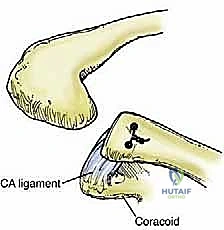
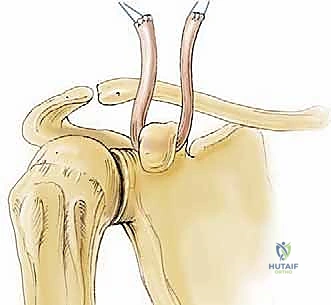
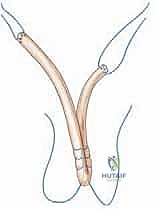
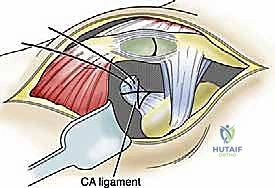
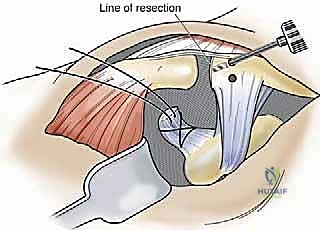
The introduction of the Weaver-Dunn procedure marked a significant advancement, utilizing the transfer of the coracoacromial (CA) ligament to the distal clavicle. While conceptually elegant, biomechanical studies later demonstrated that the native CA ligament possesses merely twenty-five percent of the tensile strength of the native coracoclavicular (CC) complex. Consequently, isolated Weaver-Dunn reconstructions were plagued by unacceptably high rates of recurrent vertical instability, particularly in high-demand laborers and elite athletes. This clinical shortcoming necessitated the development of augmentation strategies, initially utilizing synthetic tapes and subsequently evolving into the modern era of anatomic, free-tissue graft reconstructions.
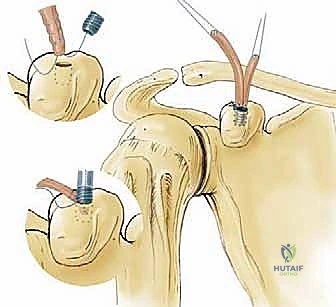
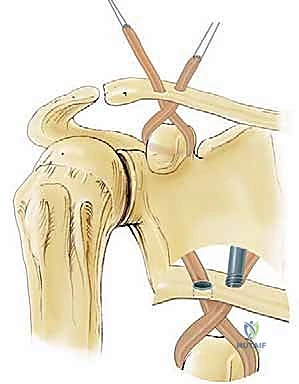
Today, the gold standard for chronic high-grade instability is the Anatomic Coracoclavicular Ligament Reconstruction (ACCR). This technique meticulously recreates both the conoid and trapezoid ligaments utilizing robust autograft or allograft tissue, often augmented with high-tensile suspensory fixation devices. By anatomically restoring the distinct footprints of the native CC ligaments, we re-establish both vertical and horizontal stability, allowing for aggressive postoperative rehabilitation and a durable return to pre-injury activity levels. This masterclass chapter will dissect the nuances of this contemporary approach, providing a definitive roadmap for achieving optimal surgical outcomes.
Detailed Surgical Anatomy and Biomechanics
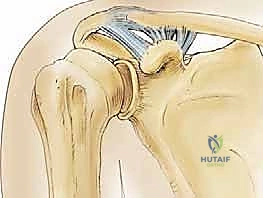
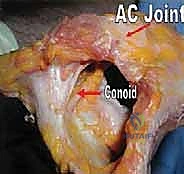
To execute a successful reconstruction, the orthopedic surgeon must possess an encyclopedic knowledge of the AC joint's intricate anatomy and its corresponding biomechanical behavior. The AC joint is classified as a diarthrodial articulation, characterized by the presence of a fibrocartilaginous intra-articular disc, which is often variable in its morphology and tends to undergo rapid degenerative changes by the fourth decade of life. The articular surfaces are incongruent, with the distal clavicle typically overriding the medial acromial facet. This inherent osseous instability dictates that the joint must rely almost entirely on a complex network of static ligamentous restraints and dynamic musculotendinous envelopes to maintain its anatomic reduction during loaded upper extremity motion.
Osteology and Articular Configuration
The distal clavicle and the medial acromion form the osseous foundation of this joint. The distal clavicular articular surface is typically convex and faces laterally, inferiorly, and slightly posteriorly, while the reciprocal acromial facet is concave and faces medially, superiorly, and anteriorly. The inclination angle of the joint in the sagittal plane is highly variable, ranging from relatively vertical to significantly oblique. This morphological variation has clinical implications; a more vertically oriented joint is inherently more susceptible to superior displacement forces, whereas an oblique joint may exhibit a higher propensity for horizontal instability.
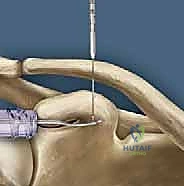
The coracoid process, a critical landmark for surgical reconstruction, projects anteriorly and laterally from the superior border of the scapula. It serves as the foundational anchor for the coracoclavicular ligaments. The base of the coracoid is robust and ideally suited to withstand the significant pull-out forces exerted by modern suspensory fixation buttons and biologic grafts. However, surgeons must be acutely aware of the coracoid's complex three-dimensional geometry to avoid iatrogenic fracture during drilling. The optimal trajectory for a coracoid tunnel is strictly vertical, positioned centrally within the base of the coracoid, posterior to the insertion of the pectoralis minor and the conjoint tendon.
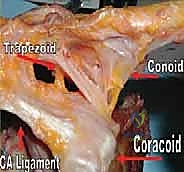
The clavicular footprints of the CC ligaments are equally specific and must be respected during anatomic reconstruction. The conoid tubercle is located on the posteromedial undersurface of the clavicle, approximately 4.5 centimeters medial to the distal articular surface. The trapezoid line is situated more anterolaterally, approximately 3.0 centimeters medial to the articular surface. Failure to accurately replicate these distinct anatomical footprints during tunnel placement will result in a non-anatomic vector of pull, potentially leading to graft failure, recurrent instability, or restricted scapulothoracic kinematics.
Static Ligamentous Restraints
The static stability of the AC joint is governed by two distinct ligamentous complexes: the acromioclavicular (AC) ligaments and the coracoclavicular (CC) ligaments. The AC ligaments consist of superior, inferior, anterior, and posterior capsular thickenings. Biomechanical studies have definitively established that the superior and posterior AC ligaments are the primary restraints to anterior-to-posterior (horizontal) translation of the distal clavicle. Disruption of these specific capsular structures results in significant anteroposterior instability, which can manifest clinically as a painful clunking sensation during cross-body adduction, even in the absence of vertical displacement.
The coracoclavicular (CC) ligament complex, comprising the conoid and trapezoid ligaments, represents the primary restraint to superior-to-inferior (vertical) translation. The conoid ligament is conical and fan-shaped, originating from the posteromedial base of the coracoid and inserting onto the conoid tubercle. Due to its relatively vertical orientation, the conoid exhibits the highest in-situ forces when resisting superior loads. The trapezoid ligament is a broad, quadrilateral structure originating anterior and lateral to the conoid and inserting onto the trapezoid line. Its oblique orientation makes it the primary restraint against axial compression of the AC joint.
Together, the conoid and trapezoid ligaments span the coracoclavicular space, which normally measures between 1.1 and 1.3 centimeters. It is crucial to understand the interplay between these structures. When the AC capsular ligaments are compromised, the CC ligaments are forced to act as secondary restraints to horizontal translation. Specifically, the conoid becomes the primary restraint to anterior loads, while the trapezoid assumes responsibility for resisting posterior loads. This biomechanical redundancy underscores the necessity of addressing both horizontal and vertical instability patterns during comprehensive surgical reconstruction to prevent premature graft elongation.
Dynamic Musculotendinous Stabilizers
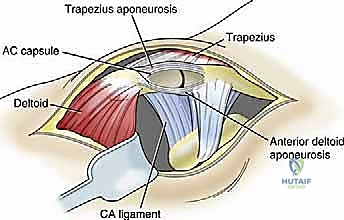
Beyond the static ligaments, the dynamic musculotendinous envelope plays an indispensable role in maintaining AC joint reduction and facilitating normal scapulothoracic rhythm. The deltoid muscle originates from the anterior border of the lateral third of the clavicle, the lateral margin of the acromion, and the spine of the scapula. The trapezius muscle inserts onto the superior border of the lateral third of the clavicle, the medial margin of the acromion, and the superior lip of the scapular spine. The fascial confluence of these two powerful muscles forms the deltotrapezial fascia, which drapes over the superior aspect of the AC joint.
In high-grade AC joint separations (particularly Types IV and V), the distal clavicle is violently driven through this fascial envelope, resulting in extensive stripping of the deltoid and trapezius attachments from the osseous anatomy. This disruption severely compromises the dynamic stability of the shoulder girdle. A critical, yet frequently underappreciated, component of any AC joint reconstruction is the meticulous, watertight imbrication and repair of the deltotrapezial fascia over the distal clavicle.
Failure to achieve a robust fascial repair leaves the underlying biologic graft and hardware vulnerable to the relentless superior pull of the trapezius and the inferior pull of the weight of the arm. Furthermore, an inadequate fascial repair can lead to persistent deltoid dysfunction, cosmetically unacceptable hardware prominence, and chronic, debilitating postoperative pain. Therefore, the surgeon must treat the fascial closure with the same degree of reverence and technical precision as the ligamentous reconstruction itself.
Neurovascular Topography
Navigating the surgical approach to the AC joint and coracoid requires a profound respect for the regional neurovascular topography. The AC joint itself receives dual sensory innervation from the lateral pectoral nerve and the suprascapular nerve. This overlapping innervation pattern explains the often diffuse and challenging nature of clinical pain localization, which can easily be misconstrued as primary glenohumeral or subacromial pathology. Superficial branches of the supraclavicular nerves (C3, C4) cross the clavicle anteriorly; these must be carefully identified and protected during the initial skin incision and subcutaneous dissection to prevent the formation of painful postoperative neuromas or areas of permanent anesthesia over the anterior chest wall.
The most critical neurovascular considerations arise during the deep dissection and preparation of the coracoid process. The coracoid serves as a beacon, but it is surrounded by structures that are entirely unforgiving of surgical error. Medial to the coracoid lies the brachial plexus and the axillary artery and vein. The musculocutaneous nerve typically enters the conjoint tendon approximately 3 to 5 centimeters distal to the coracoid tip, though significant anatomic variations exist.
During the passage of instruments, drills, or graft-passing sutures beneath the base of the coracoid, the surgeon must maintain a strict subperiosteal plane and direct all instrumentation from medial to lateral whenever possible, or utilize carefully placed blunt retractors (such as a Fukuda or a malleable retractor) to shield the medial and inferior neurovascular structures. A catastrophic plunge with a drill bit through the inferior cortex of the coracoid base can result in devastating, limb-threatening injury to the underlying neurovascular bundle. Meticulous hemostasis and direct visualization are non-negotiable tenets of this exposure.
Exhaustive Indications and Contraindications
The decision to proceed with operative intervention for an AC joint injury is rarely black and white; it requires a nuanced synthesis of the patient's physiological age, functional demands, chronicity of the injury, and specific pathoanatomic classification. We are not treating a radiograph; we are treating a patient whose livelihood and quality of life may depend heavily on overhead strength and shoulder endurance. A comprehensive clinical evaluation, coupled with high-quality, specialized radiographic imaging, is the bedrock of our decision-making algorithm.
| Injury Type / Patient Profile | Indication Status | Clinical Rationale and Biomechanical Justification |
|---|---|---|
| Type I & II (Acute) | Absolute Contraindication | Intact or partially intact CC ligaments provide sufficient stability. Excellent outcomes achieved with non-operative management and early functional rehabilitation. |
| Type III (Low Demand / Sedentary) | Relative Contraindication | Non-operative management yields satisfactory functional results in the majority of low-demand patients, avoiding surgical morbidity and hardware complications. |
| Type III (Elite Athlete / Heavy Laborer) | Relative Indication | High-demand overhead athletes or manual laborers may experience chronic pain, fatigue, and scapular dyskinesia with conservative care. Early anatomic reconstruction may expedite return to peak performance. |
| Type IV (Posterior Displacement) | Absolute Indication | Clavicle is buttonholed posteriorly into the trapezius muscle. Irreducible closed; leads to severe chronic pain and severe horizontal instability. Requires open reduction and stabilization. |
| Type V (Severe Superior Displacement) | Absolute Indication | Massive soft tissue disruption including deltotrapezial fascia. Results in profound scapular ptosis, cosmetic deformity, and debilitating weakness. Operative reconstruction is mandatory. |
| Type VI (Inferior Dislocation) | Absolute Indication | Extremely rare, high-energy injury. Clavicle rests in subcoracoid or subacromial position. High risk of neurovascular compromise and severe functional limitation. Surgical reduction required. |
| Chronic Symptomatic Type III-V (>3 months) | Absolute Indication | Persistent pain and disability despite exhaustive conservative management. Native ligaments are scarred and non-functional, necessitating biologic graft reconstruction (ACCR). |
| Active Local/Systemic Infection | Absolute Contraindication | High risk of deep space infection, graft necrosis, and catastrophic failure. Infection must be entirely eradicated prior to elective reconstructive procedures. |
Clinical Evaluation and Diagnostic Imaging
The clinical examination begins with a thorough history, focusing on the mechanism of injury, the onset of symptoms, and the patient's specific occupational and athletic requirements. Inspection often reveals a prominent distal clavicle, though in acute settings, massive swelling may obscure the deformity. Palpation will elicit exquisite point tenderness directly over the AC joint and the coracoclavicular interspace. The hallmark of horizontal instability is elicited via the cross-arm adduction test, which compresses the AC joint and stresses the posterior capsule, generating localized pain.
To differentiate AC joint pathology from concomitant glenohumeral or labral injuries, the O'Brien active compression test is highly utility. Pain localized to the superior aspect of the shoulder during the internally rotated phase of the test, which is subsequently relieved by external rotation, strongly suggests AC joint involvement. However, clinical examination alone is insufficient for surgical planning; a definitive radiographic series is mandatory.

Standard anteroposterior (AP) and true scapular Y views are obtained, but they often fail to adequately profile the AC joint due to superimposition of the scapular spine. The Zanca view is the absolute gold standard for evaluating the AC joint in the coronal plane. By tilting the X-ray beam 10 to 15 degrees cephalad and utilizing approximately fifty percent of the standard penetration voltage, the AC joint is projected entirely free of underlying osseous structures.


The axillary lateral view is equally critical, as it is the only reliable modality for identifying the posterior displacement characteristic of a Type IV injury. Furthermore, a Stryker notch view should be obtained if there is any clinical suspicion of a concomitant coracoid base fracture, which would fundamentally alter the surgical approach and fixation strategy.

The Rockwood Classification System
The Rockwood classification system remains the universally accepted framework for categorizing AC joint injuries, guiding both prognosis and therapeutic intervention. It is predicated on the degree and direction of distal clavicle displacement relative to the acromion, which serves as a surrogate marker for the extent of ligamentous and fascial disruption. Type I injuries represent a simple sprain of the AC capsular ligaments without macroscopic disruption, yielding normal radiographs. Type II injuries involve a complete rupture of the AC ligaments but an intact CC complex, resulting in widening of the AC joint but minimal vertical displacement on the Zanca view. Both Type I and II injuries are universally managed non-operatively.
Type III injuries are characterized by complete disruption of both the AC and CC ligaments, resulting in a 25% to 100% increase in the coracoclavicular interspace compared to the uninjured contralateral shoulder. The management of Type III injuries remains the most heavily debated topic in shoulder trauma. While the majority of patients tolerate this displacement well, a subset of high-demand individuals will develop chronic, debilitating symptoms. Type IV injuries involve posterior displacement of the distal clavicle into or through the trapezius muscle, often visible only on the axillary radiograph.
Type V injuries represent a catastrophic failure of the entire suspensory complex, including the AC ligaments, CC ligaments, and the deltotrapezial fascia. Radiographically, the CC interspace is increased by 100% to 300%. The profound inferior translation of the scapula (scapular ptosis) results in a severe cosmetic deformity and devastating functional weakness. Type VI injuries are exceptionally rare, characterized by inferior dislocation of the distal clavicle into a subacromial or subcoracoid position, often requiring urgent open reduction due to impending neurovascular compromise. Types IV, V, and VI are universally considered absolute indications for surgical reconstruction.
Decision-Making Matrix
When evaluating a patient for surgery, particularly in the controversial Type III cohort, the surgeon must employ a multifaceted decision-making matrix. Hand dominance is a critical factor; a Type III injury in the dominant arm of an elite tennis player warrants a much more aggressive surgical posture than the same injury in the non-dominant arm of a sedentary office worker. The chronicity of the injury also dictates the surgical technique. Acute injuries (less than 3 to 4 weeks old) may be amenable to primary repair of the native ligaments augmented with suspensory fixation.
Conversely, chronic injuries (greater than 6 weeks old) invariably require biologic reconstruction utilizing autograft or allograft tissue, as the native ligaments have undergone irreversible retraction, scarring, and biological degradation. The choice between autograft (typically semitendinosus) and allograft is discussed extensively with the patient. Autograft provides superior biological incorporation but carries the morbidity of a secondary harvest site. Allograft eliminates donor site morbidity and reduces operative time but carries a theoretical, albeit infinitesimally small, risk of disease transmission and slightly delayed incorporation. In our academic practice, we heavily favor robust allograft tissue for chronic ACCR to minimize surgical trauma while providing an exceptional biomechanical scaffold.
Pre-Operative Planning, Templating, and Patient Positioning
The success of a complex AC joint reconstruction is largely determined before the scalpel ever touches the skin. Meticulous preoperative planning, precise radiographic templating, and flawless patient positioning are absolute prerequisites for a smooth, efficient, and complication-free surgical execution. The operating theater must be prepared with the necessary specialized equipment, including high-tensile suture tapes, cortical suspensory buttons, appropriately sized drill bits, and biologic grafts pre-thawed if utilizing allograft.
Anesthesia and Operating Room Setup
The procedure is universally performed under general endotracheal anesthesia to ensure complete muscle relaxation, which is critical for mobilizing the chronically retracted scapula and achieving an anatomic reduction of the AC joint. We routinely advocate for the administration of a preoperative interscalene regional nerve block, typically performed under ultrasound guidance by our anesthesia colleagues. This block provides profound, opioid-sparing analgesia during the immediate postoperative period, significantly enhancing patient comfort and facilitating early, painless passive range of motion.
The operating room must be configured to allow unrestricted access to the operative shoulder, with the fluoroscopy unit (C-arm)
Clinical & Radiographic Imaging Archive