Acromioclavicular Joint Injuries: Comprehensive Surgical Management
Key Takeaway
Acromioclavicular (AC) joint injuries typically result from a direct downward force on the acromion. Management is dictated by the Rockwood classification, which assesses the integrity of the AC and coracoclavicular (CC) ligaments, alongside the deltotrapezial fascia. While Types I through III are generally managed non-operatively, Types IV, V, and VI require surgical intervention to restore biomechanical stability and shoulder kinematics.
Comprehensive Introduction and Patho-Epidemiology
Historical Context and Epidemiological Trends
The acromioclavicular (AC) joint represents a critical, complex biomechanical linkage between the appendicular upper extremity and the axial skeleton. Hippocrates was the first to distinctly differentiate acromioclavicular joint dislocations from glenohumeral dislocations, accurately delineating their unique mechanisms of injury and resulting clinical deformities. In contemporary orthopedic practice, AC joint injuries account for approximately 9% to 12% of all shoulder girdle injuries in the general population, with the incidence skyrocketing to over 40% within athletic cohorts, particularly those engaged in collision sports such as rugby, American football, and ice hockey. The demographic distribution is heavily skewed toward young, active males in their second and third decades of life, with a male-to-female ratio approaching 5:1.
Mechanisms of Injury: Direct Versus Indirect Trauma
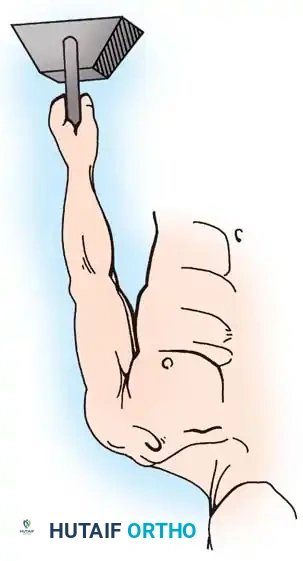
The patho-epidemiology of AC joint disruption is fundamentally categorized into direct and indirect mechanisms of trauma. The overwhelming majority of these injuries—upwards of 70%—are the result of a direct force applied to the superior aspect of the acromion with the glenohumeral joint in an adducted position. During such an impact, the clavicle is driven inferiorly until it abuts the first rib, which acts as a fulcrum blocking further downward excursion. As the kinetic energy of the trauma continues to drive the scapula and acromion inferiorly and medially, sequential and catastrophic stress is applied to the stabilizing capsuloligamentous structures. If the clavicular diaphysis does not yield to fracture, the acromioclavicular ligaments rupture first, followed by the robust coracoclavicular (CC) ligaments, and finally, the stabilizing deltotrapezial fascial envelope is torn.
Conversely, indirect mechanisms of injury are significantly less common and typically occur following a fall onto an outstretched hand (FOOSH). In this scenario, the impact force is transmitted longitudinally up the upper extremity, driving the humeral head superiorly into the acromion and the glenoid fossa. This superiorly directed force primarily stresses the acromioclavicular ligaments and the intra-articular disc. Indirect injuries generally result in lower-grade sprains (Rockwood Types I and II) and rarely possess the kinetic energy required to completely disrupt the robust coracoclavicular ligamentous complex. However, they are frequently associated with concomitant intra-articular glenohumeral pathology, such as superior labral anterior-posterior (SLAP) tears.
The Rockwood Classification and Pathoanatomic Correlation
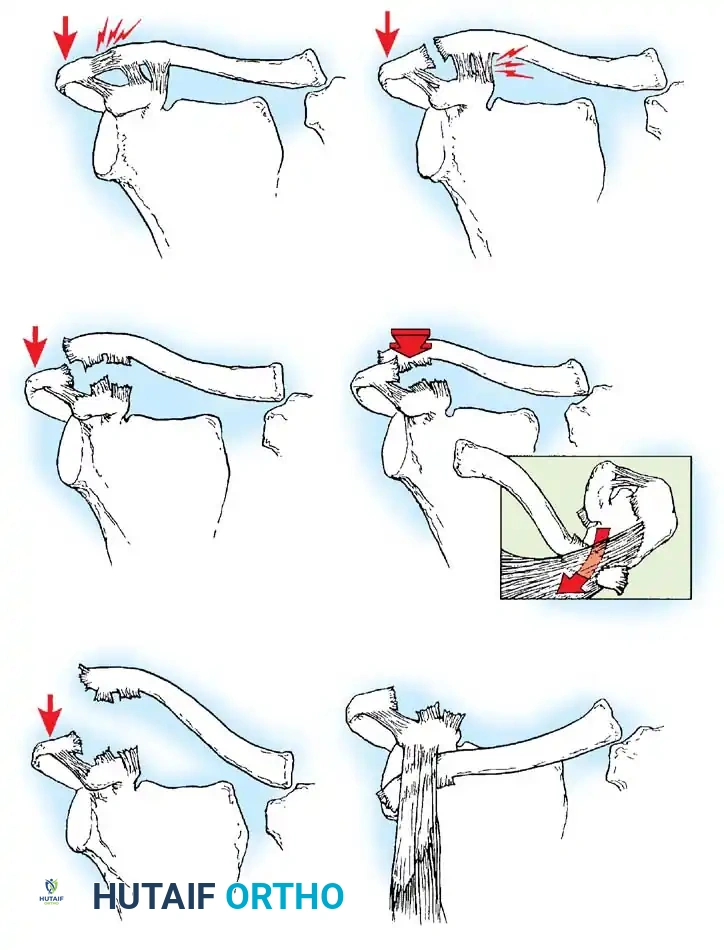
The universally adopted Rockwood classification system provides a critical framework for understanding the pathoanatomy and guiding the surgical management of AC joint injuries. This six-type system expands upon the earlier, less granular classifications by Sage and Salvatore. Type I injuries represent a simple sprain of the AC ligaments with an intact joint capsule and CC ligaments. Type II injuries involve a complete rupture of the AC ligaments and joint capsule, resulting in horizontal instability, while the CC ligaments remain intact. Type III injuries are characterized by the complete disruption of both the AC and CC ligaments, leading to 100% superior displacement of the clavicle relative to the acromion, primarily due to the inferior ptosis of the scapula.
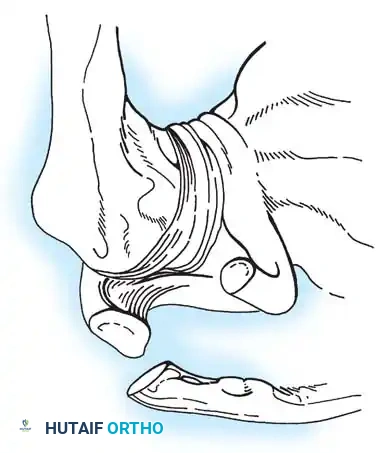
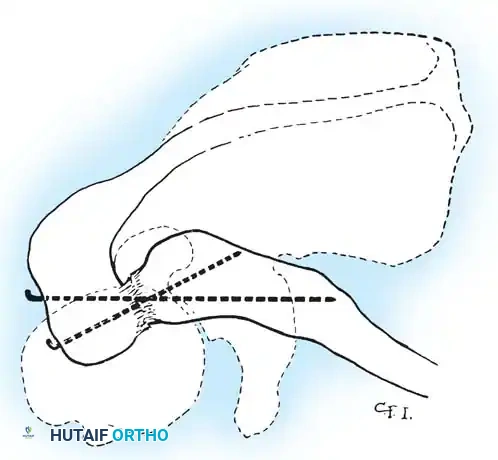
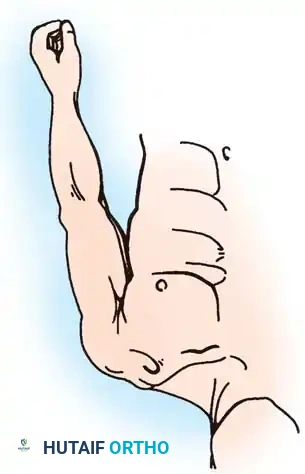
High-grade injuries (Types IV, V, and VI) represent severe soft-tissue trauma requiring meticulous surgical intervention. Type IV injuries involve posterior displacement of the distal clavicle into or through the trapezius muscle, often incarcerating the clavicle within the muscle belly. Type V injuries are severe Type III variants characterized by massive disruption of the deltotrapezial fascia, resulting in 100% to 300% superior displacement of the clavicle and a grossly irreducible deformity. Type VI, an exceedingly rare injury caused by severe hyperabduction and external rotation, involves the inferior dislocation of the distal clavicle beneath the coracoid process, often coming to rest posterior to the conjoined tendon. Understanding these distinct pathoanatomic states is paramount for the orthopedic surgeon when formulating a comprehensive operative plan.
Detailed Surgical Anatomy and Biomechanics
Osteology and the Intra-Articular Disc
The acromioclavicular joint is a diarthrodial articulation with variable morphology. The articular surfaces are typically incongruent, flat, or slightly oblique, predisposing the joint to inherent osseous instability. The distal clavicle articulates with the medial facet of the acromion, and the joint space contains a fibrocartilaginous intra-articular disc. This meniscus-like structure is complete in the pediatric population but undergoes rapid, predictable degeneration by the fourth decade of life, often leaving only a meniscoid rim in adults. This early degeneration explains the high prevalence of asymptomatic AC joint arthrosis observed on routine shoulder radiographs in older patients. The osseous anatomy dictates that stability is almost entirely reliant on the surrounding ligamentous and musculofascial envelope.
The Static Stabilizers: AC and CC Ligaments
The static stability of the AC joint is governed by a complex, synergistic relationship between the acromioclavicular (AC) ligaments and the coracoclavicular (CC) ligaments. The AC capsuloligamentous complex consists of superior, inferior, anterior, and posterior bundles. Biomechanical studies, notably those by Fukuda and Mazzocca, have definitively demonstrated that the superior AC ligament is the most robust and serves as the primary restraint to anteroposterior (horizontal) translation of the distal clavicle. Disruption of these ligaments leads to the horizontal instability pathognomonic of Type II injuries.
The coracoclavicular (CC) ligaments—the conoid and the trapezoid—are the primary suspensory restraints preventing superior and inferior translation of the scapula relative to the clavicle. The conoid ligament is cone-shaped, located posteromedially, and inserts on the conoid tubercle of the clavicle, approximately 45 millimeters medial to the distal articular surface. It is the primary restraint to superior translation. The trapezoid ligament is broader, located anterolaterally, and inserts on the trapezoid line, approximately 25 millimeters medial to the distal clavicle. The trapezoid primarily resists axial compression driving the acromion medially toward the clavicle. Precise knowledge of these anatomic footprints is critical when performing anatomic CC ligament reconstructions.
The Dynamic Stabilizers: The Deltotrapezial Fascia
Beyond the static ligaments, the dynamic stability of the AC joint is profoundly dependent on the muscular attachments of the anterior deltoid and the trapezius muscles. These muscles interdigitate over the superior aspect of the distal clavicle and acromion, forming the robust deltotrapezial fascia. This fascial sleeve acts as a dynamic tension band, actively compressing the AC joint during upper extremity motion and assisting in the suspension of the shoulder girdle.
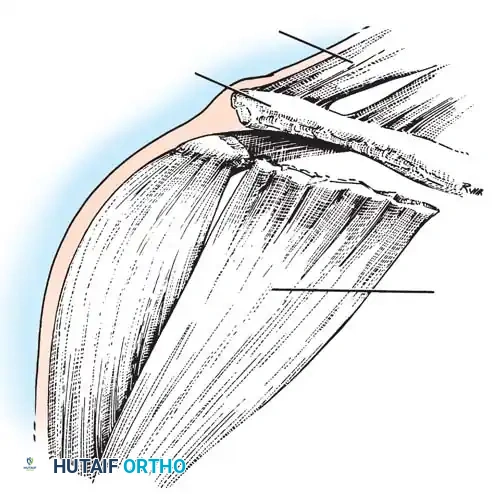
In high-grade AC joint dislocations (Rockwood Types III, IV, and V), the clavicular attachments of the deltoid and trapezius are violently avulsed. Horn and other pioneering surgeons noted that the degree of superior clavicular displacement is directly proportional to the extent of tearing in this fascial envelope. Therefore, any surgical intervention that fails to meticulously imbricate and repair the deltotrapezial fascia will inevitably result in persistent dynamic instability, hardware failure, and poor clinical outcomes, regardless of the strength of the osseous or ligamentous fixation employed.
Biomechanical Implications for Surgical Reconstruction
Understanding the native biomechanics of the AC joint is essential for evaluating modern surgical constructs. The intact AC joint allows for approximately 5 to 8 degrees of motion in all planes (rotation, elevation, and AP translation) during synchronous scapulothoracic movement. Rigid fixation techniques, such as transarticular pinning or rigid coracoclavicular lag screws (Bosworth screws), eliminate this obligate micro-motion. Consequently, if these rigid implants are not removed prior to the resumption of normal shoulder kinematics, they are subjected to immense cyclical loading and will inevitably undergo fatigue failure, leading to screw breakage or clavicular osteolysis. Modern reconstructive techniques emphasize "semi-rigid" or biological fixation—utilizing cortical buttons, high-tensile suture tapes, and free tendon grafts—which permit physiologic micro-motion while maintaining anatomic reduction during the ligamentous healing phase.
Exhaustive Indications and Contraindications
Evidence-Based Operative Indications
The decision-making algorithm for the management of AC joint injuries is heavily dictated by the Rockwood classification, patient chronologic and physiologic age, hand dominance, and occupational or athletic demands. Rockwood Types I and II are universally managed non-operatively, with excellent long-term functional outcomes. Conversely, high-grade injuries—specifically Types IV, V, and VI—carry absolute indications for surgical intervention. In these severe dislocations, the massive displacement of the clavicle, gross disruption of the deltotrapezial fascia, and interposition of soft tissue (such as the trapezius muscle in Type IV injuries) preclude any possibility of spontaneous healing or acceptable functional recovery without anatomical reduction and stable fixation.
The management of Type III injuries remains one of the most fiercely debated topics in orthopedic sports medicine. Historically, many surgeons advocated for early operative intervention to restore anatomy and maximize strength. However, prospective, randomized multicenter trials, including those by the Canadian Orthopaedic Trauma Society (COTS), have demonstrated that non-operative management of Type III injuries yields equivalent, and sometimes superior, functional outcomes compared to surgery, with significantly fewer complications. Currently, the consensus recommendation is an initial trial of non-operative management for the vast majority of Type III injuries. Operative intervention for acute Type III injuries is reserved for a highly select cohort: elite overhead athletes, heavy manual laborers who require sustained overhead strength, and patients with severe scapular dyskinesia or profound cosmetic intolerance of the deformity.
Contraindications to Surgical Intervention
While surgical reconstruction is critical for high-grade injuries, several absolute and relative contraindications must be respected to avoid catastrophic complications. Absolute contraindications include active local or systemic infection, severe medical comorbidities rendering the patient unfit for general anesthesia, and an inadequate soft-tissue envelope (e.g., severe abrasions, burn wounds, or active dermatologic conditions over the surgical site) that would compromise wound healing and increase the risk of deep infection.
Relative contraindications revolve around patient compliance and chronicity. Patients with severe psychiatric disorders, active substance abuse, or a demonstrated inability to adhere to strict, prolonged postoperative rehabilitation protocols are poor candidates for surgical reconstruction. In these populations, the risk of early hardware failure, loss of reduction, and recurrent instability far outweighs the potential benefits of surgery. Furthermore, in chronic asymptomatic Type III injuries discovered incidentally, surgical intervention is contraindicated, as the patient has already achieved functional compensation.
Tabular Summary of Indications and Contraindications
| Clinical Scenario / Factor | Operative Management | Non-Operative Management | Rationale / Clinical Notes |
|---|---|---|---|
| Rockwood Type I & II | Contraindicated | Indicated | Ligaments are sprained or partially torn; joint remains biomechanically stable. Excellent outcomes with rehab. |
| Rockwood Type III (Acute) | Relative Indication | Primary Indication | Initial conservative approach preferred. Surgery reserved for elite overhead athletes or heavy laborers. |
| Rockwood Type IV, V, VI | Absolute Indication | Contraindicated | Massive soft tissue disruption, muscle interposition, and gross instability require anatomic restoration. |
| Chronic Symptomatic Type III | Indicated | Failed | Requires distal clavicle excision (Mumford) combined with CC ligament reconstruction. |
| Poor Soft Tissue Envelope | Absolute Contraindication | Indicated | High risk of deep hardware infection and wound dehiscence. Delay surgery until soft tissues recover. |
| Non-Compliant Patient | Relative Contraindication | Indicated | High risk of construct failure (button pull-out, graft rupture) if postoperative restrictions are ignored. |
Pre-Operative Planning, Templating, and Patient Positioning
Comprehensive Clinical Evaluation
Meticulous pre-operative planning begins with a comprehensive clinical examination. Patients with acute high-grade AC joint injuries present with profound localized pain, extensive ecchymosis, and a visually striking step-off deformity. The "piano key" sign is pathognomonic: the superiorly displaced lateral clavicle can be manually depressed into an anatomic position but immediately rebounds superiorly when pressure is released, demonstrating the complete loss of suspensory CC ligament integrity. The surgeon must carefully evaluate the integrity of the overlying skin, as severe Type V injuries can cause skin tenting, leading to pressure necrosis if not reduced emergently. Furthermore, a thorough neurovascular examination of the upper extremity is mandatory to rule out concomitant brachial plexus traction injuries or subclavian vessel compromise, particularly in high-energy trauma.
Advanced Radiographic Assessment
Standard anteroposterior (AP) views of the shoulder are notoriously inadequate for evaluating the AC joint, as the X-ray beam overpenetrates the superficial joint, obscuring subtle pathology. A dedicated Zanca view is mandatory. This is an AP radiograph taken with a 10° to 15° cephalad tilt, utilizing only 50% of the standard penetrance used for a glenohumeral radiograph. This specific trajectory removes the superimposition of the scapular spine and clearly delineates the AC joint articulation. An axillary lateral view is equally critical; it is the only reliable method to diagnose the posterior horizontal displacement characteristic of a Type IV injury.

To accurately classify the degree of vertical displacement (differentiating a Type III from a Type V), bilateral panoramic AP views of the shoulder girdle are obtained with the patient standing erect. The uninjured side serves as the patient's internal baseline. Historically, stress radiographs utilizing 10 to 15 lb weights were advocated to unmask occult instability. However, modern orthopedic consensus has largely abandoned stress views. If utilized, the weights must be suspended from the patient's wrists via straps; if the patient actively grips the weights, the reflex contraction of the deltoid and trapezius muscles can artificially reduce the joint, leading to a false-negative assessment of the instability.
Surgical Templating and Construct Selection
Pre-operative templating involves precise measurement of the coracoclavicular distance on the uninjured side to guide the intra-operative reduction. The surgeon must also evaluate the morphology of the coracoid process. A hypoplastic, narrow, or previously fractured coracoid process may preclude the use of large drill holes required for modern cortical button techniques, necessitating a shift toward suture anchor fixation or subcoracoid cerclage techniques. The chronicity of the injury heavily influences construct selection: acute injuries (less than 3-4 weeks old) are amenable to primary repair and stabilization (e.g., suspensory cortical buttons), whereas chronic injuries require biological augmentation, such as a free semitendinosus allograft reconstruction, to achieve long-term stability.
Patient Positioning and Operating Room Setup
The patient is typically placed in the beach-chair position, with the backrest elevated to 30° to 45°. This positioning allows gravity to assist in reducing the inferiorly displaced scapula and provides excellent access to the superior shoulder girdle. The head is secured in a neutral position using a specialized headrest to avoid traction on the cervical spine and brachial plexus. The operative arm must be draped free to allow for full manipulation during the procedure; an articulated arm positioner (e.g., Spider arm or Mayo stand) is highly advantageous for maintaining the arm in a reduced, supported position during fixation. The C-arm fluoroscopy unit is brought in from the contralateral side or the head of the bed, ensuring that orthogonal views (AP and axillary) can be obtained seamlessly without compromising the sterile field.
Step-by-Step Surgical Approach and Fixation Technique
The Surgical Approach: Incision and Dissection
The surgical approach must provide comprehensive access to the AC joint, the distal clavicle, and the coracoid process while preserving the critical soft-tissue envelope. A sabre-cut incision is placed in Langer's lines, beginning 1 to 2 cm posterior to the AC joint and extending anteriorly over the tip of the coracoid process. Full-thickness fasciocutaneous flaps are meticulously elevated to expose the underlying deltotrapezial fascia.
The fascia is incised longitudinally in line with the clavicle, and subperiosteal dissection is utilized to reflect the anterior deltoid and the trapezius. In acute high-grade injuries, this fascial layer is often already violently torn, and the surgeon must carefully identify and tag the retracted edges with heavy non-absorbable sutures for later repair. The AC joint is then exposed, and any interposed tissue—typically the torn intra-articular disc or frayed capsular remnants—is aggressively debrided to allow for an anatomic reduction.
Technique 1: Anatomic Coracoclavicular (CC) Reconstruction
Modern surgical management heavily favors anatomic or near-anatomic reconstruction of the CC ligaments. For acute injuries, a suspensory cortical button construct is frequently utilized.
Under direct visualization, the base of the coracoid is exposed. A guide pin is drilled from the superior aspect of the clavicle (targeting the anatomic footprint of the conoid ligament, approximately 45 mm medial to the AC joint) directly through the central axis of the coracoid base. A cannulated drill is used to create the tunnel. A high-tensile suture tape construct with a distal cortical button is passed through the clavicle and shuttled under the coracoid. The button is deployed beneath the coracoid base, and the clavicle is anatomically reduced by elevating the arm and depressing the clavicle. The superior button is then tied over the clavicular cortex. This technique provides exceptional biomechanical strength while allowing the micro-motion necessary for primary ligamentous healing.
Technique 2: Biological Augmentation for Chronic Injuries
In chronic injuries (typically greater than 4 to 6 weeks post-trauma), the native ligaments have scarred and lost their healing potential. Relying solely on synthetic fixation in this setting leads to an unacceptably high rate of late hardware failure. Therefore, biological augmentation is mandatory.
The gold standard is an anatomic CC ligament reconstruction utilizing a free tendon graft (e.g., semitendinosus autograft or allograft). Following a distal clavicle excision (Mumford procedure) to prevent AC joint impingement, two bone tunnels are drilled in the clavicle corresponding to the conoid and trapezoid footprints. The tendon graft is looped under the base of the coracoid, and the two limbs are passed through the clavicular tunnels. The graft is tensioned and secured with interference screws or cortical buttons. This biological reconstruction restores the native V-shaped orientation of the CC ligaments, providing robust, long-term stability against both superior and horizontal translation.
Technique 3: Transarticular Fixation and Hook Plates
Historically, transarticular pinning with Kirschner wires (Murray, Phemister techniques) was popular but has been largely abandoned due to catastrophic complications, including wire migration into the thoracic cavity or heart.
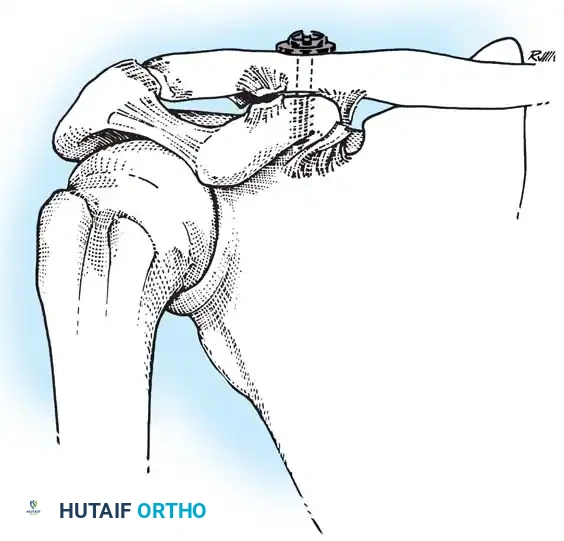
An alternative modern rigid fixation technique is the use of an AO Hook Plate. The plate is fixed to the superior clavicle with locking screws, and the hook is passed under the posterior aspect of the acromion, levering the clavicle into a reduced position. While biomechanically strong and useful in cases of concomitant distal clavicle fractures, the hook plate violates the subacromial space, frequently causing subacromial impingement, rotator cuff abrasion, and acromial osteolysis. Furthermore, it mandates a secondary surgical procedure for hardware removal at 3 to 4 months post-operatively.
Technique 4: Deltotrapezial Imbrication and Closure
Regardless of the osseous or ligamentous fixation technique employed, the operation is incomplete without a meticulous, watertight repair of the deltotrapezial fascia.
The previously tagged fascial edges are brought together over the superior clavicle in a "pants-over-vest" imbricated fashion using heavy, non-absorbable figure-of-eight sutures. This robust repair restores the dynamic tension band effect of the musculature, which is absolutely critical for shielding the underlying CC reconstruction from early cyclical loading and failure. The subcutaneous tissues and skin are then closed in standard fashion.
Complications, Incidence Rates, and Salvage Management
Hardware Failure and Loss of Reduction
Despite advancements in surgical technique, complications following AC joint reconstruction remain clinically significant. The most common complication is a partial or complete loss of reduction, occurring in 15% to 30% of cases, particularly when utilizing suspensory cortical button constructs. This failure typically results from button pull-through through the clavicular or coracoid cortex, suture tape breakage, or gradual creeping of the biological graft. Meticulous surgical technique, including the use of washers to distribute force over the clavicular cortex and ensuring central placement of the coracoid drill hole, is essential to minimize this risk. Fortunately, a mild asymptomatic loss of reduction (subluxation) rarely compromises the final functional outcome and typically does not require revision surgery.
Fractures of the Coracoid and Clavicle
Iatrogenic fractures of the coracoid process or the clavicle are devastating complications associated with modern anatomic reconstructive techniques. Drilling large tunnels (e.g., 4.5 mm to 5.5 mm) through the relatively small footprint of the coracoid base creates a significant stress riser. If the drill hole is placed too medially, too laterally, or if multiple passes are made, the coracoid can fracture under the tension of the reconstruction. Similarly, placing the clavicular tunnels too close together or too close to the anterior/posterior cortices predisposes the clavicle to fracture. Management of these fractures is exceedingly complex, often requiring transition to a hook plate or complex subcoracoid cerclage salvage techniques.
Infection and Distal Clavicle Osteolysis
Superficial and deep surgical site infections occur in approximately 2% to 4% of AC joint reconstructions. The superior shoulder has a relatively thin subcutaneous envelope, making prominent hardware (such as large knots or plates) susceptible to skin breakdown and subsequent infection. Distal clavicle osteolysis and post-traumatic AC joint arthrosis are common late complications, particularly following rigid fixation techniques or non-operative management of high-grade injuries. Patients present with insidious onset of pain exacerbated by cross-body adduction.
Tabular Summary of Complications and Salvage Strategies
| Complication | Estimated Incidence | Etiology / Risk Factors | Salvage Management Strategy |
|---|---|---|---|
| Loss of Reduction (Subluxation) | 15% - 30% | Suture stretch, graft creep, poor tissue quality. | If asymptomatic: Observe. If symptomatic: Revision reconstruction with allograft. |
| Coracoid / Clavicle Fracture | 2% - 5% | Eccentric drill holes, oversized tunnels, stress risers. | Hook plate fixation, subcoracoid cerclage wiring, open reduction internal fixation (ORIF). |
| AC Joint Arthrosis / Osteolysis | 10% - 20% | Cartilage trauma, rigid transarticular fixation, micro-instability. | Distal Clavicle Excision (Mumford procedure) via open or arthroscopic approach. |
| Deep Infection | 1% - 3% | Prominent hardware, poor soft tissue envelope, diabetes. | Aggressive I&D, hardware removal (if stable), IV antibiotics. |
| Hardware Irritation / Prominence | 10% - 15% | Prominent suture knots, superficial plate placement. | Minor procedure for knot excision or hardware removal after clinical healing (4-6 months). |
Phased Post-Operative Rehabilitation Protocols
Phase I: Maximum Protection (Weeks 0 to 4)
The ultimate success of any AC joint reconstruction is intrinsically linked to strict adherence to a phased postoperative rehabilitation protocol. The primary goal of Phase I is the absolute protection of the surgical construct and the healing deltotrapezial fascia. The patient is placed in a well-padded sling with an abduction pillow immediately post-operatively. The sling must be worn at all times, including during sleep. Rehabilitation is limited to active range of motion (ROM) of the cervical spine, elbow, wrist, and hand to prevent distal stiffness. Passive and active-assisted forward elevation of the shoulder is strictly limited to 90 degrees. Cross-body adduction, internal rotation behind the back, and any active lifting are absolutely contraindicated, as these motions place immense sheer and tensile stress on the healing CC ligaments and fascial repair.
Phase II: Controlled Motion (Weeks 4 to 8)
At the 4-week mark, provided there is clinical evidence of soft-tissue healing and no radiographic loss of reduction, the patient is gradually weaned from the sling. The focus shifts to restoring full passive and active-assisted range of motion. Pulleys and wand exercises are introduced to facilitate forward elevation and external rotation. Active range of motion is initiated, but patients are instructed to avoid any lifting heavier than a cup of coffee. Cross-body adduction remains restricted until the end of week 8 to prevent compression of the AC joint and stress on the posterior capsule. Scapular mobilization and isometric periscapular strengthening are initiated to correct the scapular dyskinesia that inevitably develops during immobilization.
Phase III: Early Strengthening (Weeks 8 to 12)
By week 8, the biological healing of the ligaments and fascia is generally sufficient to withstand mild to moderate resistance. The protocol progresses to progressive isotonic strengthening of the rotator cuff, deltoid, and periscapular
