Surgical Management of Acromioclavicular Joint Dislocations: Resection and Reconstruction Techniques
Key Takeaway
The surgical management of acromioclavicular (AC) joint dislocations requires a nuanced understanding of coracoclavicular ligament integrity. While the Mumford procedure (distal clavicle resection) is highly effective for chronic, symptomatic Grade I and II injuries with intact ligaments, high-grade chronic dislocations (Grades III-V) necessitate robust coracoclavicular reconstruction, such as the Weaver-Dunn or Rockwood techniques, to restore biomechanical stability and prevent debilitating shoulder hypermobility.
Comprehensive Introduction and Patho-Epidemiology
The acromioclavicular (AC) joint serves as the critical, solitary articular linkage suspending the entire appendicular skeleton of the upper extremity from the axial skeleton. Disruptions of this joint are ubiquitous in orthopedic traumatology, accounting for approximately 9% to 12% of all shoulder girdle injuries in the general population, and an even higher proportion—up to 40%—in athletic cohorts engaged in contact sports such as rugby, American football, and ice hockey. The mechanism of injury is classically a direct compressive force applied to the superior aspect of the acromion with the arm in an adducted position. This force drives the acromion and the entire scapula violently inferiorly and medially, while the clavicle is restrained in its anatomic position by the sternocleidomastoid musculature and the sternoclavicular joint, resulting in sequential failure of the supporting ligamentous structures.
The pathophysiology of AC joint dislocation follows a predictable, sequential cascade of soft tissue failure that directly correlates with the applied kinetic energy. Initially, the relatively weak acromioclavicular ligaments and the joint capsule fail, resulting in localized AC joint instability without gross superior migration of the clavicle (Rockwood Grades I and II). As the deforming force continues, the robust coracoclavicular (CC) ligaments—the conoid and trapezoid—are subjected to massive tensile loads until catastrophic failure occurs. Finally, in the most severe injuries, the deltotrapezial fascia is stripped from the distal clavicle, allowing the clavicle to buttonhole through the musculature, resulting in profound, multidirectional instability of the shoulder girdle (Rockwood Grades III, IV, and V).
Historically, the management of these injuries was fraught with controversy, oscillating between benign neglect and aggressive, often morbid, surgical interventions. Early surgical techniques focused heavily on non-anatomic repairs, such as primary acromioclavicular pinning or isolated distal clavicle resections, which frequently failed to address the underlying biomechanical deficit of the coracoclavicular interval. Over the past several decades, a paradigm shift has occurred within the orthopedic community. The contemporary surgical philosophy emphasizes a deep understanding of the native biomechanics, advocating for either dynamic ligamentous transfers, such as the Weaver-Dunn procedure, or modern anatomic reconstructions utilizing free tendon grafts and cortical suspensory fixation devices.
Understanding the patho-epidemiology of AC joint dislocations is not merely an academic exercise; it is the fundamental basis upon which all surgical decision-making must rest. The chronicity of the injury plays a pivotal role in the biological healing potential of the native tissues. Acute injuries (typically defined as those presenting within 3 to 4 weeks) may be amenable to primary repair or acute suspensory fixation, as the native ligaments retain some healing capacity. Conversely, chronic unreduced dislocations are characterized by retracted, atrophic, and biologically inert ligamentous remnants. In these chronic scenarios, primary repair is universally doomed to failure, necessitating complex reconstructive strategies to restore the stabilizing forces of the coracoclavicular complex and mitigate the debilitating sequelae of chronic shoulder dysfunction, periscapular pain, and scapular dyskinesia.
Detailed Surgical Anatomy and Biomechanics
The acromioclavicular joint is a complex diarthrodial articulation characterized by an incongruent articular surface that is highly variable in its morphology. The distal articular surface of the clavicle typically faces laterally, inferiorly, and slightly anteriorly, while the corresponding acromial facet faces medially, superiorly, and posteriorly. Interposed between these incongruent surfaces is a fibrocartilaginous intra-articular disc, or meniscus. This disc undergoes rapid, agerelated degenerative changes; by the fourth decade of life, it is almost universally fragmented or entirely absent, making the AC joint highly susceptible to primary osteoarthritis and post-traumatic osteolysis.
Stability of the AC joint is orchestrated by a highly synergistic network of static and dynamic stabilizers. The static stabilizers are conceptually divided into horizontal and vertical restraints. The acromioclavicular capsule and its intrinsic ligaments (superior, inferior, anterior, and posterior bundles) are the primary restraints to horizontal (anteroposterior) translation. Biomechanical studies have unequivocally demonstrated that the superior AC ligament is the most robust of these capsular thickenings, blending intimately with the overlying deltotrapezial fascia to resist posterior displacement of the distal clavicle. Surgical approaches that aggressively violate the superior capsule without meticulous plication invariably result in persistent horizontal instability, a common cause of postoperative pain and failure.
The primary vertical stabilizers are the coracoclavicular (CC) ligaments, which consist of two distinct fascicles: the conoid and the trapezoid. The conoid ligament is the more medial and posterior of the two, originating from the posteromedial base of the coracoid process and inserting onto the conoid tubercle of the clavicle. Its vertical orientation makes it the primary restraint to superior translation of the clavicle. The trapezoid ligament originates anterior and lateral to the conoid, fanning out in an oblique, horizontal trajectory to insert onto the trapezoid line of the inferior clavicle. This oblique orientation allows the trapezoid to act as the primary restraint to axial compression, preventing the acromion from being driven medially beneath the clavicle. During anatomical reconstruction, precise recreation of these distinct origins and insertions is a biomechanical imperative to restore normal coupled kinematics.
From a kinematic perspective, the clavicle is not a static strut; it is a highly dynamic bone that undergoes significant rotation during upper extremity elevation. As the arm is abducted or flexed, the scapula rotates upward, and the clavicle must concomitantly rotate posteriorly along its long axis by approximately 40 to 50 degrees. This obligatory rotation is facilitated by the unique, twisted orientation of the CC ligaments. Rigid surgical fixation across the coracoclavicular interval—such as the historical use of a static Bosworth screw—effectively eliminates this clavicular rotation. If such rigid hardware is not removed, it will inevitably restrict shoulder elevation and ultimately fail via fatigue breakage due to the immense repetitive forces generated during normal scapulothoracic rhythm.
Exhaustive Indications and Contraindications
The foundation of surgical decision-making for acromioclavicular joint pathology relies heavily on the Rockwood classification system, the chronicity of the injury, and the physiological demands of the patient. Low-grade injuries, encompassing Rockwood Grades I and II, represent sprains or partial tears of the AC ligaments with an entirely intact coracoclavicular complex. Acute management of these injuries is universally non-operative, focusing on brief immobilization, cryotherapy, and early functional rehabilitation. However, a distinct subset of these patients will develop chronic, recalcitrant pain secondary to post-traumatic osteolysis, meniscoid entrapment, or advanced degenerative joint disease. In these highly specific, chronic scenarios, an isolated resection of the distal clavicle (the Mumford or Gurd procedure) is strongly indicated.
High-grade injuries (Rockwood Grades III, IV, V, and VI) represent complete disruptions of both the AC and CC ligamentous complexes, resulting in gross macroscopic instability. Grade IV injuries (posterior displacement of the clavicle into or through the trapezius fascia), Grade V injuries (severe superior displacement greater than 100% to 300% of the contralateral side with massive fascial stripping), and the exceedingly rare Grade VI injuries (inferior subcoracoid dislocation) are absolute indications for surgical intervention. The management of acute Grade III injuries (100% superior displacement without massive fascial disruption) remains one of the most hotly debated topics in orthopedic surgery. Current consensus suggests non-operative management for the majority of Grade III injuries, reserving surgical reconstruction for elite overhead athletes, heavy manual laborers, or patients who fail a rigorous 3-to-6-month course of conservative therapy.
A critical surgical warning must be emphatically stated regarding the Mumford procedure: isolated resection of the distal clavicle is absolutely contraindicated in the setting of any high-grade (III-VI) AC joint injury, whether acute or chronic. Because the CC ligaments are incompetent in these grades, resecting the distal clavicle removes the only remaining point of bony contact between the clavicle and the scapula. This iatrogenic destabilization converts a partially constrained, albeit dislocated, clavicle into a hypermobile, free-floating strut that will relentlessly impinge upon the underlying neurovascular structures and periscapular musculature, leading to catastrophic functional outcomes.
To clearly delineate the complex decision-making matrix, the following table summarizes the precise indications and contraindications for the primary surgical interventions addressing AC joint pathology:
| Surgical Procedure | Primary Indications | Absolute Contraindications | Relative Contraindications |
|---|---|---|---|
| Isolated Distal Clavicle Resection (Mumford/Gurd) | Chronic, symptomatic Grade I/II injuries; Post-traumatic osteolysis; AC joint osteoarthritis. | Any Grade III, IV, V, or VI injury (incompetent CC ligaments); Acute Grade I/II injuries. | Poor deltotrapezial fascial integrity; Concomitant massive rotator cuff tear. |
| Dynamic Transfer (Weaver-Dunn Procedure) | Chronic Grade III, IV, or V dislocations; Salvage of failed primary repairs in lower-demand patients. | Acute injuries (where primary repair/healing is possible); Elite overhead athletes requiring maximum strength. | Previous acromioplasty (sacrificed CA ligament); Severe osteopenia of the distal clavicle. |
| Anatomic CC Ligament Reconstruction (Tendon Graft) | Chronic Grade III, IV, V dislocations in high-demand patients; Revision of failed Weaver-Dunn or suspensory fixation. | Active surgical site infection; Medically unfit for complex, prolonged surgery. | Insufficient coracoid bone stock (requires careful preoperative CT assessment). |
| Acute Suspensory Fixation (Cortical Buttons) | Acute (<3 weeks) Grade IV, V, VI injuries; Acute symptomatic Grade III in elite athletes/laborers. | Chronic injuries (>4-6 weeks) without biological augmentation; Active local infection. | Midshaft clavicle fractures on the ipsilateral side; Severe osteoporosis. |
Pre-Operative Planning, Templating, and Patient Positioning
Thorough preoperative planning begins with a meticulous clinical examination and a highly specific radiographic series. Clinically, the surgeon must assess for the presence of scapular dyskinesia, which is nearly universal in chronic high-grade dislocations. The "Paxinos sign" and cross-body adduction tests are vital for localizing pain specifically to the AC joint in low-grade or degenerative cases. In high-grade injuries, the skin overlying the prominent distal clavicle must be carefully inspected; impending skin necrosis or severe tenting in an acute Grade V injury elevates the urgency of surgical intervention to prevent a closed injury from converting into an open, contaminated joint space.
Standard radiographic evaluation must extend beyond routine shoulder views. The Zanca view is the absolute gold standard for visualizing the AC joint. It is obtained by directing the X-ray beam at a 10 to 15-degree cephalad tilt with the penetration voltage reduced by 50% compared to a standard AP shoulder radiograph. This specific projection removes the superimposition of the scapular spine, allowing for crystal-clear visualization of the articular margins and the degree of superior clavicular translation. An axillary lateral view is equally critical; it is the only reliable method to diagnose a Grade IV injury, demonstrating the posterior displacement of the clavicle through the trapezius muscle. Bilateral stress views, utilizing 10 to 15-pound weights suspended from the wrists, were historically popular but have largely been abandoned in modern practice due to patient discomfort and their limited impact on altering the surgical decision-making algorithm.
Anesthetic management typically involves a multimodal approach. General endotracheal anesthesia provides secure airway control and profound muscle relaxation, which is essential for reducing high-grade, chronically retracted dislocations. This is almost universally supplemented with an ultrasound-guided interscalene regional nerve block. The interscalene block provides exceptional intraoperative hemodynamics and dramatically reduces postoperative opioid consumption. However, the anesthesia team must be cautioned regarding the potential for transient phrenic nerve palsy, which may be poorly tolerated in patients with severe pre-existing pulmonary disease.
Patient positioning is critical for successful execution of both resection and reconstructive techniques. The patient is placed in the beach-chair position, with the torso elevated to approximately 45 to 60 degrees. The head must be meticulously secured in a neutral posture using a specialized headrest to prevent excessive cervical traction and subsequent brachial plexus neuropraxia. The operative arm is draped entirely free, utilizing a sterile hydraulic arm positioner if available. Draping the arm free is a non-negotiable requirement; it allows the surgeon to dynamically range the shoulder intraoperatively to assess for residual impingement following a Mumford resection, or to evaluate the tension and isometric properties of a coracoclavicular ligament reconstruction. A fluoroscopic C-arm must be brought in from the contralateral side to confirm hardware placement and the adequacy of the reduction before definitive closure.
Step-by-Step Surgical Approach and Fixation Technique
The Mumford/Gurd Procedure (Distal Clavicle Resection)
The open Mumford procedure remains the benchmark for addressing isolated AC joint pathology with intact coracoclavicular ligaments. A 3 to 4 cm incision is made centered directly over the AC joint, oriented in the sagittal plane following Langer's lines to optimize cosmetic healing. The deltotrapezial fascia is identified and incised in line with the clavicle. Meticulous subperiosteal dissection is utilized to expose the distal clavicle. The critical step is the bony resection: using a microsagittal saw, exactly 1.0 to 1.5 cm of the distal clavicle is resected.
A severe surgical pitfall involves over-resection. The trapezoid ligament inserts precisely 2.5 to 3.0 cm medial to the distal articular margin. Resecting 2.5 cm or more—as was historically advocated—carries a high risk of iatrogenically detaching the trapezoid ligament, catastrophically destabilizing the clavicle. Following resection, the superior and posterior cortices are aggressively rasped to prevent dermal irritation. The procedure concludes with a rigorous, watertight imbrication of the deltotrapezial fascia using heavy non-absorbable sutures, which acts as a dynamic checkrein against superior clavicular migration.
The Neviaser Technique and Historical Context
Historically, the Neviaser technique was utilized to address AC dislocations by transferring the coracoacromial (CA) ligament to the superior aspect of the clavicle to reconstruct the superior AC capsule.
While conceptually elegant in addressing horizontal instability, the Neviaser technique fails to reconstruct the vertical restraint normally provided by the conoid and trapezoid ligaments. Because the massive vertical forces of the upper extremity are not neutralized, the transferred CA ligament invariably stretches or ruptures, leading to recurrent dislocation. Consequently, this technique is now considered obsolete as an isolated procedure for high-grade injuries, though elements of capsular repair are still integrated into modern comprehensive reconstructions.
The Weaver-Dunn Procedure and Modifications
The Weaver-Dunn procedure shifted the reconstructive focus to the coracoclavicular interval. Through a saber incision extending from the clavicle to the coracoid process, the distal clavicle is resected (1.0 cm). The coracoacromial (CA) ligament is identified, meticulously dissected from its acromial attachment (often with a small osseous fleck to promote bone-to-bone healing), and mobilized. The medullary canal of the distal clavicle is prepared, and the CA ligament is drawn into the canal and secured with heavy transosseous sutures.
Because the native CA ligament possesses only 25% of the tensile strength of the native CC ligaments, it cannot withstand the deforming forces of the shoulder during the initial healing phase. Therefore, the Weaver-Dunn transfer must be protected by a static stabilizer. The Rockwood modification achieved this by utilizing a rigid Bosworth screw placed from the clavicle into the coracoid. While highly effective at maintaining reduction, the Bosworth screw eliminates physiologic clavicular rotation and mandates a secondary surgical procedure for hardware removal at 8 to 12 weeks to prevent fatigue fracture of the screw.
Modern Anatomic Coracoclavicular Reconstruction
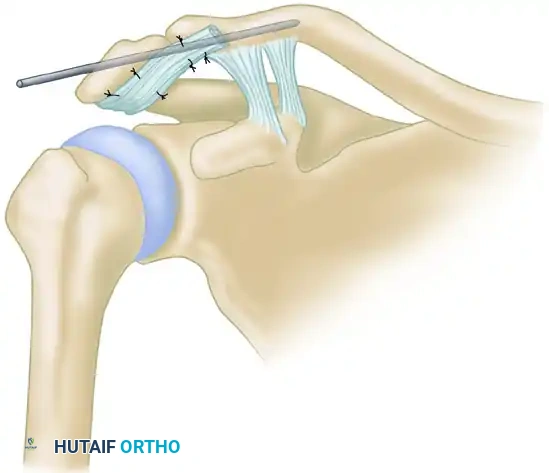
To overcome the biomechanical limitations of the CA ligament and the rigidity of metallic screws, modern surgery has evolved toward anatomic reconstruction using free tendon grafts (e.g., semitendinosus allograft or autograft) combined with cortical suspensory fixation (suture buttons).
In this technique, the coracoid base and the clavicle are exposed. A drill hole is placed perfectly centrally in the base of the coracoid. Two corresponding drill holes are placed in the clavicle: one medially and posteriorly (to recreate the conoid) and one laterally and anteriorly (to recreate the trapezoid). A suspensory suture button device is passed through the clavicular and coracoid tunnels to provide immediate, high-strength static reduction of the AC joint. Subsequently, the free tendon graft is passed beneath the coracoid and shuttled through the clavicular tunnels in a figure-of-eight or anatomic configuration. The graft is tensioned and secured with interference screws or heavy sutures while the clavicle is held in anatomic reduction. This modern construct provides immense immediate mechanical strength via the suture buttons, while the tendon graft provides a durable, biological, long-term reconstruction that permits physiologic rotation of the clavicle.
Complications, Incidence Rates, and Salvage Management
Despite significant advancements in surgical technique and biomechanical understanding, the surgical management of AC joint dislocations remains fraught with potential complications. The subcutaneous nature of the clavicle, the massive biomechanical forces acting upon the shoulder girdle, and the highly mobile nature of the scapulothoracic articulation create a challenging environment for both hardware maintenance and biological healing.
The most frequent and frustrating complication is the loss of radiographic reduction. While modern suspensory fixation devices possess high ultimate tensile strength, they are susceptible to "creep" and cyclical elongation. Furthermore, the cortical buttons can subside into the cancellous bone of the clavicle or coracoid, leading to a loss of tension. Minor losses of reduction (subluxation of 3 to 5 mm) are exceedingly common, occurring in up to 20-30% of cases, but are generally asymptomatic and do not require revision. Catastrophic loss of reduction, however, indicates a failure of the biological graft to incorporate or a complete pull-through of the hardware, necessitating complex revision surgery.
Hardware-specific complications are also notable. In historical techniques utilizing rigid metallic fixation (Bosworth screws or Kirschner wires), hardware migration and breakage were notorious. K-wires migrating into the thoracic cavity or mediastinum have been documented, making primary AC pinning an obsolete and dangerous practice. In modern suspensory fixation, the creation of multiple drill holes in the clavicle and coracoid introduces significant stress risers. Over-drilling the clavicle (e.g., using tunnels larger than 5.5 mm) dramatically increases the risk of postoperative clavicle fractures, which can occur even with minimal trauma during the rehabilitation phase.
| Complication | Estimated Incidence | Etiology / Risk Factors | Salvage / Management Strategy |
|---|---|---|---|
| Loss of Reduction (Recurrence) | 15% - 30% | Hardware creep; Button subsidence; Graft failure; Non-compliance with rehab. | Asymptomatic: Observe. Symptomatic: Revision reconstruction with allograft and secondary fixation. |
| Clavicle / Coracoid Fracture | 3% - 8% | Stress risers from large drill tunnels; Eccentric tunnel placement; Osteoporosis. | Open reduction internal fixation (ORIF) with locking plates; bypass the tunnels. |
| Superficial/Deep Infection | 2% - 5% | Subcutaneous hardware prominence; Bulky suture knots causing skin necrosis. | Superficial: Oral antibiotics. Deep: I&D, hardware removal (if healed) or retention with suppressive IV antibiotics. |
| Hardware Irritation/Pain | 10% - 20% | Prominent superior clavicular buttons or heavy suture knots under the skin. | Minor day-surgery procedure for hardware/knot removal after complete biological graft healing (>6 months). |
| Heterotopic Ossification (HO) | 30% - 40% | Subperiosteal dissection trauma; Bleeding in the CC interval. | Usually asymptomatic and requires no treatment. If impinging, surgical excision after maturation. |
Phased Post-Operative Rehabilitation Protocols
The postoperative rehabilitation following an acromioclavicular joint reconstruction is a delicate balancing act between protecting the biomechanical repair and preventing adhesive capsulitis of the glenohumeral joint. The overarching principle is that the mechanical hardware (suture buttons or screws) is merely a temporary internal splint; long-term success relies entirely on the biological incorporation and maturation of the tendon graft or ligament transfer.
Phase I: Maximum Protection (Weeks 0 to 4)
Immediately postoperatively, the patient is placed in a specialized shoulder immobilizer or a sling with an abduction pillow to offload the weight of the arm from the reconstructed CC interval. The primary goal during this phase is strict protection. Active shoulder elevation and heavy lifting are absolutely contraindicated. Rehabilitation is limited to active range of motion of the elbow, wrist, and hand to prevent distal stiffness. Passive glenohumeral range of motion is initiated but strictly limited to 90 degrees of forward flexion and 90 degrees of abduction to prevent excessive scapular rotation, which places immense strain on the healing coracoclavicular construct.
Phase II: Moderate Protection and Active-Assisted Motion (Weeks 4 to 8)
At four weeks, the sling is gradually weaned for activities of daily living, though it may still be worn in crowded environments for protection. The rehabilitation focus shifts to restoring full passive and active-assisted range of motion. Supine forward elevation using a wand or pulleys is highly effective. Submaximal, pain-free isometric strengthening of the deltoid and rotator cuff is initiated. However, the patient must be explicitly instructed to avoid any cross-body adduction or heavy lifting, as the biological graft is in the highly vulnerable "remodeling" phase where it is weakest.
Phase III: Active Motion and Early Strengthening (Weeks 8 to 12)
By the eighth postoperative week, the biological graft has achieved sufficient integration to withstand normal physiological loads. Full active range of motion in all planes is permitted and expected. The physical therapy regimen pivots toward isotonic strengthening of the periscapular stabilizers (rhomboids, trapezius, serratus anterior) to correct the scapular dyskinesia that almost universally accompanies chronic AC joint injuries. Closed kinetic chain exercises, such as wall push-ups, are introduced to enhance proprioception and dynamic stability.
Phase IV: Return to Sport and Heavy Labor (Months 3 to 6)
The final phase of rehabilitation focuses on sport-specific or occupation-specific functional training. Progression to heavy overhead lifting, contact sports, or manual labor is strictly delayed until at least 4 to 6 months postoperatively. Criteria for full clearance include painless, symmetric full range of motion, normal scapulothoracic rhythm, and isokinetic strength testing demonstrating at least 90% strength compared to the uninjured contralateral extremity. Premature return to contact sports is the leading cause of late traumatic graft rupture and must be rigorously avoided.
Summary of Landmark Literature and Clinical Guidelines
The evolution of surgical management for acromioclavicular joint dislocations is deeply rooted in several landmark biomechanical and clinical studies. The foundational work by Weaver and Dunn in 1972 revolutionized the treatment of chronic injuries by shifting the focus from the AC joint to the CC interval. However, subsequent biomechanical studies, most notably by Mazzocca et al., critically evaluated the Weaver-Dunn transfer, demonstrating that the transferred coracoacromial ligament provided less than 30% of the ultimate tensile strength and stiffness of the native intact CC ligaments. This biomechanical revelation was the catalyst for the development of modern anatomic reconstructions.
Further biomechanical investigations by Costic et al. and Grutter et al. established the superiority of free tendon grafts. These studies proved that an anatomic reconstruction utilizing a semitendinosus graft passed through independent clavicular and coracoid tunnels could closely replicate the native load-to-failure strength and stiffness of the intact conoid and trapezoid ligaments. This body of literature definitively established anatomic tendon reconstruction as the biomechanical gold standard for chronic, high-grade AC joint instability.
Clinically, the International Society of Arthroscopy, Knee Surgery and Orthopaedic Sports Medicine (ISAKOS) has provided consensus guidelines that heavily influence modern practice. The ISAKOS upper extremity committee emphasizes that while acute Rockwood Grade III injuries should generally be managed non-operatively, early surgical intervention may be justified in elite athletes or heavy laborers to prevent chronic dysfunction. For chronic Grade III, IV, and V injuries, the consensus strongly advocates for anatomic CC ligament reconstruction utilizing biological grafts augmented with suspensory cortical fixation, explicitly advising against the routine use of rigid metallic screws across the CC interval due to the high incidence of hardware failure and altered scapulothoracic kinematics.
In conclusion, the surgical management of AC joint dislocations demands a profound respect for the complex anatomy and biomechanics of the shoulder girdle. Surgeons must meticulously tailor their approach based on the chronicity and severity of the injury, utilizing time-tested resection techniques for isolated degenerative pathology, and reserving sophisticated, biologically augmented anatomic reconstructions for high-grade, destabilizing injuries. Strict adherence to these evidence-based principles, combined with flawless surgical execution and phased rehabilitation, is paramount to restoring optimal function and durability to the injured shoulder.
