Unraveling Pediatric Shoulder Fractures & Dislocations (Ages 0-18)
Key Takeaway
Learn more about Unraveling Pediatric Shoulder Fractures & Dislocations (Ages 0-18) and how to manage it. Proximal humerus fractures are breaks near the shoulder in children, representing less than 5% of pediatric fractures. They are common in adolescents and neonates (birth trauma). The physis, crucial for 80% of humeral growth, closes at specific ages to years: 14-17 for girls and 16-18 for boys, impacting remodeling potential.
Comprehensive Introduction and Patho-Epidemiology
Pediatric shoulder trauma encompasses a diverse array of injuries, with proximal humerus and clavicle fractures representing two of the most frequently encountered, yet fundamentally distinct, clinical entities in pediatric orthopedics. Understanding the patho-epidemiology of these injuries is paramount for the treating orthopedic surgeon, as the management algorithms are heavily dictated by the unique physiological and biomechanical properties of the immature skeleton. The intrinsic remodeling potential of the pediatric shoulder girdle often allows for non-operative management of deformities that would be strictly surgical in the adult population. However, the paradigm is shifting, particularly in the adolescent demographic, where the demand for early return to high-level athletics and the diminishing remodeling potential necessitate a more nuanced, and occasionally aggressive, surgical approach.
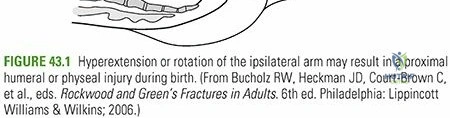
Proximal humerus fractures account for less than 5% of all pediatric fractures, with an estimated annual incidence ranging from 1.2 to 4.4 per 10,000 children. These injuries exhibit a bimodal distribution, presenting predominantly in neonates as a consequence of birth trauma, and subsequently in adolescents, driven by high-energy sports participation. In the neonatal cohort, birth trauma to the proximal humeral physis represents 1.9% to 6.7% of all physeal injuries. These are frequently associated with shoulder dystocia, breech presentations, and macrosomia, particularly in the setting of maternal gestational diabetes. The infant often presents with pseudoparalysis of the affected limb, necessitating a high index of suspicion and a thorough clinical evaluation to differentiate from brachial plexus palsy or septic arthritis.

In contrast to the proximal humerus, clavicle fractures are the most frequent long bone fractures sustained by children, constituting a staggering 8% to 15% of all pediatric fractures. The clavicle is also the most frequently fractured bone during parturition, occurring in 0.5% of normal cephalic deliveries and up to 1.6% of breech deliveries. In macrosomic infants weighing over 4,000 grams, the incidence of clavicular birth fractures skyrockets to approximately 13%. These obstetric fractures account for 84% to 92% of all birth-related skeletal trauma. The overwhelming majority of pediatric clavicle fractures (approximately 80%) occur in the midshaft region, typically just lateral to the insertion of the subclavius muscle, which acts as a crucial anatomical shield protecting the underlying brachial plexus and subclavian vessels from catastrophic injury.
The pathomechanics of these injuries vary significantly across age groups. Indirect trauma, such as a fall backward onto an outstretched hand (FOOSH) with the elbow extended and the wrist dorsiflexed, is a classic mechanism for proximal humerus fractures. Direct trauma to the posterolateral aspect of the shoulder is less common but can result in highly displaced or comminuted fracture patterns. Clavicle fractures, conversely, are most frequently the result of a direct blow to the lateral aspect of the shoulder, transmitting axial loads through the acromioclavicular joint into the S-shaped clavicular shaft. Understanding these mechanisms, coupled with the epidemiological data, provides the foundation for accurate diagnosis, appropriate imaging, and the formulation of an evidence-based treatment strategy.
Proximal Humerus Fractures
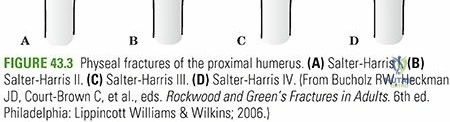
The epidemiology of proximal humerus fractures is heavily influenced by the skeletal maturity of the patient. In children under the age of five, these injuries are relatively rare outside of birth trauma, and when they do occur, they typically manifest as Salter-Harris Type I transphyseal fractures. As the child enters the pre-adolescent and adolescent years (ages 5 to 12 and beyond), the incidence rises sharply. This is largely attributable to the increased participation in contact sports and high-velocity activities such as skateboarding and cycling. In this older demographic, the fracture pattern shifts predominantly to Salter-Harris Type II injuries, where the metaphyseal bone, undergoing rapid remodeling and relative structural vulnerability, fails under sheer and bending forces.
The mechanism of injury in older children is almost exclusively traumatic. The classic presentation involves a fall from a height or a direct collision during athletic competition. The resulting force vector dictates the displacement of the fracture fragments. Because the proximal humeral physis is subjected to immense rotational and torsional forces, the fracture line often propagates through the hypertrophic zone of the physis before exiting through the metaphysis, creating the hallmark Thurston-Holland fragment. It is critical to recognize that the periosteal sleeve in children is robust and highly osteogenic; it often remains intact on one side (typically the posteromedial aspect), acting as a hinge that can both aid in closed reduction and prevent over-distraction.
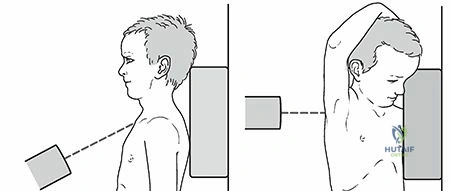
Diagnostic evaluation of the proximal humerus fracture requires a meticulous approach. The clinical presentation is typically unambiguous in older children, characterized by acute pain, swelling, ecchymosis, and a severely restricted range of motion. The patient will classically present supporting the injured extremity with the contralateral hand, holding the arm in internal rotation to minimize the painful tension exerted by the pectoralis major on the proximal shaft fragment. A palpable deformity may be appreciated anteriorly in the deltopectoral interval. However, in the neonate, the presentation is far more subtle. The infant will exhibit pseudoparalysis, holding the arm flaccidly in extension and internal rotation. The clinician must perform a rigorous differential diagnosis, ruling out concurrent brachial plexus birth palsy (Erb-Duchenne or Klumpke), clavicle fracture, and neonatal osteomyelitis or septic arthritis of the glenohumeral joint.
Clavicle Fractures
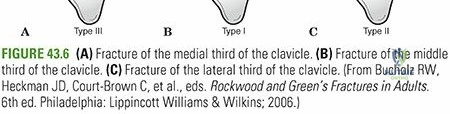
Clavicle fractures in the pediatric population are ubiquitous, yet they demand careful consideration due to their proximity to vital neurovascular structures. The anatomical distribution of these fractures is remarkably consistent: 80% occur in the middle third, 10% to 15% in the lateral third, and roughly 5% in the medial third. The middle third is anatomically predisposed to fracture because it represents the transition zone between the flattened lateral aspect and the tubular medial aspect, lacking the robust ligamentous support found at either end. Furthermore, the midshaft is the thinnest segment of the bone and is subjected to the highest bending moments during axial loading of the shoulder girdle.
Birth injuries to the clavicle are a frequent complication of difficult deliveries. They occur when the anterior shoulder becomes impacted behind the maternal symphysis pubis (shoulder dystocia), necessitating obstetric maneuvers that apply direct, forceful pressure to the fetal clavicle. Alternatively, the fracture may occur as the shoulders are delivered through a contracted pelvis. Clinically, the neonate may present with an asymmetric Moro reflex, crepitus upon palpation of the clavicle, and a visible or palpable mass representing early callus formation if the diagnosis is delayed. It is imperative to differentiate a missed clavicle fracture from congenital muscular torticollis, as an infant with a healing clavicle fracture will frequently tilt their head toward the affected side to relax the sternocleidomastoid muscle and alleviate tension on the fracture site.
In the older child and adolescent, clavicle fractures are typically the result of a direct blow to the point of the shoulder, such as a fall onto the lateral aspect of the acromion during a sporting event. This mechanism drives the scapula and lateral clavicle medially and inferiorly, while the medial clavicle is held in place by the strong sternoclavicular ligaments and the pull of the sternocleidomastoid muscle. The resulting shear force causes the midshaft to fail. Clinical evaluation reveals a gross deformity, localized tenderness, and often tenting of the overlying skin. While open fractures are exceedingly rare, the surgeon must remain vigilant for signs of neurovascular compromise or pleural injury, particularly in high-energy trauma or severely displaced midshaft fractures.
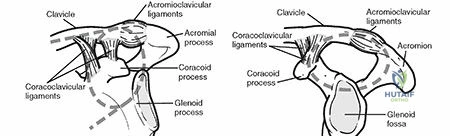
Detailed Surgical Anatomy and Biomechanics
A profound mastery of the surgical anatomy and biomechanics of the pediatric shoulder is the absolute prerequisite for both conservative and operative management. The proximal humerus and the clavicle exhibit unique developmental trajectories, ossification patterns, and vascular networks that directly influence their healing capacity and susceptibility to specific complications. The orthopedic surgeon must conceptualize these structures not merely as static bones, but as dynamic, growing organs subjected to complex, multi-directional muscular forces. The immense remodeling potential of the pediatric shoulder is a direct function of its robust physeal activity and thick, highly vascularized periosteum, which dictates the often-forgiving nature of these injuries.

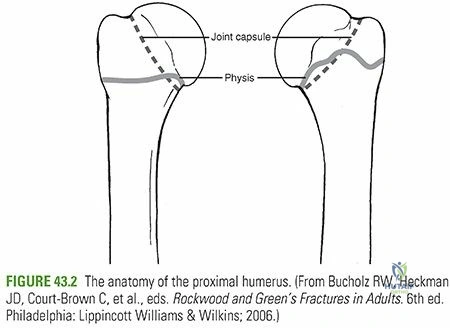
The proximal humerus is the primary engine of longitudinal growth for the upper extremity. Astonishingly, 80% of the entire humeral length is generated at the proximal physis. This extraordinary growth velocity endows the proximal humerus with an unparalleled capacity for spontaneous remodeling, allowing for the acceptance of significant angular and translational deformities in the younger child. The proximal humerus develops from three distinct secondary centers of ossification. The primary center for the humeral head ossifies at approximately 6 months of age. This is followed by the ossification of the greater tuberosity between 1 and 3 years of age, and finally, the lesser tuberosity between 4 and 5 years of age. These tuberosities coalesce into a single epiphysis around 6 to 7 years of age, which subsequently fuses with the humeral shaft between the ages of 7 and 13. The proximal physis itself does not completely close until 14 to 17 years in females and 16 to 18 years in males.
The biomechanical environment of the proximal humerus is defined by the antagonistic pull of powerful muscle groups. When a fracture occurs through the physis or proximal metaphysis, these muscular forces dictate the characteristic displacement pattern. The proximal epiphyseal fragment is subjected to the unopposed pull of the rotator cuff. The supraspinatus, infraspinatus, and teres minor (attaching to the greater tuberosity) abduct and externally rotate the proximal fragment, while the subscapularis (attaching to the lesser tuberosity) provides some internal rotation stabilization. Conversely, the distal metaphyseal/diaphyseal fragment is forcefully pulled medially and anteriorly by the pectoralis major, and superiorly by the deltoid and biceps brachii. This results in the classic apex-anterior and varus deformity seen in displaced proximal humerus fractures.
The vascular anatomy of the proximal humerus is of paramount importance, particularly when considering surgical approaches and the risk of osteonecrosis. The primary blood supply to the humeral head is derived from the anterolateral ascending branch of the anterior humeral circumflex artery. This vessel courses superiorly along the lateral aspect of the bicipital groove and penetrates the humeral head at the junction of the articular cartilage and the greater tuberosity. A smaller, supplementary blood supply to the inferior aspect of the humeral head and the greater tuberosity is provided by branches of the posterior humeral circumflex artery. Disruption of this delicate vascular network, particularly the anterior circumflex artery in cases of severe fracture-dislocations or aggressive open surgical dissection, can lead to devastating avascular necrosis (AVN) of the capital epiphysis.
Clavicular Development and Kinematics
The clavicle holds the unique distinction of being the first bone in the human body to begin the process of ossification, initiating via intramembranous ossification during the fifth week of fetal development. Unlike the long bones of the appendicular skeleton, the clavicle lacks a medullary cavity in its early developmental stages. Following the initial intramembranous phase, secondary centers of ossification develop via endochondral ossification at both the medial and lateral ends. The medial epiphysis is particularly critical, as it is responsible for approximately 80% of the longitudinal growth of the clavicle. This medial ossification center is the last in the body to fuse, typically appearing radiographically between the ages of 12 and 19 years and not completely fusing to the shaft until 22 to 25 years of age.
The kinematics of the clavicle are complex and essential for normal shoulder girdle function. During full shoulder elevation and abduction, the clavicle must rotate posteriorly along its longitudinal axis by approximately 50 degrees. This rotation is coupled with 30 degrees of superior elevation and up to 35 degrees of anterior-posterior excursion during scapular protraction and retraction. A malunited clavicle fracture, particularly one with significant shortening or angular deformity, can theoretically alter these kinematics, leading to scapular dyskinesia, loss of terminal shoulder abduction, and altered mechanics of the acromioclavicular and sternoclavicular joints. However, clinical studies have repeatedly demonstrated that the pediatric clavicle possesses an immense capacity to remodel, and functional deficits following non-operative management are exceedingly rare.
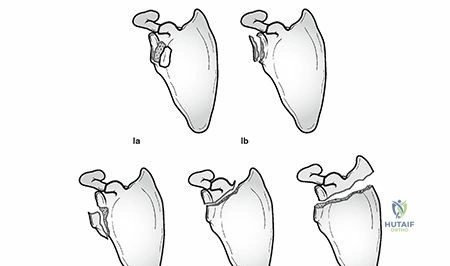
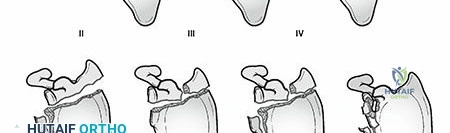
The periosteal sleeve of the pediatric clavicle is remarkably thick and resilient. In the event of a fracture, the bone often displaces within this intact periosteal tube. Even in completely displaced fractures, the inferior periosteum frequently remains in continuity, acting as a biological tether and a scaffold for rapid callus formation. This intact periosteal sleeve is the primary reason why nonunion of the pediatric clavicle is virtually non-existent, and why remodeling is so predictable. When evaluating medial clavicle injuries, what appears radiographically as a sternoclavicular joint dislocation is almost always a Salter-Harris Type I or II fracture through the medial physis, with the epiphysis remaining anatomically reduced within the sternoclavicular ligaments while the metaphyseal shaft displaces posteriorly or anteriorly.
Exhaustive Indications and Contraindications
The decision-making process regarding the management of pediatric shoulder fractures requires a delicate balance between accepting radiographic deformity and mitigating the risks associated with surgical intervention. The overarching principle in pediatric orthopedics—that younger patients possess greater remodeling potential—is nowhere more applicable than in the proximal humerus and clavicle. Consequently, the vast majority of these injuries are treated non-operatively with excellent functional outcomes. However, the surgeon must be acutely aware of the specific indications for operative fixation, which are primarily dictated by the patient's age, the degree of displacement, the stability of the reduction, and the presence of associated neurovascular or soft-tissue injuries.
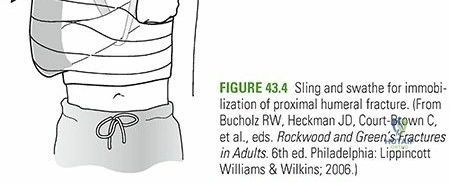
Non-operative management is the absolute gold standard for proximal humerus fractures in children under the age of ten, and for nearly all pediatric clavicle fractures regardless of age. In the proximal humerus, the acceptable parameters for deformity are incredibly generous due to the multi-planar motion of the glenohumeral joint and the massive growth potential of the proximal physis. For children aged 1 to 4 years, virtually any degree of angulation and up to 100% displacement is acceptable, as complete remodeling is anticipated. In children aged 5 to 12 years, up to 40 to 50 degrees of angulation and 50% translation of the shaft are routinely accepted. For these younger cohorts, treatment consists of a brief period of immobilization in a sling and swathe, or occasionally a shoulder spica cast for highly unstable patterns, followed by early passive and active range of motion.
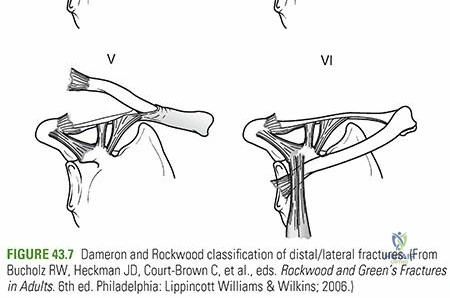
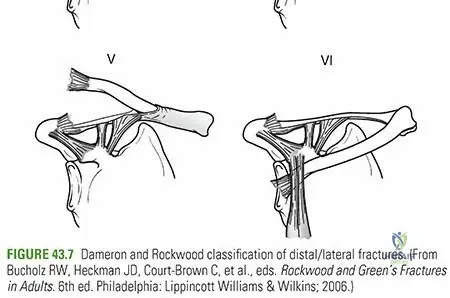
Operative intervention becomes a critical consideration in the adolescent population (ages 12 to maturity), where the remaining growth potential is insufficient to remodel severe deformities. In this age group, acceptable deformity parameters stricture significantly: angulation greater than 15 to 20 degrees or displacement exceeding 30% of the shaft width (Neer-Horowitz Grade III or IV) often warrants surgical stabilization to prevent long-term functional deficits, particularly in overhead athletes. Absolute indications for open reduction and internal fixation (ORIF) across all age groups include open fractures, fractures complicated by acute neurovascular compromise (e.g., axillary nerve or brachial plexus injury that does not resolve with reduction), and irreducible fractures where soft tissue—most commonly the long head of the biceps tendon, the periosteum, or the deltoid muscle—becomes interposed within the fracture site.
Contraindications to surgery are equally important to recognize. Operative intervention is strictly contraindicated in the presence of active local or systemic infection, severe medical comorbidities precluding safe anesthesia, or in cases of undisplaced or minimally displaced fractures where the risks of surgery (infection, iatrogenic nerve injury, physeal arrest, and avascular necrosis) far outweigh the potential benefits. Furthermore, surgical fixation of clavicle fractures in the pre-adolescent child is almost universally contraindicated, as the cosmetic bump of the callus will reliably remodel, and the risk of creating a nonunion or injuring the underlying subclavian vessels during exposure is an unacceptable hazard for an injury that reliably heals with conservative care.
Operative Management Criteria Table
| Patient Age Group | Injury Type | Acceptable Deformity (Non-Op) | Indications for Operative Fixation |
|---|---|---|---|
| Neonates (0-1 yr) | Proximal Humerus (SH I) | Up to 70° angulation, 100% displacement | Open fracture, vascular compromise (exceedingly rare) |
| Children (1-4 yrs) | Proximal Humerus (SH I/II) | Up to 50° angulation, 100% displacement | Irreducible with soft tissue interposition, open fracture |
| Children (5-12 yrs) | Proximal Humerus (SH II) | Up to 40-50° angulation, 50% translation | Open fracture, polytrauma, floating shoulder, neurovascular injury |
| Adolescents (12-18 yrs) | Proximal Humerus (SH II/III/IV) | < 20° angulation, < 30% translation (Neer-Horowitz I/II) | Neer-Horowitz III/IV, irreducible, intra-articular extension (SH III/IV), high-demand athlete |
| All Ages | Clavicle (Midshaft) | 100% displacement, significant shortening | Open fracture, skin tenting with impending necrosis, subclavian vessel injury, severe polytrauma |
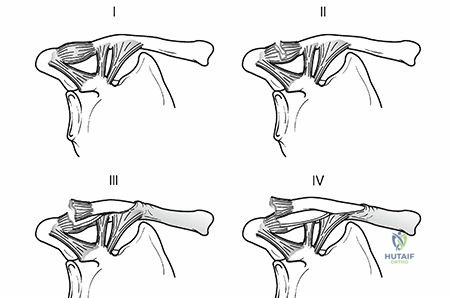
| All Ages | Medial Clavicle / SC Joint | Complete posterior displacement (if asymptomatic) | Posterior displacement causing tracheal, esophageal, or great vessel compression |
Pre-Operative Planning, Templating, and Patient Positioning
Thorough pre-operative planning is the cornerstone of successful surgical execution in pediatric orthopedic trauma. The surgeon must synthesize clinical findings, advanced imaging, and a deep understanding of classification systems to formulate a cohesive surgical strategy. This strategy must account for the specific fracture morphology, the presence of physeal involvement, the anticipated difficulty of reduction, and the optimal trajectory for fixation implants. Templating, while traditionally associated with arthroplasty, is equally critical in trauma to determine the appropriate length and diameter of Kirschner wires, Steinmann pins, or, in rare adolescent cases, locking plates. The goal is to achieve stable fixation that respects the delicate physeal anatomy and minimizes iatrogenic trauma.
Radiographic evaluation must be exhaustive. For the proximal humerus, a standard trauma series is mandatory, comprising a true anteroposterior (AP) view (Grashey view), a lateral view in the plane of the scapula (Scapular "Y" view), and an axillary lateral view. The axillary view is non-negotiable, as it is the most reliable method for assessing the degree of anterior or posterior translation, identifying associated glenohumeral dislocations, and evaluating the articular surface of the humeral head. In the uncooperative or severely injured child, a Velpeau axillary view can be obtained without removing the arm from the sling. For neonatal injuries where
Clinical & Radiographic Imaging Archive