Operative Management of Pediatric Pathological and Non-Accidental Fractures

Key Takeaway
Pediatric pathological fractures and non-accidental trauma require specialized orthopedic management. While conservative treatment remains common, operative intervention is increasingly indicated to minimize immobilization-induced osteopenia and morbidity. This guide details the biomechanical principles, surgical indications, and operative techniques for managing pediatric pathological fractures, including osteogenesis imperfecta, bone cysts, and child abuse injuries, emphasizing physeal preservation and anatomical reduction.
Comprehensive Introduction and Patho-Epidemiology
Historically, the vast majority of pediatric fractures, encompassing both traumatic and pathological variants, were managed almost exclusively non-operatively through closed reduction and cast immobilization. The inherent remodeling potential of the immature skeleton, coupled with historical risks associated with pediatric anesthesia and surgical site infections, strongly favored conservative paradigms. However, as anesthetic techniques have advanced, implant technologies have evolved, and the understanding of pediatric bone biomechanics has deepened, this paradigm has precipitously shifted. Today, an increasing number of pathological fractures and complex injuries in children are treated operatively. This proactive, surgically assertive approach significantly decreases morbidity, facilitates rapid nursing care, and minimizes the profoundly deleterious systemic effects of prolonged immobilization.
The patho-epidemiology of pediatric pathological fractures is diverse, broadly categorized into localized benign neoplastic processes and systemic metabolic or genetic dysplasias. Localized lesions, such as Unicameral Bone Cysts (UBC), Aneurysmal Bone Cysts (ABC), and Non-Ossifying Fibromas (NOF), frequently present as impending or completed fractures following trivial trauma. These lesions create significant stress risers within the metaphyseal or diaphyseal bone, compromising the structural integrity of the cortex. Conversely, systemic conditions such as Osteogenesis Imperfecta (OI), osteopetrosis, and severe rickets present with generalized osteopenia or altered material properties of the bone, leading to a recurrent fracture diathesis. Children with these underlying metabolic or genetic bone disorders must not be subjected to extended periods of cast immobilization. The absence of mechanical loading rapidly exacerbates disuse osteopenia, creating a vicious, self-perpetuating cycle of recurrent fractures, progressive deformity, and functional decline.
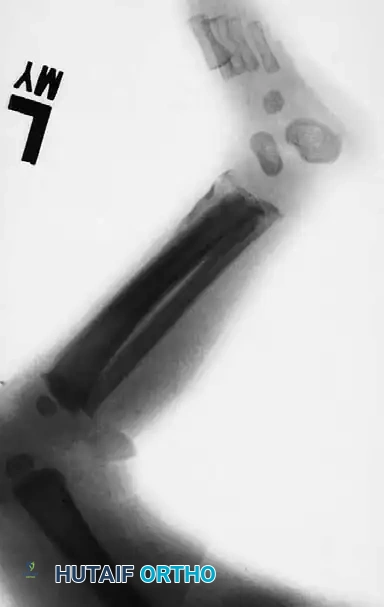
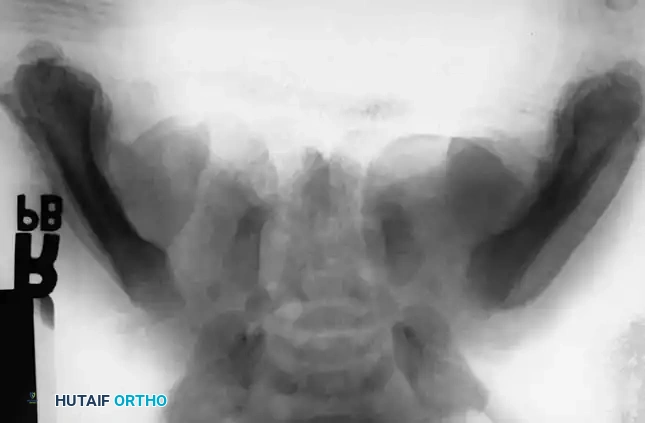
Parallel to pathological fractures, Non-Accidental Trauma (NAT), or child abuse, represents a critical epidemiological and diagnostic challenge. The highest incidence of NAT occurs in vulnerable populations, specifically infants and toddlers between birth and two years of age. The pathophysiology of these fractures often involves violent torsional, shearing, or direct compressive forces that far exceed the physiological thresholds of infant bone, resulting in highly specific fracture patterns. The orthopedic surgeon is frequently the first physician to evaluate these patients, bearing a profound medicolegal and ethical responsibility to recognize the pathognomonic signs of abuse, initiate appropriate diagnostic workups, and ensure the immediate safety of the child.

The convergence of pathological and NAT fracture management requires the orthopedic surgeon to operate at the highest level of clinical acumen. In both scenarios, the fracture is merely the mechanical manifestation of a severe underlying systemic, genetic, or psychosocial pathology. The operative intervention must be meticulously planned not only to restore anatomical alignment and biomechanical stability but also to integrate seamlessly into a broader, multidisciplinary treatment strategy encompassing endocrinology, oncology, pediatrics, and child protective services.
Detailed Surgical Anatomy and Biomechanics
A profound, granular understanding of longitudinal bone growth and pediatric surgical anatomy is mandatory when planning operative interventions in children. The remodeling potential of a pediatric fracture is not absolute; it is directly proportional to the chronological and skeletal age of the child, the distance of the fracture from the most active physis, and the plane of the deformity. The physis is a highly complex, dynamic cartilaginous structure, not merely a flat plate. It is highly undulated, featuring complex mammillary processes that interlock with the metaphyseal bone to provide intrinsic shear stability. Furthermore, the perichondrial ring (Zone of Ranvier) at the periphery is critical for latitudinal growth and must be meticulously protected during surgical exposures.
The growth contributions of the upper and lower extremity physes dictate the remodeling potential and influence the timing and technique of surgical intervention. In the upper extremity, the proximal humerus and the distal radius/ulna are the primary engines of longitudinal growth. Specifically, approximately 80% of the longitudinal growth of the humerus occurs at the proximal physis, while only 20% occurs at the distal physis. In the forearm, the proximal radius contributes 25%, whereas the distal physis is responsible for 75% of the bone's length. Similarly, the proximal ulna contributes 15%, and the distal physis contributes 85%. Consequently, fractures near these highly active physes possess massive remodeling potential in the sagittal and coronal planes. In the lower extremity, the distal femur (70%) and proximal tibia (55%) are the dominant growth centers.
Biomechanically, pathological bone behaves fundamentally differently than healthy pediatric bone. In conditions like Osteogenesis Imperfecta, the type I collagen defect leads to a significantly altered modulus of elasticity; the bone is brittle, poorly organized, and lacks the normal plastic deformation phase characteristic of pediatric bone. This necessitates fixation constructs that span the entire length of the bone to prevent peri-implant fractures at stress risers. In the presence of cystic lesions (UBC/ABC), the normal cylindrical mechanics of the diaphysis are compromised. The cyst acts as a massive stress riser, reducing the polar moment of inertia and dramatically lowering the threshold for torsional failure.
When addressing deformities, surgeons must adhere to the biomechanical reality that while sagittal and coronal plane deformities near active physes remodel predictably, rotational deformities do not. A malrotation of the femur or tibia will persist into adulthood, altering joint kinematics and predisposing the patient to early-onset osteoarthritis. Therefore, precise anatomical correction of rotational alignment is a non-negotiable surgical objective, regardless of the patient's age or the underlying pathology. Furthermore, intra-articular step-offs possess zero remodeling potential and demand absolute anatomical reduction to prevent post-traumatic arthrosis.
Exhaustive Indications and Contraindications
The decision to proceed with operative intervention in pediatric pathological and NAT fractures is nuanced, requiring a careful risk-benefit analysis tailored to the specific pathology, the patient's physiological reserve, and the psychosocial environment. Operative management is strongly indicated in several specific pathological entities where conservative management has a predictably high failure rate or leads to unacceptable morbidity. In Osteogenesis Imperfecta (OI), patients suffer from profound osteopenia, recurrent fractures, and progressive bowing deformities. Operative intervention, typically utilizing telescoping intramedullary rods (e.g., Fassier-Duval nails), is indicated to prevent progressive diaphyseal deformity, splint the fragile bone, and allow for early, upright mobilization.
Large cystic defects, particularly those occupying greater than 50% of the cortical diameter or those that have failed conservative management (such as repeated corticosteroid or bone marrow aspirate injections), require surgical intervention. Fractures through these benign bone tumors often necessitate surgical curettage, adjuvant chemical or thermal treatment of the cavity, bone grafting (autograft, allograft, or synthetic calcium phosphate substitutes), and internal fixation to ensure immediate structural stability and prevent recurrence. In Neurofibromatosis Type 1 (NF1), congenital anterolateral bowing of the tibia progressing to pseudarthrosis is a hallmark indication for aggressive surgery. These complex non-unions are notoriously recalcitrant to standard fixation and require radical resection of the hamartomatous periosteal tissue, robust bone grafting, and rigid internal or external fixation.

In the context of Non-Accidental Trauma, the indications for surgery are dual-purposed. While many infant fractures could biomechanically heal with casting, admission for surgical management or rigorous clinical observation provides optimal orthopedic care while simultaneously sheltering the abused child from their abusers until child protective services can intervene. Polytraumatized children, or those with severe Traumatic Brain Injury (TBI) and spasticity, also require early operative stabilization. In these patients, conservative management is impeded by severe muscle spasms, the need for intensive care access, and the necessity of upright positioning for pulmonary toilet.
| Parameter | Absolute Indications | Relative Indications | Contraindications |
|---|---|---|---|
| Metabolic/Genetic (e.g., OI) | Progressive diaphyseal bowing > 40 degrees; Recurrent fractures in the same bone. | Inability to ambulate due to bone fragility; Painful microfractures. | Active systemic infection; Extreme cardiopulmonary instability precluding anesthesia. |
| Benign Cystic Lesions (UBC/ABC) | Weight-bearing bone fracture with >50% cortical destruction; Imminent risk of femoral neck fracture. | Upper extremity cysts failing 2+ injection therapies; Painful impending fractures. | Asymptomatic, resolving cysts in non-weight-bearing bones; Lesions immediately adjacent to an open physis (relative). |
| Non-Accidental Trauma (NAT) | Displaced intra-articular fractures; Femur fractures in children requiring CPS sheltering. | Unstable diaphyseal fractures precluding safe nursing care. | Medically unstable polytrauma (damage control orthopedics preferred); Undiagnosed bleeding diathesis. |
| Neurofibromatosis (NF1) | Established congenital pseudarthrosis of the tibia (CPT). | Progressive anterolateral bowing prior to fracture. | Poor soft tissue envelope precluding rigid fixation (requires soft tissue optimization first). |
Pre-Operative Planning, Templating, and Patient Positioning
Meticulous pre-operative planning is the cornerstone of successful surgical outcomes in pediatric pathological fractures. The planning phase begins with comprehensive, high-quality orthogonal imaging. For cystic lesions, plain radiographs must be supplemented with advanced imaging. Computed Tomography (CT) is invaluable for assessing cortical thickness and determining the exact volume of the defect for bone graft quantification. Magnetic Resonance Imaging (MRI) is critical for delineating soft tissue extension, identifying fluid-fluid levels characteristic of Aneurysmal Bone Cysts, and ruling out malignant transformation or more aggressive pathologies such as telangiectatic osteosarcoma.
In cases of profound deformity, such as the severe anterolateral bowing seen in Osteogenesis Imperfecta, standard templating is often insufficient. Surgeons must utilize digital templating software or 3D-printed models to plan multi-apical corrective osteotomies (the Sofield-Millar technique). The surgeon must calculate the exact wedge resections required to straighten the bone sufficiently to allow passage of a straight, telescoping intramedullary nail. The diameter of the medullary canal in OI patients is often critically narrow, necessitating the availability of ultra-small diameter reamers and a wide array of implant sizes. Pre-operative planning must also account for the altered bone quality; standard cortical screws may have poor purchase, requiring the use of locking plates or intramedullary load-sharing devices.
Patient positioning is dictated by the specific fracture and the planned surgical approach, but universally requires a radiolucent operating table to facilitate unimpeded fluoroscopic visualization in multiple orthogonal planes. For lower extremity intramedullary nailing, the patient is typically positioned supine on a flat radiolucent table with a bump under the ipsilateral hip to correct external rotation. The C-arm must be positioned to allow full visualization from the hip to the ankle without moving the patient. In pediatric patients, core temperature regulation is critical; forced-air warming blankets and warmed intravenous fluids must be utilized to prevent intraoperative hypothermia, which can exacerbate coagulopathy and increase surgical site infection rates.
Furthermore, pre-operative planning for these complex cases demands rigorous multidisciplinary coordination. The anesthesia team must be briefed on the patient's specific pathology—for instance, patients with OI frequently have basilar invagination, fragile teeth, and restrictive lung disease, making intubation hazardous. In cases of NAT, the surgical team must coordinate with pediatricians, social workers, and law enforcement to ensure that all forensic evidence (e.g., skeletal surveys, clinical photographs) is properly documented and that a secure chain of custody is maintained for any legal proceedings.
Step-by-Step Surgical Approach and Fixation Technique
The surgical execution of pediatric pathological fracture repair demands adherence to strict, pediatric-specific principles. The overarching goal is to achieve adequate stability to allow for early mobilization while meticulously preserving the delicate physeal anatomy and minimizing periosteal stripping. When operative intervention is deemed necessary, the surgeon must balance the need for anatomical reduction with the biological cost of the surgical approach.
Management of Osteogenesis Imperfecta (The Sofield-Millar Technique)
The gold standard for managing severe diaphyseal deformity and recurrent fractures in OI is the Sofield-Millar fragmentation and realignment technique, combined with telescoping intramedullary nailing (e.g., Fassier-Duval). The approach involves a longitudinal incision over the diaphysis, carefully elevating the periosteum. The deformed bone is exposed, and multiple transverse osteotomies are performed at the apices of the deformities. The bone segments are then "shish-kebabbed" onto the intramedullary nail. The male component of the telescoping nail is anchored in the distal epiphysis, while the female component is anchored in the proximal epiphysis. As the child grows, the nail telescopes, providing continuous internal splinting of the diaphysis and preventing recurrent bowing. Extreme care must be taken during reaming, as the cortices are eggshell-thin and easily perforated.
Curettage and Grafting of Cystic Lesions
For fractures through benign cysts (UBC/ABC), the surgical approach is dictated by the location of the lesion. A cortical window is created over the cyst, large enough to allow thorough intralesional curettage. The cavity must be aggressively debrided using high-speed burrs to remove the membranous cyst lining entirely. For ABCs, adjuvant therapy with argon beam coagulation, phenol, or cryotherapy is often employed to reduce the high recurrence rate. The void is then packed tightly with bone graft. In structural areas like the proximal femur, autologous iliac crest bone graft combined with rigid internal fixation (e.g., a pediatric dynamic hip screw or locking plate) is mandatory to prevent catastrophic varus collapse or femoral neck fracture during the incorporation phase.
Principles of Physeal Protection
When operating near a physis, anatomical reduction is mandatory. If an open reduction is necessary for a physeal injury (e.g., Salter-Harris III or IV), the cartilaginous fragments must be repositioned perfectly to prevent the formation of a transphyseal bony bridge (bar). The surgeon must strictly utilize smooth Kirschner wires (K-wires) or Steinmann pins rather than threaded pins when crossing the physis. Threaded pins cause significant mechanical damage to the resting zone of the physeal cartilage upon insertion and removal, drastically increasing the risk of premature physeal closure. Whenever biomechanically feasible, the trajectory of fixation should parallel the physis entirely within the epiphysis, or be confined strictly to the metaphysis.
Stabilization in Non-Accidental Trauma
In NAT, diaphyseal fractures of the femur or tibia are frequently encountered. Elastic Stable Intramedullary Nailing (ESIN) is the workhorse for these injuries in children aged 5 to 11 years. Two titanium elastic nails are inserted in a retrograde or antegrade fashion, pre-bent to create a symmetrical three-point fixation construct within the medullary canal. This minimally invasive technique provides excellent rotational and axial stability while preserving the fracture hematoma and periosteal blood supply, leading to rapid, robust callus formation. In infants and toddlers (the primary demographic for NAT), spica casting remains the standard of care for femur fractures, though flexible nailing may be considered in cases of severe polytrauma or when social circumstances demand immediate rigid stabilization.
Complications, Incidence Rates, and Salvage Management
The operative management of pediatric pathological fractures is fraught with potential complications, ranging from hardware failure in osteopenic bone to catastrophic physeal growth arrest. The surgeon must proactively anticipate these complications, employing meticulous surgical technique and vigilant postoperative monitoring to mitigate risks. Comprehensive parental counseling is paramount; a parent informed preoperatively regarding the high risk of complications in pathological bone is an ally, whereas a parent informed postoperatively is often an adversary.
One of the most devastating complications is iatrogenic physeal arrest, leading to progressive angular deformity and limb length discrepancy. This occurs when hardware violates the physis or when the initial trauma crushes the highly sensitive reserve zone of the growth plate. If a physeal bar forms and occupies less than 50% of the cross-sectional area of the physis, salvage management involves surgical excision of the bony bar and interposition of a biologically inert material (e.g., fat graft or cranioplast) to prevent recurrence. If the bar is larger, contralateral epiphysiodesis or formal limb lengthening procedures (e.g., Ilizarov or Taylor Spatial Frame) may be required.
Hardware migration and failure are exceptionally common in Osteogenesis Imperfecta due to the poor bone stock. Telescoping nails may fail to expand, leading to proximal or distal migration through the epiphysis and into the joint space. This intra-articular pin penetration leads to rapid chondrolysis and severe early-onset osteoarthritis. Salvage requires immediate hardware removal, joint lavage, and revision fixation, often necessitating a larger diameter nail or supplemental plate fixation.
Compartment syndrome is a surgical emergency that requires hyper-vigilant monitoring, particularly following stabilization of tibial fractures or supracondylar humerus fractures. Pediatric patients are highly susceptible, and classic signs like paresthesia or pulselessness are late and unreliable. Increasing analgesic requirements in a previously comfortable child is the earliest and most reliable sign. Immediate four-compartment fasciotomy is the only definitive salvage.
| Complication | Estimated Incidence | Primary Etiology | Salvage Management |
|---|---|---|---|
| Physeal Arrest / Bony Bar | 5% - 15% (varies by SH type) | Trauma to the zone of Ranvier; Threaded pins crossing physis. | Bar excision and fat interposition (<50% area); Contralateral epiphysiodesis. |
| Hardware Migration (OI) | 20% - 30% | Failure of telescoping mechanism; Poor epiphyseal bone stock. | Immediate implant removal; Revision with larger diameter or alternative design nail. |
| Non-union / Pseudarthrosis | High in NF1 (>40%) | Hamartomatous periosteal tissue; Inadequate resection. | Radical resection, massive autografting, rigid circular external fixation (Ilizarov). |
| Compartment Syndrome | 1% - 3% (Tibial shaft) | Acute swelling within tight fascial compartments; Reperfusion injury. | Emergent four-compartment fasciotomy; Delayed primary closure or skin grafting. |
| Cyst Recurrence (UBC/ABC) | 15% - 25% | Incomplete curettage of the cyst membrane. | Repeat aggressive curettage; Adjuvant argon beam coagulation; Repeat bone grafting. |
Phased Post-Operative Rehabilitation Protocols
The postoperative management of pediatric pathological and non-accidental fractures requires a highly structured, multidisciplinary approach that extends far beyond the operating room. The rehabilitation protocol must be phased, dynamically adjusting to the biological healing of the fracture, the stability of the surgical construct, and the underlying systemic pathology.
Phase I: Acute Post-Operative Phase (Weeks 0-3)
The primary objectives during the acute phase are pain control, edema management, and protection of the surgical fixation. Depending on the rigidity of the internal fixation, supplemental casting is often utilized. For example, following curettage and grafting of a proximal femur cyst, a one-and-a-half spica cast may be applied to neutralize massive deforming muscle forces. Strict non-weight-bearing status is typically enforced. Vigilant neurovascular monitoring is paramount during the first 48 hours to detect impending compartment syndrome. In cases of NAT, this phase is critical for social services; the child must remain admitted until a formal, legally binding safety plan is established by child protective services and the hospital's child abuse pediatrics team.
Phase II: Subacute Healing and Early Mobilization (Weeks 3-6)
As the soft tissues heal and early soft callus forms, the focus shifts to restoring joint mobility. In cases of flexible intramedullary nailing (ESIN) for diaphyseal fractures, early mobilization of adjacent joints is permitted if the construct is rotationally stable. Physical therapy is initiated, focusing on passive and active-assisted range of motion to prevent arthrofibrosis, particularly in the knee and elbow. For pathological fractures related to metabolic bone disease (e.g., OI), this phase involves intensive coordination with pediatric endocrinology. The initiation or resumption of intravenous bisphosphonate therapy (e.g., pamidronate or zoledronic acid) is crucial to increase bone mineral density, optimize graft incorporation, and reduce future fracture risk.
Phase III: Consolidation and Weight-Bearing (Weeks 6-12)
Radiographic evidence of bridging hard callus dictates the transition to Phase III. Weight-bearing is gradually advanced from toe-touch to full weight-bearing under the guidance of physical therapy. For children with neuromuscular disorders (e.g., cerebral palsy, myelomeningocele), orthotic management (such as Ankle-Foot Orthoses - AFOs) is optimized to support the newly aligned limb and facilitate a rapid return to baseline ambulatory function. The hardware is evaluated radiographically for any signs of loosening, migration, or failure.
Phase IV: Long-Term Surveillance and Hardware Management (Months to Years)
Pediatric patients with physeal injuries or pathological fractures require long-term radiographic follow-up, often extending until skeletal maturity. The surgeon must meticulously monitor for late-onset growth arrest, progressive angular deformity, or recurrent cystic lesions. Scanograms or orthoroentgenograms should be utilized annually to track limb length discrepancies accurately. Unlike in adults, where hardware is often left in situ permanently, pediatric implants frequently require elective removal to prevent tethering of growth, stress shielding, or interference with future bone development. The timing of hardware removal must be carefully balanced against the risk of refracture, particularly in cystic lesions that have not fully consolidated.
Summary of Landmark Literature and Clinical Guidelines
The operative management of pediatric pathological and non-accidental fractures is heavily guided by landmark literature and established clinical guidelines that have shaped modern orthopedic practice. A thorough command of these foundational studies is essential for evidence-based surgical decision-making.
In the realm of Osteogenesis Imperfecta, the seminal work by Sofield and Millar (1959) revolutionized the treatment of severe long bone deformities. Their description of multiple osteotomies and intramedullary rod fixation remains the foundational principle for deformity correction in OI. This was later advanced by the development of telescoping nails. The outcomes published by Fassier and Duval demonstrated significantly reduced reoperation rates compared to static rods, as the telescoping mechanism accommodates longitudinal growth, fundamentally altering the life trajectory of children with severe OI.
For benign cystic lesions, the literature has evolved from aggressive open surgery to minimally invasive techniques, and back to a balanced approach. Chigira's classification and subsequent studies highlighted the role of venous outflow obstruction in the pathogenesis of UBCs, leading to treatments like multiple drill hole decompression. However, contemporary guidelines, supported by randomized controlled trials, suggest that while corticosteroid or bone marrow aspirate injections are appropriate first-line treatments for active, non-structural cysts, large structural cysts with impending fractures require formal curettage and grafting to achieve acceptable union rates and prevent catastrophic structural failure.
Regarding Non-Accidental Trauma, the American Academy of Pediatrics (AAP) and the Pediatric Orthopaedic Society of North America (POSNA) have published definitive, legally binding guidelines. These guidelines unequivocally establish that the presence of specific fracture patterns (e.g., posterior rib fractures, metaphyseal corner fractures, multiple fractures in various stages of healing) in a non-ambulatory infant is pathognomonic for abuse until proven otherwise. The literature mandates that definite knowledge or a confirmed specific diagnosis is not required to make a report; reasonable clinical suspicion is sufficient and legally protected. The orthopedic surgeon's adherence to these guidelines is not merely a matter of clinical excellence, but of profound moral and legal duty to protect the most vulnerable patient populations.
