
As academic orthopedic surgeons and medical educators, our understanding and management of pathologic fractures demand a rigorous, evidence-based approach. These fractures represent a significant challenge, complicating patient care and often requiring intricate surgical decision-making. This comprehensive guide synthesizes current knowledge and best practices for evaluating and treating pathologic fractures, targeting orthopedic surgeons, residents, and medical students.
Introduction and Epidemiology
A pathologic fracture is defined as a fracture occurring in bone whose normal structural integrity and inherent strength have been compromised by an underlying disease process. Unlike traumatic fractures, which result from forces exceeding normal bone strength, pathologic fractures occur due to minimal or even no discernible trauma, including during routine activities. This fundamental distinction underscores the critical importance of identifying the underlying pathology, as it dictates prognosis and subsequent treatment.
Etiology of Pathologic Fractures
The causes of pathologic fractures are diverse, broadly categorized into neoplastic, metabolic, infectious, inflammatory, and iatrogenic origins.
* Neoplastic Causes: This is the most prevalent etiology, encompassing both primary bone tumors and metastatic disease. Metastatic disease, particularly from breast, lung, prostate, kidney, and thyroid cancers, accounts for the vast majority of adult pathologic fractures. Primary bone tumors, while less common, can be either benign (e.g., unicameral bone cysts, nonossifying fibromas, fibrous dysplasia, aneurysmal bone cysts, osteochondromas, enchondromas, osteoid osteomas) or malignant (e.g., osteosarcoma, Ewing sarcoma, chondrosarcoma, malignant fibrous histiocytoma, fibrosarcoma).
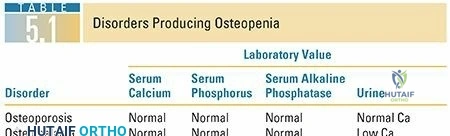
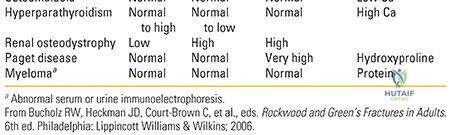
* Metabolic Bone Diseases: Conditions such as severe osteoporosis, osteomalacia, hyperparathyroidism (leading to brown tumors), Paget's disease, and renal osteodystrophy can significantly weaken bone, predisposing to fracture.
* Infectious Causes: Osteomyelitis, particularly chronic forms, can lead to extensive bone destruction and subsequent fracture.
* Inflammatory Conditions: Rarely, severe cases of rheumatoid arthritis or other inflammatory arthropathies can compromise subchondral bone integrity.
* Disuse Osteopenia: Prolonged immobilization or non-weight-bearing status can lead to profound bone loss, making bone susceptible to fracture.
* Iatrogenic Causes: Previous surgical defects, radiation-induced osteonecrosis (which can also predispose to secondary malignancies like Ewing sarcoma or lymphoma), or stress risers created by hardware can be sites of pathologic fracture.
* Necrosis: Avascular necrosis, from various etiologies, can weaken bone structurally and lead to collapse or fracture.
Incidence and Demographics
While pathologic fractures can occur at any age, the specific etiologies show distinct age predilections. In adults, metastatic carcinoma is the leading cause, predominantly affecting the axial skeleton and proximal long bones. The femur and humerus are common sites. In the pediatric population, pathologic fractures are more frequently associated with benign bone lesions. Common predisposing conditions in children include unicameral bone cysts (UBC) in the proximal humerus and femur, nonossifying fibromas (NOF), fibrous dysplasia, and eosinophilic granuloma.
Clinical Presentation
Most pathologic fractures, especially those stemming from benign lesions or early metastatic disease, are asymptomatic before the actual fracture event. The fracture itself often presents acutely with pain and loss of function after minimal trauma or an unexceptional activity. However, specific etiologies can present with prodromal symptoms. For instance, patients with primary malignant bone tumors often report antecedent pain, particularly night pain, which progressively worsens irrespective of activity. Antecedent nocturnal symptoms are rare in benign lesions or early metastatic disease. When evaluating a patient with a suspected pathologic fracture, a thorough history detailing pain characteristics, duration, and associated systemic symptoms is crucial.
Initial Diagnostic Suspicion
The initial radiographic evaluation of a suspected pathologic fracture requires careful scrutiny for features suggestive of the underlying pathology.
* Benign Lesions: Typically exhibit well-defined margins (narrow zone of transition), often with a sclerotic rim, indicating a slow, non-aggressive growth pattern. Matrix production is usually cartilaginous or fibrous. Periosteal reaction, if present, is often solid and benign.
* Aggressive Lesions (Primary Malignant Tumors or Aggressive Metastases): These often present with poorly defined margins (wide zone of transition) where the lesion seamlessly blends into normal bone, indicating rapid, infiltrative growth. The presence of matrix production (osteoid, chondroid) within the lesion can suggest specific tumor types. Periosteal reaction may be aggressive, such as a Codman triangle (elevation of the periosteum by tumor, leaving a triangular new bone formation at the edges) or an onion-skin pattern. A large associated soft tissue component is highly suspicious for malignancy.
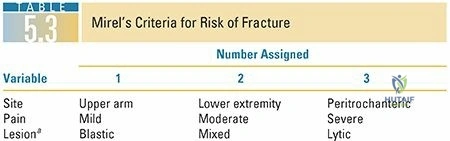
Figure 1: Radiographic example of an aggressive lesion with wide zone of transition and periosteal reaction indicative of underlying malignancy.
Patients presenting with these aggressive radiographic features, especially younger patients, warrant immediate oncologic evaluation. It is critical to obtain a biopsy of a solitary destructive bone lesion before proceeding with definitive fixation, even in patients with a known history of primary carcinoma, to confirm the diagnosis and guide appropriate oncologic management. This principle guards against treating a new primary or a different metastatic lesion incorrectly.
Surgical Anatomy and Biomechanics
The management of pathologic fractures fundamentally relies on an understanding of how disease processes compromise skeletal anatomy and biomechanics. Unlike healthy bone, which can heal predictably and withstand physiological loads, diseased bone presents unique challenges.
Altered Bone Architecture and Strength
Underlying pathologies significantly alter the macroscopic and microscopic architecture of bone:
* Cortical Thinning and Destruction: Lytic lesions erode cortical bone, reducing the cross-sectional area and increasing stress concentration. This significantly lowers the bone's resistance to bending, torsion, and axial compression.
* Medullary Canal Expansion: Lesions that expand within the medullary canal (e.g., metastatic disease, primary tumors, UBCs) displace healthy cancellous bone and weaken the internal structural support.
* Trabecular Disruption: Even in non-lytic processes like osteoporosis, the microarchitecture of trabeculae is compromised, reducing the ability to distribute loads efficiently.
* Abnormal Matrix: Tumor matrices (osteoid, chondroid) or fibrous dysplasia tissue often lack the organized lamellar structure and mineral density of normal bone, rendering them mechanically inferior.
* Vascularity: Hypervascular lesions can predispose to excessive bleeding during surgery, while avascular necrosis creates regions of dead bone that are mechanically weak and prone to collapse.
Biomechanical Principles of Fracture Propagation
The mechanism of injury for pathologic fractures is often described as low-energy trauma or even spontaneous occurrence. This is because the bone's structural integrity is already so compromised that normal physiological stresses exceed its diminished capacity.
* Stress Risers: Focal lesions act as stress risers, concentrating mechanical forces at their weakest point, leading to crack initiation and propagation. This is particularly relevant in long bones where bending and torsional stresses are high.
* Fatigue Fractures: In some chronic conditions, repetitive subthreshold loading can lead to fatigue fractures in weakened bone, rather than an acute traumatic event.
* Weight-Bearing vs. Non-Weight-Bearing Bones: Pathologic fractures are more commonly problematic in weight-bearing bones (femur, tibia, spine) due to constant mechanical loading. However, fractures of the humerus, especially proximally, are also frequent.
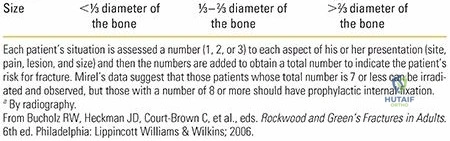
Predicting Impending Fractures Mirels Scoring System
To proactively manage patients with bone lesions and prevent catastrophic pathologic fractures, several scoring systems have been developed. The Mirels score is the most widely adopted and clinically useful tool for assessing the risk of impending pathologic fracture in long bones affected by metastatic disease.
Figure 2: Lateral radiograph showing a lytic lesion in the proximal femur, a common site for impending pathologic fracture.
The Mirels scoring system assigns points (1-3) based on four parameters:
1. Site: Upper extremity (1), lower extremity (2), peritrochanteric (3)
2. Pain: Mild (1), moderate (2), functional (3)
3. Lesion Size: <1/3 cortical destruction (1), 1/3-2/3 cortical destruction (2), >2/3 cortical destruction (3)
4. Lesion Type: Blastic (1), mixed (2), lytic (3)
A total score of 8 or greater is generally considered an indication for prophylactic surgical stabilization, as the risk of subsequent fracture is deemed high enough to warrant intervention. While not universally predictive, the Mirels score provides a standardized method for assessing risk and guiding decision-making regarding prophylactic fixation.
Indications and Contraindications
The decision to proceed with operative versus non-operative management for a pathologic fracture or an impending fracture is complex, requiring careful consideration of the underlying pathology, patient's overall health, prognosis, functional goals, and potential for morbidity.
Indications for Operative Management
Operative management is typically favored for pathologic fractures or high-risk impending fractures due to its ability to provide immediate stability, pain relief, and functional restoration.
Absolute Indications
- Acute Pathologic Fracture: Any displaced or unstable pathologic fracture requires stabilization to alleviate pain and restore function.
- Impending Fracture with High Risk Score: A Mirels score of 8 or higher in a long bone is a strong indication for prophylactic stabilization to prevent an actual fracture and its associated morbidity.
- Uncontrolled Pain: Despite non-operative measures, severe or functionally limiting pain due to a bone lesion, particularly in weight-bearing areas, often warrants surgical intervention.
- Spinal Instability/Neurological Deficit: Pathologic fractures of the spine causing instability, cord compression, or neurological deficits are surgical emergencies.
- Primary Malignant Bone Tumors: Pathologic fractures in the setting of primary malignant tumors often necessitate en bloc resection and reconstruction as part of the oncologic management, even if the fracture itself is relatively stable.
Relative Indications
- Specific Lesion Types: Certain benign aggressive lesions (e.g., aneurysmal bone cysts, aggressive fibrous dysplasia) that cause significant bone destruction or functional impairment may warrant surgical curettage and bone grafting/fixation.
- Need for Biopsy: In cases where a definitive diagnosis cannot be obtained through less invasive means, an open biopsy may be combined with stabilization.
- Anticipated Poor Healing: Pathologic fractures in bone compromised by extensive disease, radiation, or metabolic issues may have a low potential for non-operative healing, favoring surgical stabilization.
Contraindications for Operative Management
While surgery offers significant benefits, it is not always the appropriate course of action.
Absolute Contraindications
- Extremely Limited Life Expectancy: In patients with a very short life expectancy (e.g., less than 4-6 weeks) and extensive systemic disease, the morbidity of surgery may outweigh the potential benefits of improved function or pain relief. Quality of life and comfort care may be prioritized.
- Unfit for Anesthesia/Surgery: Patients with severe comorbidities that render them medically unstable for the proposed surgical procedure and anesthesia.
- Extensive Unresectable Disease: For primary bone tumors or widespread metastatic disease, where local control is not feasible and surgery offers no functional or survival advantage.
Relative Contraindications
- Stable, Non-Displaced Fractures: Certain pathologic fractures, particularly in non-weight-bearing bones or those with minimal displacement, may be managed non-operatively with immobilization and pain control.
- Benign Lesions Amenable to Non-Operative Treatment: Some benign lesions, especially in children (e.g., small nonossifying fibromas, inactive unicameral bone cysts), may resolve spontaneously or respond to non-surgical interventions.
- Patient Preference: If a patient, after thorough counseling regarding risks and benefits, opts for non-operative management, their wishes must be respected within ethical boundaries.
Operative vs. Non-Operative Indications Summary Table
| Feature | Operative Indications | Non-Operative Indications |
|---|---|---|
| Fracture Status | Acute, displaced, or unstable pathologic fracture | Stable, non-displaced pathologic fracture (selected cases) |
| Impending Fracture | Mirels score ≥ 8 (long bones) | Mirels score < 8 or low-risk lesions |
| Pain Control | Intractable pain refractory to conservative management | Well-controlled pain with analgesics and immobilization |
| Underlying Pathology | Primary malignant tumors, aggressive benign lesions, spinal instability | Benign lesions with low risk of fracture, indolent metastases |
| Prognosis | Life expectancy > 4-6 weeks, good functional prognosis | Extremely limited life expectancy (< 4-6 weeks) |
| Medical Fitness | Medically fit for surgery and anesthesia | Unfit for anesthesia or high surgical risk |
| Functional Goal | Restore weight-bearing, mobility, improve quality of life | Comfort care, limited functional expectations |
| Biopsy | Need for open biopsy to establish diagnosis | Diagnosis established, no further tissue required |
Pre Operative Planning and Patient Positioning
Thorough preoperative planning is paramount in the management of pathologic fractures, involving a multidisciplinary approach and meticulous attention to detail to optimize patient outcomes and minimize complications.
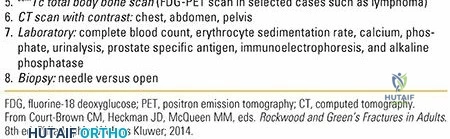
Diagnostic Workup and Staging
- Biopsy: As previously emphasized, a definitive tissue diagnosis is critical. For solitary destructive lesions, a biopsy must precede definitive fixation.
- Technique: Image-guided core needle biopsy is often preferred for initial diagnosis due to its minimally invasive nature. Open biopsy may be necessary if needle biopsy is inconclusive or for larger tissue samples.
- Planning: The biopsy incision must be carefully placed longitudinally and within the planned definitive surgical incision field to avoid contaminating unaffected tissue planes, especially in cases of primary malignancy where limb salvage may be considered.
- Imaging:
- Plain Radiographs: Initial assessment, evaluation of fracture pattern, bone quality, and lesion characteristics (lytic/blastic, margins, periosteal reaction).
- Computed Tomography (CT): Provides detailed assessment of cortical destruction, intraosseous extent, and identification of a soft tissue component. CT angiography may be used for vascular mapping.
- Magnetic Resonance Imaging (MRI): Excellent for evaluating intramedullary extent, soft tissue involvement, neurovascular structures, and identifying skip lesions. Essential for surgical planning in primary tumors.
- Positron Emission Tomography (PET) and Bone Scans: For staging of metastatic disease, identifying other sites of involvement, or assessing metabolic activity of primary tumors.
- Systemic Staging: For suspected malignant lesions, a comprehensive systemic workup (e.g., chest CT, abdominal/pelvic CT, blood work including tumor markers) is necessary to assess the extent of disease and guide overall oncologic management.
Multidisciplinary Team Approach
Effective management of pathologic fractures necessitates collaboration with a specialized team:
* Oncology/Hematology: For systemic treatment of primary or metastatic disease.
* Radiation Oncology: For adjuvant or neoadjuvant radiation therapy, especially for radiosensitive tumors or prophylactic radiation for impending fractures.
* Pathology: Crucial for accurate diagnosis from biopsy specimens.
* Interventional Radiology: For image-guided biopsies, pre-operative embolization of hypervascular lesions (e.g., renal cell carcinoma, thyroid carcinoma) to minimize intraoperative blood loss.
* Palliative Care: For patients with advanced disease, to optimize symptom management and quality of life.
Surgical Goals and Implant Selection
The primary goals of operative intervention are:
* Pain Relief: Stabilizing the fracture significantly reduces pain.
* Functional Restoration: Allowing for early mobilization, weight-bearing, and return to activity.
* Local Disease Control: For primary tumors, this involves oncologic resection principles. For metastatic disease, it may involve intralesional curettage or cement augmentation.
* Prevention of Further Fractures: Prophylactic stabilization or bypassing the entire lesion.
Implant Selection Principles:
* Bypass the Entire Lesion: The chosen implant must extend well beyond the proximal and distal extent of the compromised bone segment to prevent new stress risers or propagation of the fracture.
* Load-Sharing vs. Load-Bearing: While load-sharing implants (e.g., intramedullary nails) are generally preferred, load-bearing implants (e.g., plates, endoprostheses) are often necessary given the severely compromised bone.
* Augmentation: Polymethylmethacrylate (PMMA) cement augmentation is frequently used with screws or intramedullary nails to enhance fixation strength in osteolytic or osteoporotic bone.
* Longer Constructs: Implants should be substantially longer than typical fracture fixation to ensure adequate purchase in healthy bone.
* Consider Future Adjuvant Therapy: Implant choice should accommodate potential radiation therapy or further surgical interventions.
Patient Positioning and Preparation
Patient positioning must be meticulously planned to ensure adequate exposure while protecting compromised bone.
* Fracture Table: Often used for femoral or tibial shaft fractures to provide traction and facilitate reduction. Special care is needed during transfer and positioning to avoid further displacement or injury.
* Lateral Decubitus/Supine: Standard positions adapted for specific approaches (e.g., lateral approach for femur, deltopectoral for humerus).
* Careful Draping and Padding: To protect vulnerable areas, especially over bony prominences.
* Sterile Field: Broad sterile field to allow for extension of incisions if needed and access for potential tumor resection.
Detailed Surgical Approach and Technique
The surgical management of pathologic fractures often combines principles of trauma surgery, oncologic surgery, and reconstructive surgery. The approach and technique must be tailored to the specific anatomical location, type of pathology, and patient's overall condition.
General Principles of Fixation in Diseased Bone
- Immediate Stability: The primary goal is to achieve immediate, rigid fixation that allows for early weight-bearing and mobilization. The potential for bone healing is often compromised, so the construct must be strong enough to withstand physiological loads indefinitely.
- Bypass the Lesion: The implant should extend sufficiently proximal and distal to the lesion to engage healthy bone, typically at least two cortical diameters or more beyond the lesion's margins. This prevents stress concentration at the implant ends.
- Bone Augmentation: PMMA cement is frequently used to augment screw purchase, fill lytic defects, and enhance construct stability, especially with intramedullary nails or plates in osteopenic or osteolytic bone.
- Oncologic Considerations: For primary bone tumors, strict adherence to oncologic principles (e.g., en bloc resection with clear margins) is paramount. For metastatic disease, curettage of the tumor may be performed to decompress the area and reduce tumor burden, but extensive tumor removal often carries higher risks without clear survival benefits.
Specific Surgical Techniques
Intramedullary Nailing
- Indications: Preferred for diaphyseal pathologic fractures and impending fractures of the femur and humerus due to their load-sharing capabilities, minimally invasive nature, and ability to bypass long segments of bone.
- Technique:
- Entry Point: Standard entry points are used (e.g., piriformis fossa, greater trochanteric tip for femur; antegrade or retrograde for humerus).
- Reaming: Reaming can be performed cautiously. In wide medullary canals due to extensive lysis, over-reaming should be avoided.
- Nail Insertion: A large diameter nail is generally selected to provide maximum stability and fill the compromised medullary canal.
- Cement Augmentation: After nail insertion, PMMA cement can be injected through fenestrated nails or around the nail into residual lytic defects to enhance stability. This is particularly useful in metastatic disease or multiple myeloma. The cement provides immediate structural support.
- Locking Screws: Proximal and distal locking screws are essential to prevent rotation and maintain length.
- Challenges: Tumor cells can be disseminated during reaming, though the clinical significance of this in metastatic disease is debated. In very wide canals, achieving adequate nail-bone contact can be difficult without cement.
Figure 3: Intraoperative fluoroscopic image showing an intramedullary nail with cement augmentation for a pathologic femoral fracture.
Plate Fixation
- Indications: Used for metaphyseal or epiphyseal fractures, juxta-articular lesions, or when intramedullary nailing is contraindicated (e.g., very large lytic lesions, extensive soft tissue involvement, extreme canal widening, certain primary tumors).
- Technique:
- Approach: Standard surgical approaches providing adequate exposure are used. For the femur, a lateral approach can be used. For the humerus, a deltopectoral or lateral approach depending on the location.
- Reduction: Gentle reduction of the fracture is performed. The compromised bone may not tolerate aggressive manipulation.
- Plate Application: Long plates, often locking compression plates (LCPs), are preferred. The plate must span the entire lesion and gain solid purchase in healthy bone proximally and distally, typically with at least 6-8 cortices of screw fixation on each side.
- Cement Augmentation: After initial plate placement, lytic defects can be curetted and filled with PMMA cement, which is then often secured with screws. This creates a stronger bone-implant interface.
- Adjuvant Therapy: For primary tumors, tumor resection (intralesional curettage or en bloc resection) is performed, followed by reconstruction.
- Challenges: Plates are load-bearing, which can lead to fatigue failure if bone healing is inadequate or disease progresses. Extensive soft tissue stripping can compromise vascularity.
Endoprosthetic Reconstruction
- Indications: For extensive bone loss, destruction of articular surfaces, primary malignant bone tumors requiring en bloc resection, or when other fixation methods are unlikely to provide durable results (e.g., pathologic fracture through the proximal femur or humerus necessitating arthroplasty).
- Technique:
- Resection: The diseased segment of bone, including any involved joint, is resected with appropriate oncologic margins for primary tumors.
- Reconstruction: A custom or modular endoprosthesis is implanted. This can involve total hip or knee arthroplasty components with extended stems, or tumor prostheses for segments of the femur, tibia, or humerus.
- Advantages: Provides immediate, rigid stability and often excellent functional recovery for the specific joint involved.
- Challenges: Significant surgery with higher risks of infection and long-term mechanical failure.
Vertebral Augmentation and Spinal Instrumentation
- Indications: Pathologic fractures of the spine due to metastatic disease causing intractable pain, impending vertebral collapse, or spinal instability. Vertebroplasty or kyphoplasty for pain relief and stabilization of compressed vertebrae. Posterior or anterior instrumentation for spinal instability or neurological compromise.
- Technique:
- Vertebroplasty/Kyphoplasty: Percutaneous injection of PMMA cement into a collapsed or compromised vertebral body under fluoroscopic guidance. Kyphoplasty involves balloon inflation to restore vertebral height before cement injection.
- Spinal Instrumentation: Open approach to decompress neural elements (laminectomy, corpectomy) and stabilize the spine with pedicle screws and rods, often with adjunctive cement or allograft.
- Challenges: Risk of cement extravasation, neurological injury, particularly in the setting of existing cord compression.
Internervous Planes and Dissection
Meticulous surgical technique, including adherence to internervous planes, is crucial to minimize iatrogenic injury and preserve function.
* Femur: Lateral approach (vastus lateralis split or elevation) for diaphyseal/proximal femur, avoiding damage to the femoral nerve/vessels anteriorly and sciatic nerve posteriorly.
* Humerus: Deltopectoral approach for proximal humerus (between deltoid and pectoralis major, protecting axillary nerve). Lateral approach for humeral shaft (between lateral head of triceps and brachialis, protecting radial nerve).
* Tibia: Anterolateral approach, respecting the anterior tibial neurovascular bundle.
Care must be taken to minimize soft tissue stripping, which can further compromise the already tenuous vascularity of diseased bone.
Complications and Management
Pathologic fractures are associated with higher rates of complications compared to traumatic fractures, primarily due to the compromised nature of the bone, the underlying disease, and the general health status of the patient. Proactive identification and management of these complications are essential for optimal outcomes.
Common Complications and Salvage Strategies
| Complication | Incidence (Approximate) | Salvage Strategies |
| Local Recurrence | ~10-20% for primary bone sarcomas after limb salvage surgery; varies significantly for metastatic disease depending on pathology and margin status. | Definition: The reappearance of the initial disease at the primary site after treatment.
Diagnosis: Close follow-up with clinical exams and imaging (MRI, CT, PET-CT) is crucial. Biopsy to confirm suspicion.
Management:
- Surgical Resection: If feasible, wide local excision of the recurrence is the primary treatment. This may require more aggressive surgery, potentially including amputation if limb salvage is no longer possible or curative margins cannot be achieved.
- Radiation Therapy: Adjuvant or salvage radiation therapy can be used, particularly for incompletely resected margins or in cases where surgery is not feasible.
- Chemotherapy: Systemic chemotherapy is typically reserved for chemosensitive tumors or disseminated disease.
- Biological Therapies: Emerging targeted therapies may be considered depending on tumor genomics. |
| Non-union / Malunion | Up to 10-30% in highly compromised bone, especially with inadequate fixation or progressive disease. | Definition: Failure of bone healing or healing in an unacceptable anatomical position.
Diagnosis: Persistent pain, instability, progressive deformity, and lack of radiographic callus formation over several months.
Management:
- Revision Surgery:
- Improved Fixation: Augment existing fixation with longer implants, additional plates, or cement.
- Bone Grafting: Autograft or allograft may be used, though healing potential remains a concern in compromised bone.
- Adjunctive Biologics: Bone morphogenetic proteins (BMPs) may be considered, though evidence is limited in this setting.
- Adjuvant Therapy: Optimize systemic treatment or local radiation.
- Amputation: In rare, intractable cases, especially with significant pain and poor function. |
| Implant Failure | 5-15%, often due to progressive lysis, inadequate construct, or delayed healing. | Definition: Breakage, loosening, or migration of surgical hardware.
Diagnosis: New pain, instability, palpable crepitus, and radiographic evidence of hardware failure.
Management:
- Revision Surgery: Remove failed hardware, debride any tumor progression, and implant a stronger, longer, or more robust construct. Often requires cement augmentation.
- Endoprosthetic Reconstruction: For extensive bone loss or repeat failure.
- Amputation: As a last resort for unreconstructable defects with severe functional impairment. |
| Infection | 2-10%, higher in immunocompromised patients, open fractures, or extensive tumor surgery. | Definition: Bacterial or fungal colonization of the surgical site.
Diagnosis: Erythema, swelling, fever, purulent drainage, elevated inflammatory markers (ESR, CRP). Aspiration/biopsy for culture.
Management:
- Surgical Debridement: Aggressive debridement of infected tissue, lavage, and removal of contaminated hardware if necessary.
- Antibiotics: Long-term, culture-specific intravenous antibiotics.
- Staged Reconstruction: For chronic infections, implant removal, debridement, antibiotic spacer, followed by delayed reconstruction once infection is controlled.
- Flap Coverage: For soft tissue defects.
- Amputation: In intractable cases where infection cannot be cleared. |
| Neurovascular Injury | <1-5%, depending on location and tumor proximity. | Definition: Damage to nerves or blood vessels during surgery.
Diagnosis: Intraoperative bleeding, post-operative neurological deficit (motor/sensory loss), compartment syndrome, pulse deficits.
Management:
- Immediate Repair: Intraoperative repair of injured vessels (vascular surgeon consultation).
- Nerve Repair/Grafting: If a major nerve is transected, primary repair or nerve grafting may be attempted.
- Postoperative Monitoring: Close monitoring for compartment syndrome and neurological changes.
- Rehabilitation: Nerve gliding exercises, bracing, pain management. |
| Fat Embolism Syndrome| Rare, but can be higher in long bone IM nailing and compromised marrow. | Definition: Systemic effects from embolized fat globules after trauma or surgery.
Diagnosis: Respiratory distress, mental status changes, petechial rash.
Management:
- Supportive Care: Oxygen, ventilatory support, hemodynamic stabilization.
- Prevention: Careful reaming, limiting intramedullary pressure during nailing. |
| Systemic Complications| Varies widely based on underlying disease and patient health. | Definition: Complications related to underlying malignancy (e.g., hypercalcemia, coagulopathy) or general surgical risks (e.g., DVT, PE, cardiac events, renal failure).
Diagnosis: Careful preoperative medical optimization, vigilant postoperative monitoring.
Management:
- Multidisciplinary Medical Management: Collaboration with oncologists, intensivists, internists.
- Prophylaxis: DVT prophylaxis, judicious fluid management. |
| Soft Tissue Complications | 5-15%, higher with radiation, extensive resections, or poor nutritional status. | Definition: Wound dehiscence, necrosis, hematoma, seroma.
Diagnosis: Clinical examination of the wound.
Management:
- Wound Care: Local wound care, vacuum-assisted closure (VAC) therapy.
- Debridement and Closure: Surgical debridement of necrotic tissue, secondary closure, or flap coverage (plastic surgery consultation).
- Hematoma/Seroma Drainage: Surgical or percutaneous drainage. |
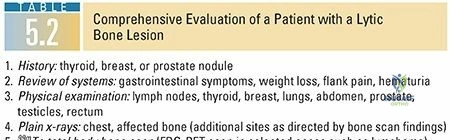
Figure 4: Radiograph demonstrating implant failure and subsequent non-union of a pathologic fracture, often necessitating revision surgery.
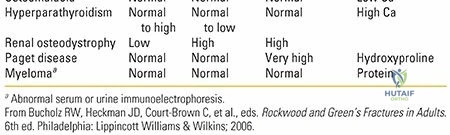
Figure 5: Postoperative image depicting potential soft tissue and wound complications following extensive oncologic surgery.
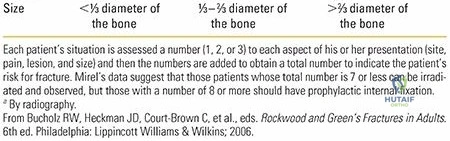
Figure 6: Example of a revision surgery for implant failure, showing a longer, more robust construct and cement augmentation.
Overall Prognosis and Limb Salvage
Pathologic fracture complicates the prognosis but does not inherently mitigate against successful limb salvage for primary bone sarcomas. However, local recurrence rates are often higher following pathologic fractures, emphasizing the need for meticulous oncologic resection and careful follow-up. For metastatic disease, surgical intervention is primarily palliative, aimed at improving quality of life and function.
Post Operative Rehabilitation Protocols
Postoperative rehabilitation is an integral component of managing pathologic fractures, aiming to restore function, alleviate pain, and integrate with adjuvant oncologic therapies. Protocols must be individualized, considering the patient's overall prognosis, the extent of bone compromise, the stability of fixation, and the type of underlying pathology.
Immediate Postoperative Period
- Pain Management: A multimodal approach is crucial, often involving opioid and non-opioid analgesics, nerve blocks, and adjunctive medications to control pain effectively and facilitate early mobilization.
- Wound Care: Meticulous wound care to monitor for infection and promote healing.
- Weight-Bearing Status:
- Immediate Protected Weight-Bearing: Often permitted for robustly fixed long bone fractures, particularly with intramedullary nails and cement augmentation, to facilitate early ambulation and reduce complications of immobility.
- Delayed/Non-Weight-Bearing: May be necessary for less stable constructs, extensive bone defects, or certain types of primary tumor resections. Careful patient education regarding limitations is essential.
- Early Mobilization: As soon as medically stable, initiation of range of motion exercises for adjacent joints and ambulation with appropriate assistive devices (walker, crutches) to prevent stiffness, muscle atrophy, and complications like deep vein thrombosis (DVT) and pneumonia.
Progressive Rehabilitation Phases
- Phase I: Acute Recovery and Protection (Weeks 0-6)
- Goals: Pain control, wound healing, prevention of complications, maintain joint range of motion, initiation of protected weight-bearing.
- Interventions: Passive and active-assisted range of motion (PROM/AAROM) exercises, isometric strengthening, gentle ambulation with maximal assistance, education on precautions.
- Phase II: Intermediate Strengthening and Functional Progression (Weeks 6-12)
- Goals: Increase strength, improve active range of motion, progress weight-bearing, enhance functional independence.
- Interventions: Progressive resistive exercises (PREs), balance and proprioception training, gait training with decreasing assistance, initiation of light functional activities. Close collaboration with physical and occupational therapists.
- Phase III: Advanced Strengthening and Return to Activity (Weeks 12+)
- Goals: Maximize strength and endurance, achieve full functional independence, return to modified activities of daily living (ADLs) or work.
- Interventions: High-level strengthening, sport-specific (if applicable and appropriate for prognosis) or vocational rehabilitation, continued focus on endurance and balance.
Integration of Adjuvant Therapies
Rehabilitation protocols must be seamlessly integrated with adjuvant oncologic treatments such as chemotherapy and radiation therapy.
* Chemotherapy: Can cause fatigue, myelosuppression, and neuropathy, which may impact rehabilitation tolerance and progression. Therapy sessions may need to be adjusted during cycles.
* Radiation Therapy: Can impair wound healing, cause soft tissue fibrosis, and further compromise bone viability. Radiation typically starts a few weeks post-surgery after initial wound healing. Rehabilitation must account for potential localized tissue changes and monitor for radiation-induced complications.
Long-Term Monitoring and Follow-Up
Regular clinical and radiographic follow-up is critical.
* Clinical Assessment: Monitor for pain, function, neurological status, and signs of implant loosening or infection.
* Radiographic Assessment: Plain radiographs at regular intervals (e.g., 3, 6, 12 months, then annually) to assess implant integrity, bone healing (if applicable), and progression or recurrence of the underlying disease. MRI or CT may be used to evaluate specific concerns.
* Oncologic Surveillance: Continued surveillance for systemic disease progression or local recurrence in consultation with oncology specialists.
The ultimate goal of rehabilitation is to optimize the patient's quality of life and functional independence, acknowledging the limitations imposed by the underlying pathology and its treatment.
Summary of Key Literature and Guidelines
The management of pathologic fractures is a rapidly evolving field, with ongoing advancements in diagnostic imaging, surgical techniques, and adjuvant therapies. A commitment to evidence-based practice and continuous learning is paramount for orthopedic surgeons.
Key Literature and Consensus Guidelines
- Mirels' Criteria (1989): This seminal work established a widely accepted scoring system for predicting the risk of impending pathologic fractures in long bones due to metastatic disease. While not without limitations, it remains a cornerstone of clinical decision-making regarding prophylactic stabilization.
- National Comprehensive Cancer Network (NCCN) Guidelines: Provide comprehensive, evidence-based guidelines for the diagnosis, staging, and treatment of various cancers, including primary bone tumors and metastatic bone disease. These guidelines offer valuable insights into multidisciplinary management, surgical indications, and adjuvant therapies.
- Orthopedic Oncologic Society (OOS) / Musculoskeletal Tumor Society (MSTS) Guidelines: These professional societies regularly publish consensus statements and treatment algorithms specific to musculoskeletal tumors, addressing surgical techniques, biopsy principles, and limb salvage considerations.
- AAOS Clinical Practice Guidelines: The American Academy of Orthopaedic Surgeons (AAOS) periodically publishes clinical practice guidelines on fracture management and musculoskeletal conditions, which may include aspects relevant to pathologic fractures.
Evolving Concepts and Future Directions
- Personalized Medicine: Advances in genomics and molecular profiling are leading to more targeted therapies for various cancers, which will undoubtedly influence the systemic management of patients with pathologic fractures and potentially impact bone healing.
- Advanced Imaging Modalities: Ongoing development of quantitative imaging techniques (e.g., texture analysis of CT/MRI, advanced PET tracers) may provide more accurate assessments of bone quality, tumor response to therapy, and improved prediction of fracture risk.
- Biologic Augmentation: Research into novel biologic agents (e.g., parathyroid hormone analogs, specific growth factors, stem cell therapies) to enhance bone healing in compromised bone is ongoing, although their role in pathologic fractures is still largely experimental.
- Minimally Invasive Techniques: Continued refinement of minimally invasive surgical approaches, particularly in spinal interventions and percutaneous fixation, aims to reduce surgical morbidity while maintaining effective stabilization.
- Role of Radiosurgery: Stereotactic body radiation therapy (SBRT) or radiosurgery is increasingly being used for localized control of metastatic bone lesions, offering a non-invasive alternative or adjunct to surgical stabilization, particularly for spinal metastases.
Conclusion
The effective management of pathologic fractures requires a nuanced understanding of the underlying disease, sound biomechanical principles, meticulous surgical technique, and a robust multidisciplinary approach. By adhering to established guidelines, staying abreast of evolving literature, and prioritizing patient-centered care, orthopedic surgeons can optimize outcomes for this challenging patient population. Early diagnosis, appropriate staging, and individualized treatment plans remain critical to achieving pain relief, functional restoration, and improved quality of life.
Clinical & Radiographic Imaging
Detailed Chapters & Topics
Dive deeper into specialized chapters regarding pathologic-fractures