Pathological Subtrochanteric Femoral Fracture Secondary to Multiple Myeloma: Diagnostic Nuances & Bone Scintigraphy

Key Takeaway
Multiple myeloma presenting as a pathological femoral fracture often involves elderly patients with pre-existing vague symptoms. Diagnostic imaging shows comminuted lytic lesions and a widespread lytic pattern. Crucially, Tc-99m bone scans typically show 'cold' or equivocal lesions due to osteoclast predominance, a key differentiator from other metastatic processes.
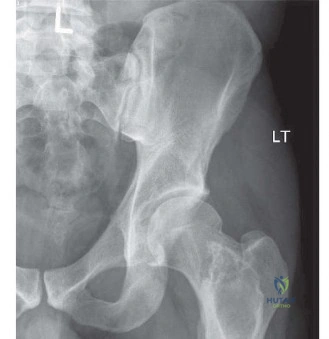
An 82-year-old male presents with a painful, shortened, and externally rotated left leg after a low-energy fall. Radiographs reveal a comminuted subtrochanteric fracture with significant cortical destruction. Given the history of weight loss and back pain, you suspect a pathological fracture. Describe your initial assessment and how you would differentiate between a traumatic and pathological cause on plain films.

Candidate: I would perform a thorough history and physical, looking for "B" symptoms. On X-rays, I’d look for signs like cortical thinning, permeative margins, or a lack of callus, which would suggest a pathological process rather than a standard fragility fracture.
Candidates often jump straight to surgery or mention specific staging scans without first identifying the radiographic markers of malignancy. Failing to mention "cortical destruction" or "ill-defined margins" demonstrates a lack of radiographic pattern recognition.
A high-scoring answer addresses the "red flags" (age, B-symptoms, mechanical fall). Radiographically, I look for: (1) Cortical destruction or focal bone loss, (2) Ill-defined (permeative/moth-eaten) margins vs. sclerotic, (3) Absence of healing (no callus formation), and (4) Disproportionate deformity given the mechanism. I would then state that an expedited staging workup (CT Chest/Abd/Pelvis) is mandatory to identify the primary tumor.
The staging workup confirms Multiple Myeloma. You are planning surgical intervention for this subtrochanteric fracture. What are the biomechanical principles you must adhere to when selecting an implant for this specific region?
Candidate: The subtrochanteric region is under high stress. I would use a long cephalomedullary nail to bridge the fracture and protect the rest of the femur, potentially using cement if there is a large void.
Candidates failing to mention the "cantilever" effect or the need to bypass the entire femoral shaft. They often forget that in pathological bone, the implant must span beyond the lesion to prevent a second fracture (fracture at the tip of the implant).
The subtrochanteric femur is a high-stress transition zone. My principles are: (1) Load sharing/bypass: Use a long cephalomedullary nail to span from the femoral head to the distal diaphysis. (2) Construct stability: Ensure the proximal cephalic screw is well-seated. (3) Medial buttress restoration: Use PMMA cement for structural augmentation if cortical defects exist, as hardware alone in lytic bone will suffer cyclic fatigue failure.
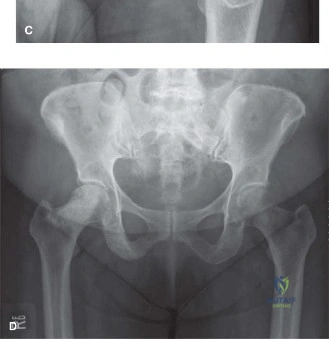
Look at this image. Why is this diagnostic modality generally discouraged for initial staging in patients with Multiple Myeloma, and what would you use instead?
Candidate: That is a Technetium bone scan. Myeloma is often "cold" on these because it's a lytic process, so it won't pick up the tracer. I would use a CT or an MRI instead.
Failing to explain the underlying pathophysiology. Simply saying it's "not sensitive" is insufficient. An elite candidate explains the suppression of osteoblastic activity by myeloma cells (Dickkopf-1 pathway) which leads to a false-negative result.
Standard Technetium-99m MDP bone scans rely on osteoblastic activity. In Multiple Myeloma, the disease creates an uncoupling of bone remodeling: osteoclasts are activated, but osteoblasts are inhibited by myeloma-secreted factors like Dickkopf-1 and sclerostin. Consequently, lesions are frequently "cold" or occult. I would use Whole Body Low-Dose CT (WBLDCT), MRI, or 18F-FDG PET-CT, which visualize marrow infiltration and direct lytic destruction, providing an accurate assessment of skeletal burden.
Describe your intraoperative setup and the specific surgical pearls for placing a cephalomedullary nail in a patient with significant proximal femoral lytic destruction.
Candidate: I'd put them on a fracture table, ensure good fluoroscopy access, and carefully ream. I'd add cement through a cortical window to make sure the hardware stays in place.
Ignoring the risks of iatrogenic fracture. Candidates often suggest aggressive reaming or traction, which can shatter the fragile bone. They also miss the importance of the entry point accuracy in compromised bone.
Key pearls include: (1) Avoid aggressive traction to prevent further displacement. (2) Entry point accuracy is critical; use a precise starting point on the medial greater trochanter to avoid varus malreduction. (3) Reaming nuance: Over-reaming by 1.5mm is essential to reduce hoop stresses that could fracture the osteopenic shaft. (4) Cement augmentation: Use a lateral approach for intralesional curettage; inject cement to fill the lytic void and restore the medial buttress, ensuring it interdigitates with cancellous bone to create a composite, stable construct.
