
Introduction and Epidemiology
The development and growth of the skeletal system from gestation to skeletal maturity create interrelated fibrous, tendinous, cartilaginous, and osseous changes resulting in patterns of susceptibility and reparative response that distinguish the pediatric patient from the adult. Pediatric orthopaedic trauma requires a profound understanding of these unique biological and biomechanical properties. As a fundamental rule of pediatric fracture management, the younger the patient, the greater the remodeling potential. Consequently, absolute anatomic reduction in a child is often less critical than in a comparable injury in an adult, provided the deformity lies in the plane of adjacent joint motion and the patient possesses sufficient remaining growth.
The incidence of pediatric fractures is steadily increasing, a trend primarily attributed to heightened participation in organized and extreme sports. Epidemiological data indicate that approximately fifty percent of all children will sustain at least one fracture during childhood. Despite this high incidence of morbidity, the overall mortality rate of children has fallen drastically from 1 in 250 per year in 1900 to less than 1 in 4,000 per year in contemporary analyses. This decline is largely attributed to improved public education, the widespread use of preventive devices, and advancements in trauma resuscitation and medical care. Nevertheless, accidental trauma remains the leading cause of death in children ages 1 to 14 years.
Skeletal trauma accounts for ten to fifteen percent of all childhood injuries. Of these skeletal injuries, approximately fifteen to thirty percent represent physeal fractures, with fractures of the phalanges being the most common physeal injury overall. Gender disparities in fracture incidence are well documented. From birth to age sixteen, forty-two percent of boys will sustain at least one fracture compared with twenty-seven percent of girls. The overall ratio of boys to girls who sustain a single, isolated fracture is 2.7 to 1. The peak incidence of fractures in boys occurs at age sixteen, with an incidence of 450 per 10,000 per year. Conversely, the peak incidence in girls occurs at age twelve, with an incidence of 250 per 10,000 per year. Open fractures in the pediatric population remain relatively rare, comprising less than five percent of all pediatric fractures.
When evaluating pediatric trauma, the orthopaedic surgeon must maintain a high index of suspicion for non-accidental trauma. Discrepancies between the reported mechanism of injury and the observed fracture pattern, particularly in non-ambulatory infants, require immediate multidisciplinary evaluation. Classic patterns highly specific for non-accidental trauma include posterior rib fractures, metaphyseal corner fractures, and fractures of the sternum, scapula, or spinous processes.
Surgical Anatomy and Biomechanics
Pediatric bone exhibits fundamental material differences compared to mature adult bone. It possesses a higher water content and lower mineral content per unit volume. Therefore, pediatric bone demonstrates a significantly lower modulus of elasticity, making it less brittle, and exhibits a higher ultimate strain-to-failure. Biomechanically, pediatric bone is relatively stronger in tension than in compression when compared to adult bone. These unique material properties result in specific injury patterns rarely seen in adults, including plastic deformation, buckle or torus fractures, and greenstick fractures.
The physis, or growth plate, is a highly specialized cartilaginous structure that varies in thickness depending on patient age and anatomic location. It serves as the primary center for longitudinal bone growth. Biomechanically, the physis is frequently weaker than the surrounding trabecular bone in torsion, shear, and bending forces. This relative structural weakness predisposes the pediatric patient to failure through this delicate area rather than through the adjacent ligamentous or osseous structures.
Histological Zones of the Physis
The physis is traditionally divided into four distinct histological zones, each with specific cellular functions and vulnerabilities.
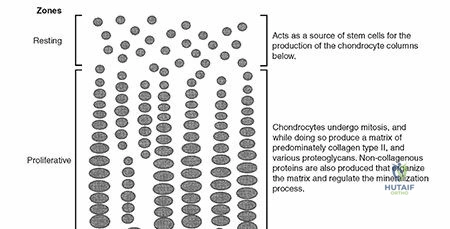
- Reserve Zone: Also known as the resting or germinal zone, this layer is immediately adjacent to the epiphysis. It stores lipids, glycogen, and proteoglycans necessary for matrix production. It is relatively inactive in cell division but is the target zone for certain metabolic conditions such as Gaucher disease.
- Proliferative Zone: This zone is characterized by longitudinal columns of dividing chondrocytes. It is the primary site of longitudinal growth and is heavily influenced by growth hormone and local factors. This zone is the primary site of pathology in achondroplasia.
- Hypertrophic Zone: Chondrocytes in this zone mature, enlarge, and eventually undergo apoptosis. This zone lacks substantial collagen and is structurally the weakest layer of the physis. Consequently, most physeal fractures, including Slipped Capital Femoral Epiphysis, propagate through the hypertrophic zone.
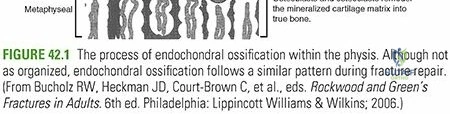
- Zone of Provisional Calcification: Here, the cartilaginous matrix is calcified, and vascular invasion from the metaphysis begins, leading to enchondral ossification.
The Periosteum and Ligamentous Anatomy
The periosteum in a child is a thick, highly vascular, and osteogenic fibrous structure that can measure up to several millimeters in thickness. It encompasses the entire bone except for the articular ends. At the level of the physis, the periosteum thickens and becomes continuous with the perichondral ring of LaCroix. This anatomical arrangement offers substantial additional resistance to shear forces across the growth plate. The robust nature of the pediatric periosteum often leaves an intact hinge following displacement, which can be utilized to aid in closed reduction and maintain stability during cast immobilization.

As a general rule, ligaments in children are functionally stronger than the adjacent physis. Therefore, a higher proportion of mechanical forces that would produce ligamentous sprains or ruptures in adults result in physeal fractures in children.
Vascular Anatomy of the Growing Bone
The blood supply to the growing bone is uniquely adapted to support rapid osteogenesis. It includes a rich metaphyseal circulation with fine capillary loops that terminate abruptly at the physis. The epiphyseal circulation is separate and supplies the reserve and proliferative zones. In the neonate, small transphyseal vessels may traverse the growth plate, ending in the epiphysis, which explains the mechanism by which metaphyseal osteomyelitis can spread to the joint space in infants, resulting in concurrent septic arthritis. By around eighteen months of age, these transphyseal vessels regress, establishing the physis as a relative barrier to the spread of infection.
Indications and Contraindications
The decision to proceed with operative intervention in pediatric fractures relies on several critical factors, including the patient age, remaining growth potential, specific bone involved, fracture pattern, and the presence of associated injuries. While conservative management with closed reduction and casting remains the gold standard for the vast majority of pediatric fractures, operative management is increasingly utilized to ensure rapid mobilization, prevent prolonged hospitalization, and avoid the psychosocial burden of extensive immobilization.
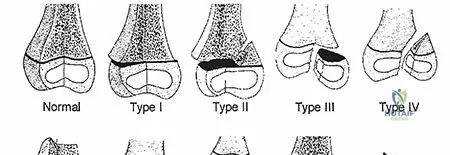
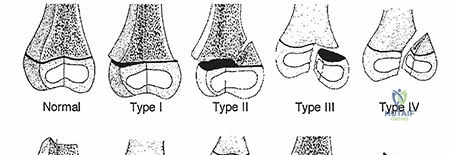
Absolute indications for surgical intervention include open fractures requiring thorough irrigation and debridement, fractures associated with vascular compromise that does not resolve with reduction, compartment syndrome requiring fasciotomy, and irreducible intra articular fractures. Salter Harris type III and type IV fractures inherently involve the articular surface and the physis; these injuries demand anatomic reduction to restore joint congruity and minimize the risk of premature physeal closure.
Relative indications include polytrauma, where stabilization of long bone fractures facilitates nursing care and pulmonary toilet, and fractures that demonstrate unacceptable alignment despite optimal attempts at closed reduction. The definition of unacceptable alignment varies strictly by age and anatomic location. For example, a midshaft femur fracture with twenty degrees of anterior angulation may be perfectly acceptable in a three year old due to robust remodeling potential, but the same angulation in a fourteen year old necessitates surgical fixation.
Contraindications to operative management include active local or systemic infection at the planned surgical site, unless the surgery is specifically aimed at source control. Severe physiological instability in a polytraumatized child may preclude definitive fixation, necessitating the use of temporary damage control external fixation until the patient is physiologically optimized.
| Clinical Scenario | Operative Indications | Non Operative Indications |
|---|---|---|
| Diaphyseal Femur Fracture | Age over 5 years, polytrauma, open fracture, unacceptable shortening or angulation | Age under 5 years, isolated injury, acceptable alignment in spica cast |
| Supracondylar Humerus Fracture | Gartland Type III and IV, Type II with medial comminution or anterior humeral line missing capitellum, pulseless pink hand | Gartland Type I, stable Type II with intact posterior hinge and acceptable alignment |
| Forearm Diaphyseal Fracture | Unacceptable angulation or rotation based on age, failure of closed reduction, open fracture | Acceptable alignment, younger age with high remodeling potential |
| Intra Articular Physeal Fracture | Salter Harris III and IV with greater than 2mm step off or gap | Non displaced Salter Harris III and IV, isolated Salter Harris I and II |
| Tibial Eminence Fracture | Meyers McKeever Type III, Type II failing closed reduction, meniscal entrapment | Meyers McKeever Type I, Type II achieving anatomic reduction with extension |
Pre Operative Planning and Patient Positioning
Thorough preoperative planning is paramount in pediatric orthopaedic trauma to minimize surgical time, reduce radiation exposure, and ensure the availability of appropriate pediatric specific implants. Standard radiographic evaluation must include high quality orthogonal anteroposterior and lateral views of the injured extremity, ensuring the joints above and below the fracture are visualized. Contralateral comparison views are frequently invaluable, particularly for injuries involving complex ossification centers such as the pediatric elbow, to differentiate true fractures from normal developmental anatomy.
Advanced imaging modalities are utilized selectively. Computed tomography with multiplanar reconstruction is indicated for complex intra articular fractures, such as triplane or Tillaux fractures of the distal tibia, to precisely define the fracture geometry and plan screw trajectories. Magnetic resonance imaging is highly sensitive for identifying occult cartilaginous injuries, unossified epiphyseal fractures in infants, and assessing the integrity of the soft tissue envelope or vascular supply in the setting of suspected avascular necrosis.
Preoperative templating must account for the unique dimensions of the pediatric medullary canal. When planning for elastic stable intramedullary nailing, the narrowest diameter of the isthmus should be measured to select the appropriate nail size. The combined diameter of the two elastic nails should approximate eighty percent of the narrowest canal diameter to ensure adequate three point biomechanical fixation.
Patient positioning must facilitate unhindered access for intraoperative fluoroscopy. Radiolucent operating tables are mandatory. For upper extremity trauma, the patient is typically positioned supine with the arm extended on a radiolucent hand table. The C arm should be brought in parallel to the table to allow for seamless transition between anteroposterior and lateral views by simply rotating the arm or the machine, rather than repositioning the patient. For lower extremity trauma, a radiolucent flat table is generally preferred over a fracture table in younger children, as manual traction provides sufficient reduction force and avoids the risk of perineal soft tissue complications associated with fracture table posts.
Pediatric anesthesia considerations are critical. Meticulous attention must be paid to temperature regulation, as children have a higher body surface area to mass ratio and are prone to rapid hypothermia in the operating theater. Fluid management and allowable blood loss calculations must be strictly monitored, as the total blood volume in a small child is significantly lower than in an adult.
Detailed Surgical Approach and Technique
The surgical management of pediatric fractures utilizes specific modalities tailored to the biological advantages of the growing skeleton. The vast majority of operative pediatric fractures can be managed with minimally invasive techniques, preserving the fracture hematoma and the osteogenic potential of the periosteum.
Closed Reduction and Percutaneous Pinning
Closed reduction and percutaneous pinning is the workhorse technique for pediatric metaphyseal and epiphyseal fractures, most notably supracondylar humerus fractures and lateral condyle fractures.
For a displaced supracondylar humerus fracture, the procedure begins with longitudinal traction and correction of coronal plane translation and rotation. The elbow is then hyperflexed while applying an anteriorly directed force to the olecranon to correct sagittal plane extension deformity. Once anatomic reduction is confirmed on orthogonal fluoroscopic views, fixation is achieved using smooth Kirschner wires. Smooth pins are utilized to allow for easy removal in the clinic setting and to minimize the risk of physeal damage.
Pin configuration typically involves two or three divergent lateral entry pins. The starting point is the center of the lateral epicondyle. The pins are driven across the fracture site, engaging the medial cortex of the proximal fragment to ensure bicortical purchase. If medial comminution is present, a medial pin may be required to prevent varus collapse. However, medial pin placement carries a significant risk of iatrogenic injury to the ulnar nerve. To mitigate this risk, the elbow should be extended to less than ninety degrees to allow the ulnar nerve to fall posteriorly, and a mini open incision should be utilized to directly visualize and protect the nerve before pin insertion.
Elastic Stable Intramedullary Nailing
Elastic stable intramedullary nailing has revolutionized the treatment of pediatric diaphyseal fractures, particularly of the femur, tibia, and forearm. This technique relies on the principle of symmetric, opposing three point biomechanical fixation within the medullary canal.
For a pediatric diaphyseal femur fracture, the patient is positioned supine on a radiolucent table. Two titanium or stainless steel elastic nails are selected. The nails are pre contoured into a gentle bow, with the apex of the curve corresponding to the level of the fracture. The entry points are typically retrograde, utilizing the medial and lateral distal femoral metaphysis, approximately two centimeters proximal to the distal femoral physis to avoid physeal injury.
Small incisions are made, and the cortex is opened with an awl or drill. The nails are advanced sequentially up the medullary canal to the level of the fracture. Closed reduction is achieved using manual traction and manipulation. The nails are then advanced across the fracture site into the proximal fragment, diverging into the proximal metaphysis. One nail is driven towards the femoral neck, and the other towards the greater trochanter. The opposing tension of the contoured nails provides rotational and angular stability while allowing for micro motion at the fracture site, which stimulates robust secondary bone healing via callus formation. The nails are cut flush with the cortex to minimize soft tissue irritation.
Open Reduction and Internal Fixation
Open reduction and internal fixation utilizing plates and screws is reserved for specific indications in the pediatric population. These include intra articular fractures requiring absolute anatomic reduction, such as displaced lateral condyle fractures or transitional ankle fractures, and diaphyseal fractures in older adolescents approaching skeletal maturity where elastic nails would fail to provide sufficient biomechanical stability.
When utilizing plate osteosynthesis, meticulous surgical technique is required to minimize periosteal stripping. Submuscular, minimally invasive plate osteosynthesis techniques are preferred. If fixation must cross a physis, smooth pins or screws placed perfectly parallel to the physis should be utilized. Transphyseal screws should be avoided if possible; if necessary, they should be fully threaded, placed centrally within the physis, and removed as soon as fracture healing allows to minimize the risk of growth arrest.
Rigid intramedullary nailing is indicated for femur and tibia fractures in older adolescents who have achieved skeletal maturity or are nearing complete physeal closure. For adolescent femur fractures, a lateral trochanteric entry point is strictly utilized to avoid the piriformis fossa and the medial circumflex femoral artery, thereby minimizing the catastrophic risk of iatrogenic avascular necrosis of the femoral head.
Complications and Management
Despite the robust healing potential of pediatric bone, significant complications can arise from both the initial trauma and the subsequent surgical management. Anticipation, early recognition, and appropriate management of these complications are critical to ensuring optimal long term outcomes.
Premature physeal closure, resulting in complete growth arrest or partial arrest with subsequent angular deformity, is the most feared complication of pediatric trauma. The risk is highest with high energy Salter Harris type IV and type V injuries, particularly around the distal femur and distal tibia. If a physeal bar forms and encompasses less than fifty percent of the cross sectional area of the physis, and the child has at least two years of remaining growth, a physeal bar excision (Langenskiold procedure) is indicated. This involves precise mapping of the bar using magnetic resonance imaging or computed tomography, surgical resection of the osseous tether, and interposition of a biologically inert material, such as autologous fat or synthetic wax, to prevent recurrence.
Overgrowth is a unique complication observed primarily in pediatric diaphyseal femur fractures in children between the ages of two and ten years. The hyperemic response associated with fracture healing stimulates the adjacent physes, leading to accelerated longitudinal growth. To compensate for this anticipated overgrowth, surgeons often intentionally accept one to two centimeters of overriding at the fracture site during initial reduction and casting.
Compartment syndrome remains a devastating potential complication, particularly following supracondylar humerus fractures, proximal third tibia fractures, and forearm fractures. The classic signs of pain out of proportion to the injury and pain with passive stretch of the involved muscles must prompt immediate clinical evaluation. In the pediatric patient, agitation and increasing analgesic requirements are often the earliest indicators. If compartment syndrome is diagnosed, emergent four compartment fasciotomy is mandatory.
| Complication | Estimated Incidence | Salvage and Management Strategies |
|---|---|---|
| Physeal Growth Arrest | 1 to 10 percent (varies by anatomic site and severity) | Serial radiographic monitoring, physeal bar excision with fat interposition, corrective osteotomy, contralateral epiphysiodesis |
| Overgrowth (Limb Length Discrepancy) | Common in femur fractures ages 2 to 10 | Intentional bayonet apposition during initial reduction, shoe lifts, contralateral epiphysiodesis if discrepancy exceeds 2 cm at maturity |
| Compartment Syndrome | Less than 1 percent | High clinical suspicion, removal of all constrictive dressings, emergent surgical fasciotomy |
| Pin Tract Infection | 2 to 5 percent | Oral antibiotics for superficial erythema, pin removal and intravenous antibiotics for deep infection or osteomyelitis |
| Malunion | 5 to 15 percent (depends on acceptable criteria) | Observation if remodeling potential is high, corrective osteotomy for severe angular or rotational deformities affecting joint mechanics |
Post Operative Rehabilitation Protocols
Rehabilitation protocols following pediatric orthopaedic trauma differ significantly from adult protocols. The rapid rate of osteogenesis allows for shorter durations of immobilization. Prolonged immobilization is generally avoided to prevent joint stiffness and osteopenia, although children are remarkably resilient and rarely develop the permanent adhesive capsulitis seen in adults.
For fractures managed with closed reduction and percutaneous pinning, such as supracondylar humerus fractures, the extremity is typically immobilized in a long arm cast or splint for three to four weeks. Clinical union is usually evident at this stage. The pins are removed in the outpatient clinic setting, and the child is allowed to begin active range of motion exercises. Formal physical therapy is rarely required, as children naturally regain motion through play and activities of daily living.
For lower extremity fractures managed with elastic stable intramedullary nailing, postoperative protocols depend on the stability of the fixation and the age of the child. Generally, the patient is placed in a soft dressing or a removable splint. Touch down weight bearing is initiated immediately, progressing to full weight bearing as radiographic callus becomes evident, typically around four to six weeks.
Hardware removal is a unique consideration in pediatric orthopaedic trauma. Unlike adults, where retained hardware is often asymptomatic, retained implants in a growing child can become deeply embedded in cortical bone or migrate as the bone grows. Furthermore, retained hardware can complicate future imaging or surgical procedures. Therefore, routine removal of elastic nails, plates, and screws is generally recommended once complete consolidation and remodeling of the fracture have occurred, typically six to twelve months postoperatively.
Summary of Key Literature and Guidelines
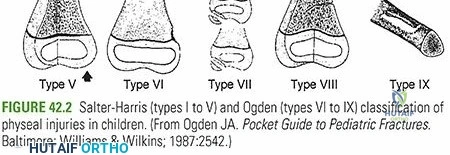
The foundation of pediatric fracture management is built upon several landmark studies and classification systems. The Salter and Harris classification, originally published in 1963, remains the universal language for describing physeal injuries. Their prognostic guidelines regarding the risk of growth arrest based on the fracture pattern continue to dictate clinical decision making.
The treatment of pediatric diaphyseal femur fractures was revolutionized by the introduction of elastic stable intramedullary nailing. The Flynn criteria, established to evaluate the outcomes of this technique, remain the standard for assessing success, focusing on limb length discrepancy, angular deformity, and complications.
Contemporary practice is heavily guided by evidence based clinical practice guidelines. The American Academy of Orthopaedic Surgeons has published comprehensive guidelines on the management of pediatric supracondylar humerus fractures and pediatric diaphyseal femur fractures. These guidelines emphasize the importance of early operative intervention for displaced supracondylar fractures to minimize neurovascular complications and advocate for the use of elastic nailing in school aged children with femur fractures to accelerate recovery and reduce the psychosocial burden of spica casting. Familiarity with these foundational texts and evolving guidelines is essential for any orthopaedic surgeon managing pediatric trauma.
Detailed Chapters & Topics
Dive deeper into specialized chapters regarding pediatric-fractures-and-dislocations