Children's Wrist and Hand Fractures: What You Need to Know

Key Takeaway
This article provides essential research regarding Children's Wrist and Hand Fractures: What You Need to Know. Pediatric carpal injuries in the wrist and hand are rare due to protective factors like the distal radial physis and abundant cartilaginous carpal envelopes. These injuries typically result from direct trauma or high-energy falls onto an outstretched hand. Localized tenderness is a common sign. While rare in younger children, scaphoid fractures are the most common carpal bone fracture, peaking around age 15.
Comprehensive Introduction and Patho-Epidemiology

Pediatric injuries to the wrist and hand, specifically involving the carpus, represent a unique and often underappreciated subset of orthopedic trauma. While fractures of the distal radius and forearm are ubiquitous in pediatric practice, isolated carpal fractures remain exceedingly rare. This rarity is primarily attributed to the unique biomechanical properties of the immature skeleton. The adjacent physis of the distal radius is among the most commonly injured structures in the pediatric upper extremity; paradoxically, this vulnerability is highly protective of the carpus. As axial and bending loads are transmitted through the hand and wrist, the energy is diffused and ultimately absorbed by the biomechanically weaker distal radial physis, resulting in a Salter-Harris fracture rather than a carpal disruption. Consequently, true pediatric carpal injuries account for less than 1% of all pediatric fractures.
Despite their rarity, the true incidence of pediatric carpal injuries is likely underestimated due to a combination of clinical and radiographic diagnostic challenges. Examining an acutely injured, agitated child is inherently difficult, and localizing tenderness specifically to the carpus rather than the adjacent distal radius requires meticulous clinical acumen. Furthermore, the limited ability of standard plain radiographs to detail the largely cartilaginous immature skeleton often leads to missed diagnoses. Occult fractures of the cartilaginous anlage may not manifest on initial plain films, leading to a misdiagnosis of a "wrist sprain." High clinical suspicion must be maintained, as delayed diagnosis can lead to profound long-term morbidity, including nonunion, malunion, and progressive carpal collapse.
The epidemiology of these injuries shifts dramatically as the child matures. In the first decade of life, the abundant cartilaginous envelope surrounding the ossific nuclei provides a highly resilient, shock-absorbing cushion that effectively dissipates traumatic forces. However, as the child enters adolescence, a "critical bone-to-cartilage ratio" is reached. The expanding ossific nuclei replace the resilient cartilage, rendering the carpal bones more brittle and susceptible to fracture under similar loading conditions. Consequently, the peak incidence of carpal fractures, particularly of the scaphoid, occurs at approximately 15 years of age, closely mirroring the injury patterns observed in the adult population.
Understanding the mechanisms of injury is critical for accurate diagnosis. In younger children, the most common mechanism of carpal injury is direct, blunt trauma to the wrist, such as a crush injury or a direct blow. Conversely, indirect injuries typically result from falls onto an outstretched hand (FOOSH), generating a massive axial compressive force with the wrist in forceful hyperextension. Because the pediatric distal radius typically fails first under these conditions, a carpal fracture resulting from a FOOSH in a child usually implies a significantly higher energy mechanism than in an adult, such as falling from a moving bicycle, a motorized vehicle accident, or a fall from a significant height.
Detailed Surgical Anatomy and Biomechanics
Ossification Sequence and Chondral Envelope
The embryologic and developmental anatomy of the pediatric carpus dictates both its radiographic appearance and its biomechanical resilience. The cartilaginous anlage of the wrist initially begins as a single, undifferentiated mesenchymal mass. By the 10th week of gestation, this mass undergoes programmed segmentation and transforms into eight distinct cartilaginous masses, each precisely contoured to match the morphology of its respective mature carpal bone. At birth, the carpus is entirely cartilaginous and radiolucent, making radiographic evaluation of neonatal and infant wrist injuries virtually impossible without advanced imaging modalities such as ultrasonography or magnetic resonance imaging (MRI).
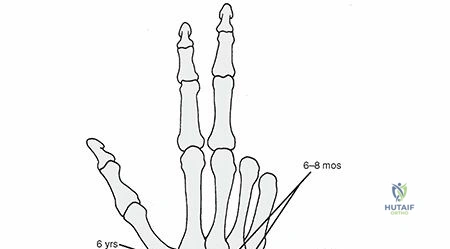

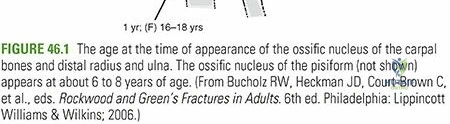
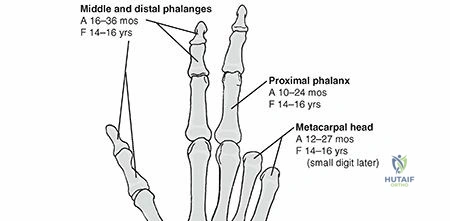
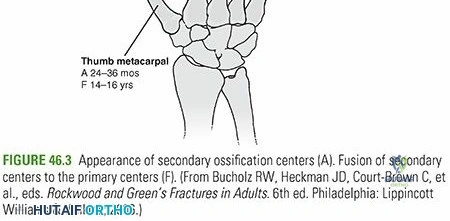
The appearance of the ossification centers within these cartilaginous shells follows a highly predictable, sequential timeline, which is a critical tool for the pediatric orthopedic surgeon in determining skeletal age and recognizing pathologic deviations. Ossification typically begins centrally within each cartilaginous mass and expands peripherally. The sequence is remarkably consistent: the capitate is the first to ossify at approximately 6 months of age, followed by the hamate, triquetrum, lunate, scaphoid, trapezium, trapezoid, and finally the pisiform, which may not ossify until 8 to 12 years of age. This sequential ossification means that at any given point during childhood, the radiographic size of a carpal bone dramatically underestimates its true anatomic volume.
The unique structural configuration of the immature carpal bone—an expanding ossific nucleus surrounded by a thick, resilient cartilaginous envelope—provides profound protection against fracture. The cartilage acts as a viscoelastic shock absorber, deforming under load and returning to its original shape, thereby shielding the central woven bone from critical stress concentrations. However, this same cartilaginous envelope is entirely dependent on diffusion for its nutritional supply, making severe crush injuries particularly devastating, as they can cause irreversible chondrocyte necrosis and subsequent growth arrest or deformity of the developing carpal bone.
Biomechanical Load Transmission
The biomechanics of the pediatric wrist involve a complex interplay between the carpal bones, the intrinsic and extrinsic ligamentous stabilizers, and the adjacent physes. Load transmission across the wrist joint is not uniform; approximately 80% of an axial load is transmitted through the radiocarpal joint (primarily the scaphoid and lunate fossae), while the remaining 20% passes through the ulnocarpal space via the triangular fibrocartilage complex (TFCC). In the pediatric patient, the thick articular cartilage of the radiocarpal and midcarpal joints further diffuses these loads, preventing point-loading on any single ossific nucleus.
When the wrist is subjected to hyperextension, such as during a fall, the palmar extrinsic ligaments (e.g., the radioscaphocapitate and long radiolunate ligaments) become taut. In an adult, this tension often leads to a scaphoid fracture or a perilunate dislocation. In a child, however, the ligaments are biomechanically stronger than the cartilaginous anlage and the distal radial physis. Therefore, the force is transmitted proximally, leading to a distal radius physeal fracture or a metaphyseal buckle fracture. It is only when the critical bone-to-cartilage ratio is surpassed in adolescence that the scaphoid becomes the weak link in this biomechanical chain.
Furthermore, the specific vascular anatomy of the carpal bones plays a pivotal role in their biomechanical vulnerability to osteonecrosis following trauma. The scaphoid, for example, receives its primary blood supply from branches of the radial artery that enter via the dorsal ridge and flow in a retrograde fashion to the proximal pole. Even in the pediatric population, a fracture through the waist or proximal pole of the scaphoid disrupts this tenuous intraosseous vascular network, placing the proximal fragment at an exceptionally high risk for avascular necrosis (AVN) and subsequent structural collapse.
Exhaustive Indications and Contraindications
The decision-making process for operative versus non-operative management of pediatric carpal fractures requires a nuanced understanding of the child's skeletal maturity, fracture displacement, and the specific carpal bone involved. The overarching goal is to achieve anatomic restoration of the articular surfaces and preserve the delicate vascular supply to the ossific nuclei, thereby preventing long-term sequelae such as nonunion, osteonecrosis, and carpal instability.
Non-operative management is the mainstay for the vast majority of pediatric carpal fractures. Stable, non-displaced fractures of the scaphoid, triquetrum, trapezium, and trapezoid typically heal uneventfully with appropriate cast immobilization. The robust osteogenic potential of the pediatric periosteum and the rich vascularity of the surrounding soft tissues facilitate rapid union. A brief period of immobilization (typically 4 to 8 weeks, depending on the bone) in a well-molded cast is usually sufficient. Even in cases where a fracture is suspected clinically but occult radiographically, a conservative approach with a 2-week period of immobilization followed by clinical and radiographic re-evaluation is strongly indicated.
Operative intervention is reserved for specific, high-risk scenarios. Absolute indications for surgery include open fractures, fractures associated with acute neurovascular compromise (such as acute carpal tunnel syndrome secondary to a displaced lunate or hamate fracture), and severely displaced fractures that disrupt the congruent arcs of the carpus. For scaphoid fractures, surgical fixation is indicated for displacement greater than 1 mm, angulation greater than 10 degrees (intrascaphoid angle >35 degrees), or proximal pole fractures, due to the unacceptably high risk of nonunion and osteonecrosis. Additionally, adolescent athletes nearing skeletal maturity may be candidates for percutaneous fixation of minimally displaced scaphoid fractures to expedite healing and facilitate an earlier return to play.
Contraindications to operative intervention must be carefully weighed. Active local infection, severe soft tissue compromise that precludes safe surgical incisions, and medical comorbidities making anesthesia unacceptably risky are standard absolute contraindications. Relative contraindications include highly comminuted, non-displaced fractures where surgical hardware might further fragment the ossific nucleus, or very young patients (under 8 years old) where the target bone is predominantly cartilaginous, making rigid internal fixation technically impossible and potentially destructive to the developing anlage.
| Indication/Contraindication Parameter | Operative Management | Non-Operative Management |
|---|---|---|
| Scaphoid Displacement | > 1 mm step-off or gap | < 1 mm, anatomically aligned |
| Scaphoid Angulation | > 10 degrees intrascaphoid angulation | < 10 degrees, normal carpal alignment |
| Fracture Location (Scaphoid) | Proximal pole, unstable waist | Distal pole, stable waist |
| Lunate/Capitate | Displaced, greater arc injuries, rotational deformity | Non-displaced, incidental findings |
| Patient Age/Maturity | Adolescents (approaching adult bone morphology) | Young children (thick cartilaginous envelope) |
| Clinical Scenario | Open fracture, neurovascular compromise, delayed nonunion | Closed, neurovascularly intact, acute presentation |
Pre-Operative Planning, Templating, and Patient Positioning
Advanced Imaging Modalities
Meticulous pre-operative planning is the cornerstone of successful surgical management of pediatric carpal fractures. The diagnostic algorithm begins with high-quality, multi-planar plain radiography. Standard anteroposterior (AP) and lateral views of the wrist are mandatory but often insufficient due to the superimposition of the complex carpal anatomy and the radiolucency of the immature skeleton. Comparison views of the uninjured, contralateral wrist are invaluable in the pediatric population to differentiate subtle fractures from normal, irregular ossification centers or accessory ossicles.
When plain radiographs are equivocal but clinical suspicion remains high (e.g., persistent anatomic snuffbox tenderness), advanced imaging is imperative. Historically, technetium bone scanning was utilized; however, this has been entirely superseded by Magnetic Resonance Imaging (MRI). MRI is exquisitely sensitive for detecting occult trabecular microfractures, bone bruising, and disruptions of the cartilaginous envelope without exposing the child to ionizing radiation. Furthermore, MRI provides critical information regarding the integrity of the intrinsic interosseous ligaments (e.g., scapholunate, lunotriquetral) and the vascular status of the proximal scaphoid pole.
For complex, displaced fractures or fracture-dislocations (greater arc injuries), high-resolution Computed Tomography (CT) with 3D reconstructions is the gold standard for pre-operative templating. CT allows the surgeon to precisely map the fracture planes, quantify the degree of displacement and comminution, and select the appropriate trajectory and size for internal fixation devices. In the pediatric patient, minimizing radiation dose is critical, and CT protocols should be strictly optimized for the pediatric upper extremity.
Operating Room Setup and Patient Positioning
Proper operating room setup and patient positioning are critical to facilitate efficient and safe surgical intervention. The patient is typically placed supine on the operating table with the affected upper extremity extended onto a radiolucent hand table. General anesthesia is almost universally required for pediatric patients to ensure absolute immobility, though regional blocks (e.g., supraclavicular or axillary brachial plexus blocks) are highly recommended as adjuncts for profound intra-operative muscle relaxation and excellent post-operative pain control.
A well-padded pneumatic tourniquet is applied to the proximal arm to provide a bloodless surgical field, which is absolutely essential for identifying the delicate neurovascular structures and cartilaginous surfaces of the pediatric wrist. The tourniquet should be inflated to a pressure appropriate for the child's age and systolic blood pressure (typically 150-200 mmHg above systolic). Intra-operative fluoroscopy (mini-C-arm) is indispensable and must be positioned such that the surgeon can obtain true AP, lateral, and oblique views of the carpus without compromising the sterile field.
Pre-operative templating should dictate the surgical inventory. For pediatric carpal fractures, the surgeon must have access to a wide array of fine fixation implants. This includes smooth Kirschner wires (0.035 to 0.062 inches) for temporary or definitive fixation, as well as pediatric-specific headless compression screws (ranging from 1.5 mm to 3.0 mm in diameter). The surgeon must meticulously plan the screw trajectory to ensure that the threads do not violate the adjacent radiocarpal or midcarpal articular surfaces, a task made significantly more challenging by the thick, radiolucent cartilaginous cap covering the ossific nucleus.
Step-by-Step Surgical Approach and Fixation Techniques by Carpal Bone
Scaphoid Fracture Management
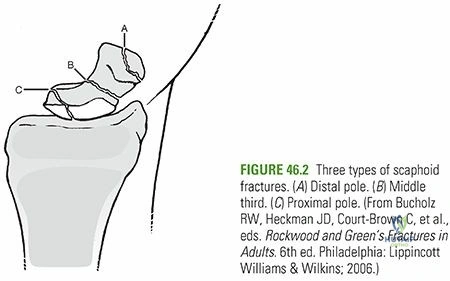
The scaphoid is the most commonly fractured carpal bone in the pediatric population, with a peak incidence at 15 years of age. Unlike adults, the most common mechanism in younger children is direct trauma, resulting in fractures of the distal third. Proximal pole fractures are exceedingly rare and typically result from severe mechanisms involving scapholunate ligament avulsion. Clinical evaluation classically reveals tenderness in the anatomic snuffbox and over the scaphoid tubercle volarly. Radiographic evaluation requires a dedicated "scaphoid series," including a posteroanterior (PA) view in ulnar deviation to elongate the scaphoid axis.
For displaced scaphoid fractures requiring operative intervention, the surgical approach is dictated by the fracture location. Distal pole and waist fractures are typically approached volarly (Russe approach) via an incision between the flexor carpi radialis (FCR) tendon and the radial artery. The radiocarpal capsule is incised longitudinally to expose the scaphoid. In children, care must be taken not to aggressively strip the volar ligaments, which provide critical vascularity. The fracture is reduced under direct vision using fine dental picks or small reduction forceps.

Fixation is typically achieved with a headless compression screw. A guide wire is placed from distal-volar to proximal-dorsal, aiming down the central axis of the scaphoid. In the immature skeleton, it is crucial to verify fluoroscopically that the wire is contained entirely within the ossific nucleus and does not breach the cartilaginous envelope. After measuring and drilling, the headless screw is advanced until it is buried beneath the articular cartilage. For proximal pole fractures, a dorsal approach is preferred. An incision is made over the Lister tubercle, the extensor pollicis longus is retracted, and the dorsal capsule is opened. This allows direct access to the proximal pole for antegrade screw placement.
Lunate and Triquetrum Fracture Management
Lunate fractures are extremely rare in children and almost exclusively result from severe, direct crush injuries. Clinical evaluation reveals diffuse volar wrist tenderness and profoundly painful range of motion. AP and lateral radiographs are often inadequate due to overlapping densities; thus, CT is the diagnostic modality of choice. Non-displaced lunate fractures are treated with short arm casting for 4 weeks. However, displaced or comminuted fractures require open reduction to restore the articular congruity and allow for the formation of vascular anastomoses, mitigating the risk of lunatomalacia (pediatric Kienböck's disease). The lunate can be approached dorsally or volarly depending on the displacement pattern, and fixation is typically achieved with multiple fine (0.035-inch) smooth K-wires, as the pediatric lunate is often too small to accommodate a compression screw.

Triquetrum fractures, while rare, are likely underdiagnosed due to their late ossification. The mechanism is typically direct trauma to the ulnar wrist or a forceful avulsion by the dorsal radiocarpal ligaments during extreme flexion. Dorsal chip fractures are the most common variant and are best visualized on a lateral or oblique radiograph. Treatment for these avulsion fractures is almost universally non-operative, utilizing an ulnar gutter splint or short arm cast for 2 to 4 weeks. Fractures of the triquetral body with significant displacement are exceedingly rare but may necessitate open reduction and internal fixation via a dorsal ulnar approach, utilizing K-wires or micro-screws to restore the integrity of the lunotriquetral and triquetrohamate articulations.
Trapezium, Trapezoid, Capitate, and Hamate Fracture Management
Fractures of the trapezium and trapezoid are extraordinarily rare. Trapezium fractures occur via axial loading of the adducted thumb, driving the first metacarpal base into the trapezium. Diagnosis requires a Robert view (true AP of the first carpometacarpal joint). While most are treated with thumb spica casting, severely displaced articular fractures require open reduction via a radiopalmar approach (Wagner incision) and fixation with K-wires or 1.5 mm screws to prevent early carpometacarpal arthrosis. Trapezoid fractures similarly result from axial loads through the second metacarpal and are managed with cast immobilization unless severely displaced, necessitating dorsal open reduction and K-wire fixation.


The capitate, despite being the largest carpal bone, is rarely fractured in isolation due to its protected, central position. It is more commonly injured as part of a greater arc injury pattern (transscaphoid, transcapitate perilunate fracture-dislocation) or naviculocapitate syndrome. Hyperdorsiflexion causes the capitate waist to impinge against the dorsal rim of the radius. Displaced capitate fractures require open reduction, typically via a dorsal approach, to prevent rotation of the proximal pole, which can lead to osteonecrosis and midcarpal collapse. Fixation is achieved with headless compression screws or K-wires.
Hamate fractures in the pediatric population are scarcely documented but typically involve direct trauma from racquet sports, softball, or golf. Patients present with hypothenar pain and potential ulnar neuropathy due to proximity to Guyon's canal. Routine radiographs are often unrevealing. The diagnosis of a hamate fracture can usually be made on the basis of the carpal tunnel view or computed tomography, which remains the gold standard for identifying fractures of the hook. Non-displaced fractures are casted; however, symptomatic nonunions of the hook of the hamate may require surgical excision of the fragment with careful protection of the ulnar nerve and artery.
Complications, Incidence Rates, and Salvage Management
Despite the robust healing potential of the pediatric skeleton, complications following carpal fractures can be profound and life-altering if not appropriately managed. The most significant complications stem from missed diagnoses, delayed treatment, or biological failures such as osteonecrosis. The pediatric orthopedic surgeon must be highly vigilant in monitoring for these adverse outcomes during the post-operative or post-injury period.
Delayed union and nonunion are rare in the pediatric population but do occur, particularly in scaphoid waist and proximal pole fractures that were initially missed or inadequately immobilized. A nonunion in a child alters the complex kinematics of the carpus, leading to a predictable pattern of degenerative changes akin to the SNAC (scaphoid nonunion advanced collapse) wrist seen in adults. Salvage management for a pediatric scaphoid nonunion typically requires operative debridement of the fibrous nonunion site and placement of a structural bone graft (often harvested from the distal radius or iliac crest) combined with rigid internal fixation using a compression screw or K-wires.
Osteonecrosis is perhaps the most devastating biological complication. It is extremely rare in the general pediatric population but becomes a significant risk in older adolescents with proximal pole scaphoid fractures or severe lunate crush injuries. Osteonecrosis of the lunate, referred to as "lunatomalacia" or pediatric Kienböck's disease, typically occurs in children under 10 years of age. Unlike the adult form, which often progresses to carpal collapse, pediatric lunatomalacia has a remarkable potential for spontaneous revascularization and remodeling. Symptoms are rarely dramatic, and radiography reveals mildly increased density of the lunate with no change in morphology. Treatment is conservative, consisting of prolonged immobilization (up to 1 year), which usually results in excellent functional and symptomatic recovery.
| Complication | Estimated Incidence (Pediatric) | Risk Factors | Salvage / Management Strategy |
|---|---|---|---|
| Delayed Union / Nonunion | < 5% (Scaphoid) | Missed diagnosis, proximal pole location, inadequate casting | Open debridement, structural autogenous bone grafting, rigid internal fixation. |
| Osteonecrosis (Scaphoid) | Exceedingly rare (< 1%) | Proximal pole fractures |
