Pediatric Sacral Fracture & Neurological Deficit: A Detailed Trauma Case Study

Key Takeaway
Pediatric sacral fractures with neurological deficits present with severe pain, lower extremity weakness, perineal numbness, and absent sacral reflexes. Diagnosis involves thorough clinical neurological examination, CT for fracture morphology, and MRI to confirm nerve root compression, edema, or hemorrhage, all crucial for guiding surgical decompression and stabilization planning.
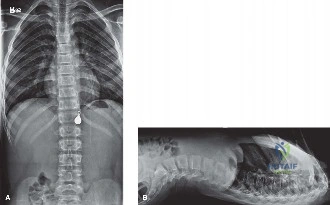
An 8-year-old child presents following a high-velocity road traffic accident. They have profound pelvic pain and neurological deficits, including urinary retention and perineal numbness. You have reviewed the imaging below.
Describe your immediate clinical assessment priorities and explain how you would classify this sacral injury.
Candidate: I would start with ATLS protocols to ensure hemodynamic stability. Neurologically, I need to perform a rectal exam to assess sphincter tone and the bulbocavernosus reflex. For the fracture, I would use the Denis classification system (Zones I-III). This appears to be a Zone III injury given the neurological deficit, indicating potential cauda equina compression.
Candidates often focus exclusively on the osseous fracture lines on the radiograph. They fail to prioritize the "Red Flag" clinical findings (sphincter tone, perianal sensation) that differentiate a stable fracture from a surgical emergency (cauda equina syndrome/sacral plexopathy).
A structured, high-scoring response: 1. Stabilization: Resuscitation and ATLS, ruling out concurrent life-threatening injuries. 2. Neurological Assessment: Emphasize the digital rectal exam (DRE) for S2-S4 function. 3. Classification: Define the injury using Denis (Zones I-III) and specifically check for Spino-pelvic dissociation using the Isler system (relationship to the L5-S1 facet joint). 4. Soft Tissue: Mention screening for Morel-Lavallée lesions, which are high-risk for infection if ignored.
The imaging and MRI confirm a displaced sacral fracture with neural element compression. You have decided on operative management. Describe your surgical planning, specifically regarding the fixation construct in this pediatric patient.
Candidate: I would perform a posterior midline approach for decompression. Because of the lumbopelvic instability, I would use a lumbopelvic fixation construct. This would involve pedicle screws in L4 and L5, connected to iliac screws to bypass the sacrum. I would also use neuromonitoring to track the S1-S3 roots.
Failing to mention the specific challenges of pediatric anatomy (cartilaginous models, growth plates) and omitting the requirement for 3D navigation or O-arm, which is now standard practice for the narrow and potentially dysmorphic pediatric sacral corridor.
A concise, professional plan: 1. Decompression: Wide laminectomy S1-S3, formal root decompression. 2. Fixation: Lumbopelvic construct (L4/L5 pedicle screws to iliac screws) for stability. 3. Safety: Mandatory use of Multimodality Neuromonitoring (SSEP/MEP/EMG) and intraoperative 3D imaging/navigation to ensure safe screw trajectories. 4. Considerations: Mentioning the need for subfascial drain and waterproof closure to mitigate the high risks associated with the posterior degloving environment.
