Pediatric Pelvic Fractures: Comprehensive Surgical Management

Key Takeaway
Pediatric pelvic fractures are rare, high-energy injuries often associated with severe multisystem trauma. Due to the inherent elasticity and remodeling potential of the immature pelvis, conservative management is typically successful. However, unstable ring disruptions, triradiate cartilage injuries, and mature pelvic fractures may necessitate operative intervention. This guide details the biomechanics, clinical evaluation, classification systems, and step-by-step surgical management of pediatric pelvic trauma.
Comprehensive Introduction and Patho-Epidemiology
Pediatric pelvic fractures represent a relatively rare but highly significant clinical entity in orthopedic traumatology, accounting for approximately 1% to 3% of all pediatric skeletal injuries. Unlike adult pelvic ring disruptions, which frequently occur from lower-energy mechanisms in osteoporotic bone or high-energy blunt force trauma, pediatric pelvic fractures are almost exclusively the result of massive energy transfer. The classic mechanism of injury involves a child acting as a pedestrian who is struck by a moving motor vehicle, though other high-energy etiologies such as falls from significant heights, crush injuries, and high-speed motor vehicle collisions are also prevalent. Because of the immense remodeling potential and inherent viscoelasticity of the immature skeleton, the vast majority of these fractures can be managed non-operatively with highly satisfactory long-term functional and radiographic outcomes. However, the paradigm of universally conservative management has shifted, recognizing that specific unstable patterns and injuries in near-skeletally mature adolescents demand aggressive surgical intervention to prevent lifelong disability.
The patho-epidemiology of pediatric pelvic fractures is inextricably linked to the severity of concomitant multisystem trauma. Because the pediatric pelvis is highly malleable, a force sufficient to fracture the pelvic ring has inevitably transmitted massive kinetic energy through the surrounding visceral, vascular, and neurologic structures. Consequently, the initial evaluation and resuscitation must strictly adhere to Advanced Trauma Life Support (ATLS) protocols. The overall mortality rate in children sustaining pelvic fractures is alarmingly high, ranging historically from 9% to 18%. However, landmark epidemiological analyses by Demetriades et al. and Silber and Flynn have definitively established that the mortality rate attributable to the pelvic fracture alone (i.e., exsanguinating retroperitoneal hemorrhage) is exceptionally low, ranging from 0% to 2.3%. Mortality in this demographic is almost exclusively driven by associated catastrophic injuries, most notably severe traumatic brain injuries (TBI), hollow viscus ruptures, and massive solid organ lacerations.
Understanding the correlation between pelvic fracture patterns and associated injuries is paramount for the treating orthopedic surgeon and the trauma team. Bond et al. established a critical, statistically significant correlation between the anatomical location and multiplicity of pelvic fractures and the probability of intra-abdominal injury requiring emergent laparotomy. Their data demonstrated a mere 1% probability of severe intra-abdominal injury for isolated pubic fractures, which escalates to a 15% probability for iliac wing or sacral fractures, and skyrockets to a 60% probability for multiple fractures disrupting the pelvic ring. Local adjacent injuries must also be meticulously ruled out; these include damage to major vascular conduits (e.g., internal iliac artery branches), voluminous retroperitoneal hemorrhage, rectal tears, and genitourinary trauma such as rupture of the posterior urethra or the bladder dome.
During the secondary survey, the orthopedic surgeon must be vigilant for pathognomonic physical signs indicative of severe pelvic trauma. The Destot sign, characterized by a large superficial hematoma forming beneath the inguinal ligament or within the scrotum or labia, suggests significant anterior ring disruption and hemorrhage. The Roux sign, defined as a measurable decrease in the distance from the greater trochanter to the pubic spine on the affected side, is highly indicative of a lateral compression fracture with internal rotation of the hemipelvis. Finally, the Earle sign involves the detection of a palpable bony prominence, a large hematoma, or severe tenderness on a digital rectal examination, mandating further investigation for an open pelvic fracture communicating with the rectal vault. Provocative maneuvers, such as posterior pressure on the iliac crests to assess for "open-book" instability or lateral-to-medial compression, should be performed gently and only once to elicit pain and crepitation without exacerbating retroperitoneal hemorrhage.
Detailed Surgical Anatomy and Biomechanics
The pediatric pelvis is not merely a miniature version of the adult pelvis; it possesses unique biomechanical, histological, and anatomical characteristics that directly dictate fracture patterns, energy absorption, and management algorithms. The osseous malleability of the pediatric pelvic bone is profound. Due to a lower mineral content, higher porosity, and a thicker, more osteogenic periosteum, the pediatric hemipelvis can undergo significant plastic deformation before reaching the point of catastrophic failure. The extensive cartilaginous structures, particularly the symphysis pubis and the sacroiliac (SI) joints, exhibit significantly greater elasticity than their adult counterparts.
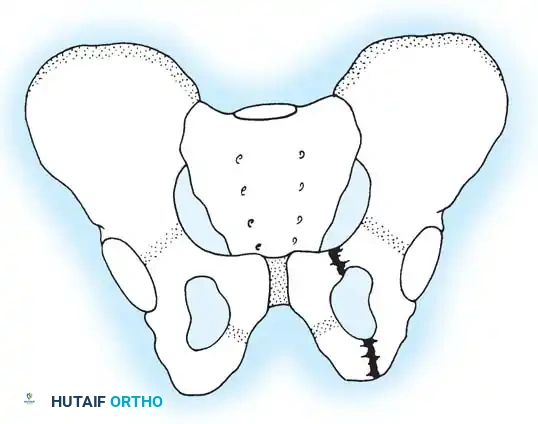
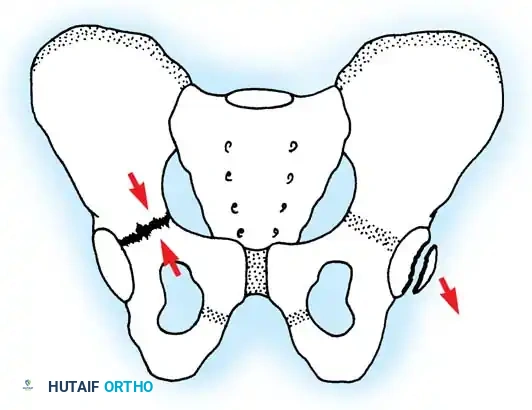
This hyper-elasticity allows for substantial displacement and deformation, frequently resulting in a fracture in only one area of the ring. This single-break phenomenon contrasts sharply with the traditional "double break" obligatory in rigid adult pelves (e.g., the classic Malgaigne fracture, which requires both an anterior and posterior disruption to displace). In children, the symphysis pubis can widen significantly, or the SI joint can stretch without tearing the robust anterior or posterior sacroiliac ligaments, allowing the kinetic energy to dissipate through a single osseous failure, typically the pubic rami.
Another critical anatomical distinction is apophyseal vulnerability. The cartilage at the apophyses (secondary centers of ossification) is inherently weaker than the adjacent ossified bone or the attaching musculotendinous units. Consequently, avulsion fractures occur with much higher frequency in children and adolescents, particularly athletic populations, due to sudden, violent muscle contractions against a fixed resistance.
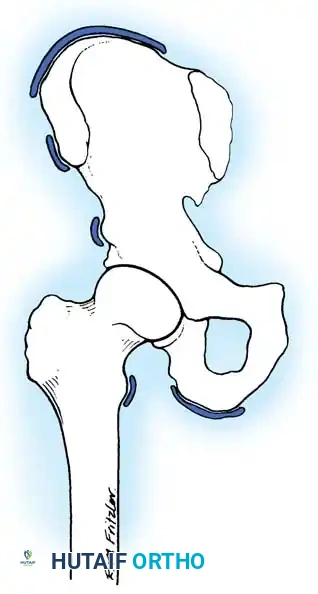
Common sites of apophyseal avulsion include the Anterior Superior Iliac Spine (ASIS) via the sartorius muscle, the Anterior Inferior Iliac Spine (AIIS) via the direct head of the rectus femoris, the ischial tuberosity via the hamstring complex, and the iliac crest via the abdominal musculature. These injuries, while acutely painful, rarely compromise the structural integrity of the pelvic ring.
The most critical anatomical structure unique to the pediatric pelvis is the triradiate cartilage. This Y-shaped physeal complex is the confluence of the ilium, ischium, and pubis within the acetabular fossa. It is responsible for the concentric expansion of the acetabulum during childhood growth. Fractures extending into the triradiate cartilage, particularly compression injuries that act as Salter-Harris Type V equivalents, can cause premature physeal closure and localized growth arrest. Because the femoral head continues to grow while the acetabulum ceases to expand concentrically, this complication inevitably results in a shallow, dysplastic acetabulum, lateral subluxation of the femoral head, and secondary leg-length inequality.
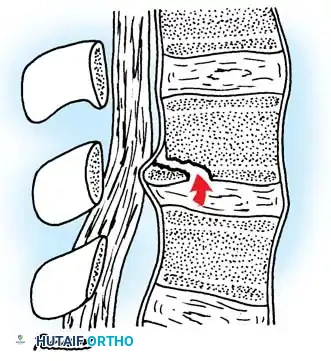
High-energy trauma can also result in complex injuries at the lumbosacral junction. Because of the elasticity of a child’s spine, forces are transmitted over many segments, sometimes resulting in posterior physeal injuries that can mimic a ruptured disc or cause nerve root compression.
Exhaustive Indications and Contraindications
The decision-making process for operative versus non-operative management of pediatric pelvic fractures is highly nuanced. It requires a delicate balance between respecting the immense remodeling potential of the immature skeleton and recognizing the severe functional deficits that arise from malunion in unstable or articular injuries. The orthopedic surgeon must base surgical indications on the physiological stability of the patient, the anatomical location of the fracture, the degree of displacement, and the skeletal maturity of the patient (specifically the status of the triradiate cartilage).
Operative intervention is definitively indicated in the setting of hemodynamic instability directly attributable to the pelvic ring disruption. Severe diastasis of the pubic symphysis or open-book pelvic fractures (Anteroposterior Compression Types II and III) can cause life-threatening retroperitoneal hemorrhage. While children vasoconstrict effectively and maintain blood pressure longer than adults, once their physiological reserve is depleted, they rapidly decompensate. Rapid reduction of pelvic volume via external fixation or pelvic binders is a life-saving indication. Furthermore, unstable pelvic ring disruptions (Torode and Zieg Type IV), such as vertical shear injuries or highly displaced Malgaigne fractures in older adolescents, require rigid internal fixation to prevent chronic pelvic pain, sitting imbalance, and severe leg-length discrepancies. Intra-articular displacement of the acetabulum greater than 2mm, particularly in weight-bearing domes, mandates Open Reduction and Internal Fixation (ORIF) to restore joint congruity and mitigate the risk of early-onset post-traumatic osteoarthritis.
Conversely, absolute and relative contraindications must be strictly observed. The most critical absolute contraindication to definitive pelvic ORIF is a physiologically exhausted patient exhibiting the "lethal triad" of trauma: severe coagulopathy, profound hypothermia, and metabolic acidosis. In such scenarios, the principles of Damage Control Orthopedics (DCO) must be employed. The surgeon should perform only rapid, life-saving interventions, such as the application of a pelvic external fixator or a supra-acetabular C-clamp, deferring definitive internal fixation until the patient has been adequately resuscitated in the Intensive Care Unit (ICU). Relative contraindications include undisplaced or minimally displaced fractures of the pubic rami or iliac wing, which will reliably heal with conservative management and protected weight-bearing.
| Clinical Scenario | Indications for Surgery | Contraindications for Surgery |
|---|---|---|
| Hemodynamic Status | Refractory hypotension due to pelvic venous/arterial bleeding (requires Ex-Fix or Packing). | Patient in extremis (lethal triad); definitive ORIF is strictly contraindicated (Perform DCO). |
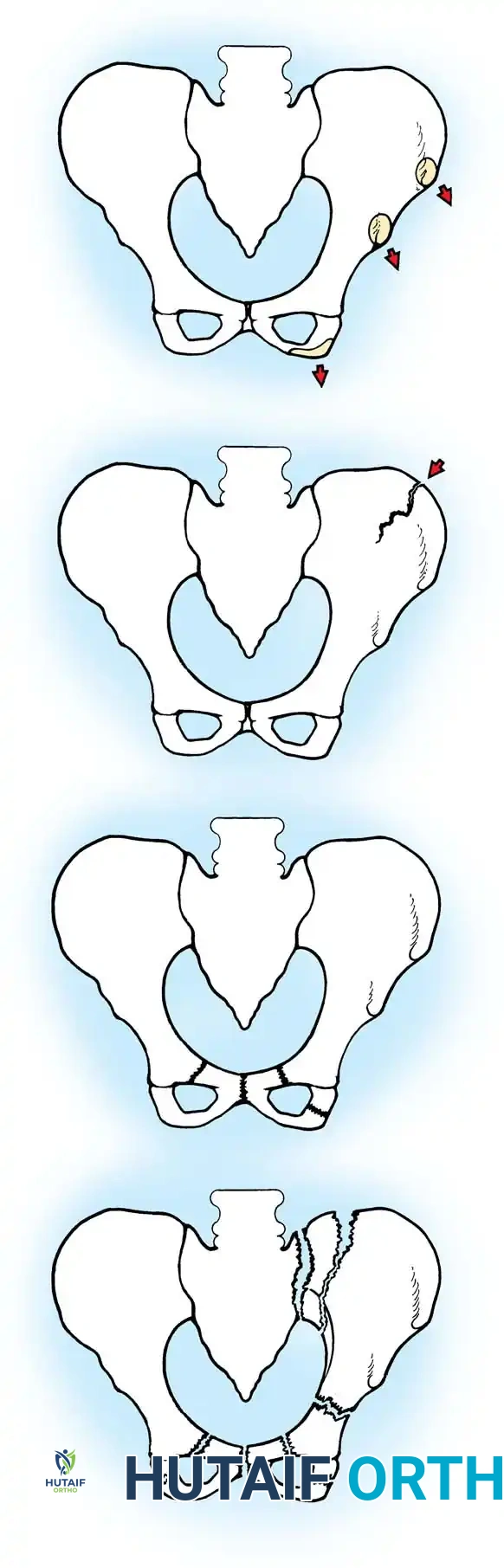
| Pelvic Ring Stability | Unstable Torode & Zieg Type IV (Vertical Shear, severe APC-III). | Stable Torode & Zieg Types I, II, and III (isolated rami, single breaks). |
| Acetabular Involvement | Intra-articular step-off > 2mm; incarcerated intra-articular fragments. | Undisplaced acetabular fractures; isolated triradiate compression without displacement. |
| Soft Tissue Envelope | Open pelvic fractures requiring emergent debridement and stabilization. | Severe local infection or massive soft tissue degloving over planned surgical incisions (Morel-Lavallée lesion) delaying ORIF. |
| Skeletal Maturity | Near-skeletally mature adolescents with displaced ring fractures. | Young children with massive remodeling potential and acceptable alignment. |
Pre-Operative Planning, Templating, and Patient Positioning
Meticulous pre-operative planning is the cornerstone of successful surgical execution in pediatric pelvic trauma. The diagnostic imaging cascade must begin with a high-quality anteroposterior (AP) radiograph of the pelvis, typically obtained in the trauma bay. If a pelvic ring disruption or acetabular fracture is identified, specialized fluoroscopic or radiographic views are mandatory. The Pelvic Inlet view (directed 45 degrees caudad) is critical for assessing anterior-posterior translation of the hemipelvis and rotational deformity. The Pelvic Outlet view (directed 45 degrees cephalad) is essential for evaluating vertical translation (cranial migration of the hemipelvis) and true sacral foraminal anatomy.
In the modern era of trauma management, fine-cut Computed Tomography (CT) scans with multi-planar reconstruction (MPR) and 3-dimensional (3D) rendering are the gold standard for pre-operative templating. CT imaging allows for the precise delineation of triradiate cartilage involvement, the identification of incarcerated osteochondral fragments within the hip joint, and the assessment of posterior ring instability (sacroiliac joint widening or sacral alar impaction).
Templating for percutaneous sacroiliac (SI) screws requires specific attention to the morphology of the upper sacrum. In pediatric and adolescent patients, the sacrum can frequently exhibit transitional anomalies or dysmorphism (e.g., a "non-recessed" or "mammillary" S1 body). The surgeon must utilize the CT scan to map the safe osseous corridors, measuring the available width and trajectory for 6.5mm or 7.3mm cannulated screws to avoid catastrophic iatrogenic injury to the L5 nerve root anteriorly or the S1 nerve root inferiorly.
Patient positioning is dictated by the planned surgical approach and the necessity for concurrent procedures by other surgical subspecialties. For anterior ring stabilization (external fixation or symphyseal plating) and percutaneous posterior ring fixation, the patient is positioned supine on a fully radiolucent Jackson table or a flat trauma table. A bump may be placed under the lumbosacral junction to accentuate the pelvic inlet and outlet views for the C-arm. The patient must be prepped and draped widely, from the nipple line to the bilateral knees, allowing for a simultaneous exploratory laparotomy by general surgery if required, as well as access to the lower extremities for traction. If an open posterior approach is necessitated for a severely displaced sacral fracture or an irreducible SI joint dislocation, the patient is carefully log-rolled into the prone position, ensuring all pressure points are meticulously padded and the abdomen hangs free to decrease venous pressure and minimize epidural bleeding.
Step-by-Step Surgical Approach and Fixation Technique
The surgical execution of pediatric pelvic fracture management ranges from rapid, minimally invasive external fixation to complex, multi-incisional open reduction and internal fixation. The choice of technique is dictated by the patient's physiological status and the specific fracture morphology.
Application of Pelvic External Fixator
External fixation remains the workhorse for acute, hemodynamically unstable "open-book" fractures in children. It rapidly reduces pelvic volume, promoting the tamponade of retroperitoneal venous bleeding.
The supra-acetabular corridor is biomechanically superior to the iliac crest and is preferred in older children and adolescents.
1. Incision and Dissection: A 1-2 cm longitudinal incision is made slightly distal and medial to the Anterior Superior Iliac Spine (ASIS), targeting the Anterior Inferior Iliac Spine (AIIS). Blunt dissection is performed between the sartorius and the direct head of the rectus femoris, carefully protecting the Lateral Femoral Cutaneous Nerve (LFCN).
2. Guidewire Placement: Under fluoroscopic guidance (utilizing Obturator Oblique Outlet and Iliac Oblique Inlet views), a drill guide is placed on the AIIS. A guidewire is advanced from the AIIS toward the Posterior Superior Iliac Spine (PSIS). The surgeon must stay strictly within the dense osseous corridor above the sciatic notch, avoiding intra-articular penetration of the hip joint.
3. Pin Insertion: Over the guidewire, 4.5 mm or 5.0 mm Schanz pins are inserted into the dense supra-acetabular bone.
4. Reduction and Frame Assembly: The pins are connected with a carbon fiber rod system. Manual internal rotation compression forces are applied to the trochanters or the pins themselves to close the symphyseal diastasis. The reduction is confirmed fluoroscopically, and the frame is locked. The surgeon must ensure the connecting bars do not compress the abdomen, preventing secondary abdominal compartment syndrome.
Open Reduction and Internal Fixation (ORIF) of the Anterior Ring
In older adolescents with closed triradiate cartilages and unstable Type IV ring disruptions, ORIF of the symphysis pubis is indicated.
1. Approach: A transverse Pfannenstiel incision is utilized, positioned 2 fingerbreadths superior to the symphysis pubis. The anterior rectus sheath is incised, and the rectus abdominis muscles are split linearly along the linea alba.
2. Exposure: The retropubic space (Space of Retzius) is exposed. The surgeon must be acutely aware of the "corona mortis," a vascular anastomosis between the external iliac and obturator vessels crossing the superior pubic ramus, which can cause massive hemorrhage if inadvertently lacerated.
3. Reduction and Fixation: A pelvic reduction forceps (Weber clamp) or a Jungbluth clamp is placed on the superior pubic rami to anatomically reduce the symphysis. A multi-hole symphyseal plate (typically a 3.5mm reconstruction or specific symphyseal plate) is contoured to the superior surface of the pubic ring and secured with bicortical screws. In children, periosteal stripping must be minimized to preserve osteogenic potential.
Percutaneous Sacroiliac (SI) Screw Fixation
For posterior ring instability, percutaneous SI screws provide excellent biomechanical stability with minimal soft tissue morbidity.
1. Imaging Setup: Perfect true lateral, pelvic inlet, and pelvic outlet fluoroscopic views of the sacrum are mandatory before any incision is made.
2. Guidewire Insertion: Through a stab incision over the lateral gluteal region, a guidewire is advanced from the lateral ilium, across the SI joint, and into the center of the S1 vertebral body. The lateral view ensures the wire is anterior to the spinal canal and posterior to the anterior sacral cortex. The inlet view ensures the wire is within the AP confines of the sacral body. The outlet view ensures the wire is superior to the S1 neural foramen.
3. Screw Placement: A cannulated, partially threaded 6.5mm or 7.3mm screw (with a washer) is inserted over the wire to provide compression across the SI joint. In cases of severe vertical shear, a fully threaded screw may be used as a position screw to prevent over-compression and iatrogenic nerve injury.
Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique and advanced perioperative care, the management of pediatric pelvic fractures carries a significant risk of severe complications. These complications can arise from the initial high-energy trauma itself or as iatrogenic sequelae of surgical intervention. The orthopedic surgeon must be prepared to identify and manage these issues promptly to prevent lifelong disability.
The most feared and uniquely pediatric complication is premature closure of the triradiate cartilage. This occurs primarily following severe crush injuries to the acetabulum (Salter-Harris Type V equivalents) or displaced intra-articular fractures. When the triradiate cartilage arrests prematurely, the acetabulum fails to expand concentrically, while the femoral head continues its normal growth trajectory. This mismatch inevitably leads to secondary acetabular dysplasia, progressive lateral subluxation of the hip, and early-onset osteoarthritis. Salvage management for this condition requires complex reconstructive pelvic osteotomies, such as the Salter innominate osteotomy, the Pemberton pericapsular osteotomy, or a Triple pelvic osteotomy, depending on the patient's age and the degree of dysplasia.
Neurologic injuries are also prevalent, particularly in unstable posterior ring disruptions and vertical shear fractures. The L5 nerve root, which drapes over the anterior sacral ala, and the S1 nerve root, which exits the S1 foramen, are highly vulnerable to traction injuries or direct compression from displaced sacral fragments. Iatrogenic injury during percutaneous SI screw placement is a catastrophic complication that demands immediate screw removal and potential open decompression.
Other complications include leg-length discrepancies resulting from malunion of vertical shear injuries, and massive heterotopic ossification or myositis ossificans following severe apophyseal avulsion fractures. Myositis ossificans near the ischial tuberosity can present as a rapidly expanding, painful mass that radiographically mimics Ewing sarcoma or acute osteomyelitis. If a symptomatic nonunion or massive callus restricts athletic activity, salvage management consists of delayed surgical excision of the fragment once the heterotopic bone has fully matured (typically 6 to 12 months post-injury).
| Complication | Estimated Incidence | Etiology / Risk Factors | Salvage Management / Intervention |
|---|---|---|---|
| Premature Triradiate Closure | 5% - 15% (in acetabular fx) | Crush injuries (SH-V); displaced intra-articular fractures. | Reconstructive pelvic osteotomies (Salter, Pemberton, Triple) for resulting dysplasia. |
| Neurologic Injury (L5/S1) | 10% - 20% (in posterior ring fx) | Traction from vertical shear; iatrogenic from SI screw misplacement. | Immediate removal of hardware if iatrogenic; AFO bracing for foot drop; nerve exploration if completely severed (rare). |
| Leg-Length Discrepancy | 5% - 10% | Malunion of vertical shear fractures; growth arrest of hemipelvis. | Shoe lifts for minor discrepancies (<2cm); epiphysiodesis of contralateral limb; limb lengthening procedures. |
| Myositis Ossificans | Variable (common in avulsions) | Severe hematoma formation following ischial or AIIS avulsions. | Rest, NSAIDs (Indomethacin); delayed surgical excision only after maturation (6-12 months). |
| Infection / Pin Tract Sepsis | 10% - 15% (with Ex-Fix) | Poor pin site hygiene; prolonged external fixation duration. | Aggressive local wound care; oral antibiotics; premature removal of pins and transition to internal fixation or bed rest. |
Phased Post-Operative Rehabilitation Protocols
The post-operative rehabilitation of a pediatric patient following a pelvic fracture is a protracted, highly structured process that demands close collaboration between the orthopedic surgeon, physical therapists, and the patient's family. The protocol is strictly dictated by the mechanical stability of the fixation achieved intraoperatively, the patient's overall physiological status, and the presence of concomitant multisystem injuries.
Phase 1: Acute Inpatient Management (Weeks 0 - 2)
Immediately following surgery, the primary goals are pain control, physiological stabilization, and the prevention of secondary complications such as deep vein thrombosis (DVT) and pulmonary complications. While routine chemical DVT prophylaxis is controversial in young children, it is highly recommended for post-pubertal adolescents with severe pelvic trauma and prolonged immobility. Patients managed with external fixators or ORIF are strictly restricted to bed rest or bed-to-wheelchair transfers. Weight-bearing on the affected extremities is strictly prohibited (Non-Weight-Bearing, NWB). For patients with external fixators, meticulous daily pin site care utilizing chlorhexidine or sterile saline solutions is mandatory to prevent superficial pin tract infections, which can rapidly progress to deep osteomyelitis or necessitate premature frame removal.
Phase 2: Subacute Mobilization and Early Healing (Weeks 2 - 6)
As the acute pain subsides and early soft callus begins to form, physical therapy focuses on maintaining joint mobility and preventing contractures. Passive and active-assisted range of motion exercises for the hips, knees, and ankles are initiated, provided they do not place stress on the pelvic ring constructs. Patients may be transitioned to Toe-Touch Weight-Bearing (TTWB) using crutches or a walker, depending on their upper extremity strength and cognitive ability to comply with restrictions. At the 6-week mark, clinical and radiographic evaluations are performed. If bridging callus is evident and the patient is non-tender over the fracture sites, external fixators
