Comprehensive Management of Pediatric Knee Dislocations and Proximal Tibial Fractures
Key Takeaway
Acute dislocations of the pediatric knee and proximal tibiofibular joint are exceedingly rare but carry significant morbidity, particularly regarding popliteal artery compromise. Management requires meticulous clinical evaluation, advanced imaging, and often surgical intervention for displaced physeal fractures. This guide details the biomechanics, classification systems, and step-by-step operative techniques for proximal tibial fractures, ensuring optimal outcomes and minimizing complications like angular deformity or ischemia.
Comprehensive Introduction and Patho-Epidemiology
Acute dislocations of the knee and the proximal tibiofibular joint are exceedingly rare in the pediatric population, presenting a unique diagnostic and therapeutic challenge for the orthopedic surgeon. Unlike the adult knee, where high-energy trauma typically results in catastrophic ligamentous failure and true tibiofemoral dislocation, the pediatric knee possesses a distinct biomechanical profile. In the skeletally immature patient, the robust ligaments and thick periosteal sleeve are biomechanically superior to the relatively weaker cartilaginous physes (growth plates) of the distal femur and proximal tibia. Consequently, what may clinically masquerade as a gross knee dislocation in a child or adolescent is, upon radiographic and intraoperative scrutiny, frequently a displaced physeal fracture equivalent. True ligamentous dislocations of the pediatric knee seldom require surgical reconstruction of the joint itself in the acute setting, as closed reduction is often highly successful, provided that the periarticular soft tissue envelope remains competent.
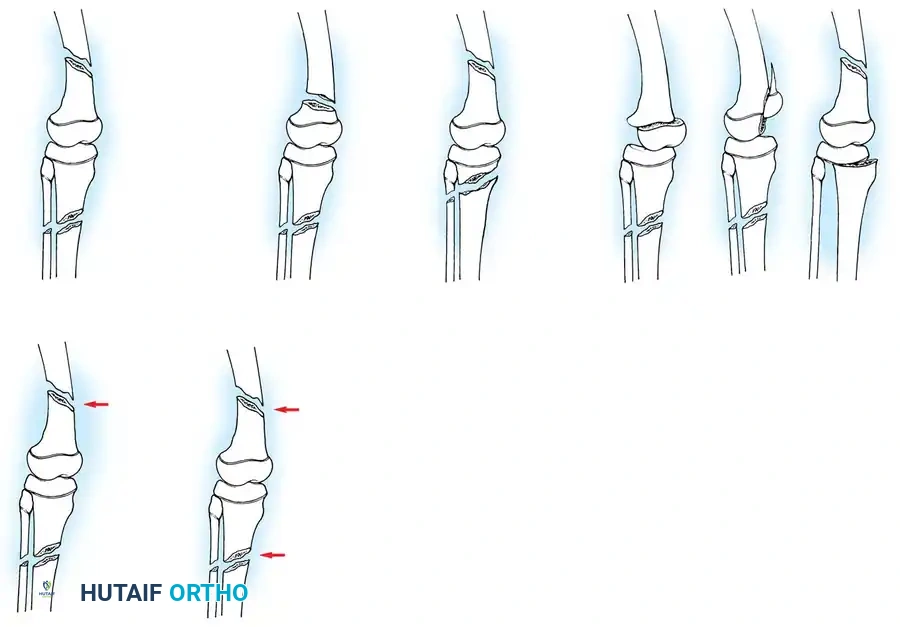
The primary clinical imperative when evaluating these high-energy injuries lies in accurately identifying the underlying pathological condition, recognizing subtle radiographic markers of physeal separation, and, most critically, ruling out limb-threatening vascular compromise. The popliteal artery is exceptionally vulnerable in this region due to its rigid anatomical tethering. Furthermore, these injuries frequently occur in the context of polytrauma, necessitating a multidisciplinary approach to patient resuscitation and stabilization. The incidence of proximal tibial physeal fractures accounts for less than 1% of all pediatric epiphyseal injuries, a statistic that underscores the necessity for heightened clinical vigilance. When these injuries do occur, they are typically the result of severe hyperextension or extreme valgus/varus bending moments applied to the knee, often sustained during motor vehicle collisions, high-impact sports, or falls from significant heights.
A particularly devastating variant of these high-energy trauma patterns is the "floating knee" injury, defined by ipsilateral fractures of the femoral and tibial shafts, which effectively uncouples the knee joint from the rest of the lower extremity kinematic chain. These flail extremities are universally associated with massive soft tissue trauma, high rates of open fractures, and profound systemic physiological derangement. The Letts classification (Types A through E) provides a critical framework for categorizing these injuries based on the presence of open wounds and the specific anatomical involvement of the diaphysis, metaphysis, or epiphysis. The management of the pediatric floating knee demands aggressive initial resuscitation, provisional stabilization (often via external fixation), and eventual definitive fixation tailored to the child's remaining growth potential and the condition of the soft tissue envelope.
The complexity of floating knee injuries is further delineated by the Bohn and Durbin classification system, which was subsequently modified by Arslan et al. to better capture the nuances of pediatric trauma. This system stratifies injuries from Type I (double shaft fractures) to Type IV (femur and/or tibia fractures at two distinct sites), with Type IIIb representing the most perilous pattern: simultaneous epiphyseal fractures of both the distal femur and proximal tibia. This specific pattern implies a massive transfer of energy directly across the joint line, exponentially increasing the risk of popliteal artery transection, common peroneal nerve palsy, and subsequent catastrophic growth arrest. The epidemiological data surrounding these complex patterns dictate that the treating orthopedic surgeon must maintain a low threshold for advanced vascular imaging and aggressive surgical intervention to preserve both the limb and its longitudinal growth capacity.
Detailed Surgical Anatomy and Biomechanics
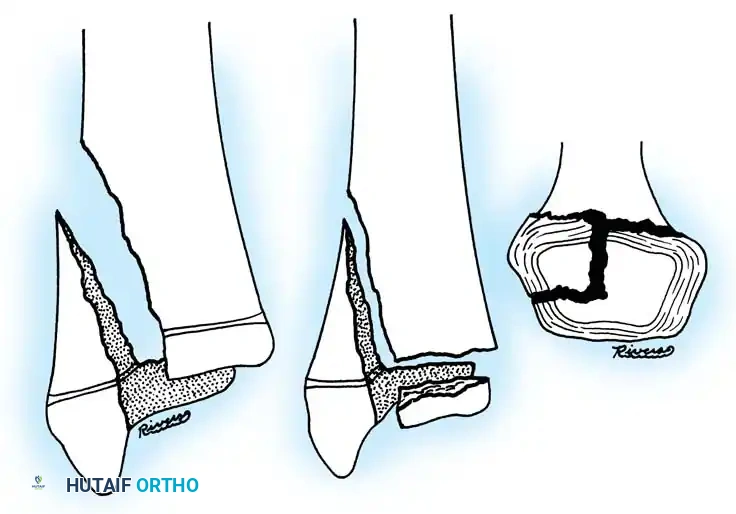
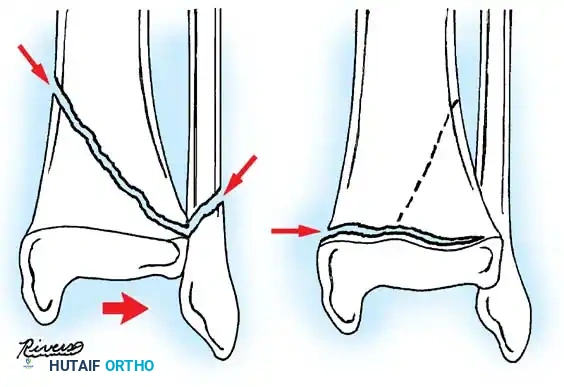
A profound understanding of the surgical anatomy and biomechanics of the pediatric knee is the cornerstone of successful management for proximal tibial and distal femoral injuries. The proximal tibial physis is a complex, undulating cartilaginous structure that contributes approximately 55% of the longitudinal growth of the tibia (averaging 6 mm per year). Anatomically, the proximal tibial epiphysis is unique because it encompasses not only the articular surface of the tibial plateau but also extends anteriorly and distally to include the tibial tuberosity apophysis. This anterior tongue of cartilage serves as the insertion site for the patellar tendon, making it a critical component of the extensor mechanism. During the transitional phase of skeletal maturation (typically ages 13 to 15), the physis begins to close in a highly predictable, asymmetric pattern—starting centrally, progressing posteromedially, and finally closing anterolaterally. This asymmetric closure pattern is the direct biomechanical catalyst for transitional fracture patterns, such as the triplane fracture of the proximal tibia.
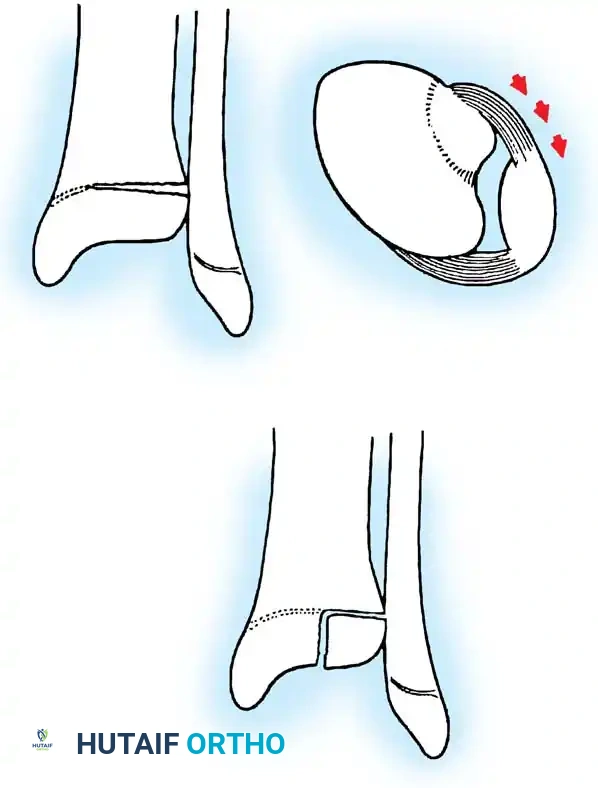
The ligamentous anatomy surrounding the pediatric knee dictates the pattern of failure under mechanical stress. In 1965, Aitken made the seminal observation that there are significantly fewer ligaments attaching directly to the proximal tibial epiphysis compared to the distal femoral epiphysis. Crucially, the superficial medial collateral ligament (MCL) originates on the distal femoral epiphysis but traverses the joint to insert distally onto the proximal tibial metaphysis, completely bypassing the proximal tibial physis. Similarly, the lateral collateral ligament (LCL) inserts onto the fibular head. Because these robust collateral ligaments bypass the tibial physis, valgus and varus stresses are transmitted directly to the metaphyseal bone rather than the physis itself. This anatomical quirk explains why distal femoral physeal separations are approximately eight times more common than their proximal tibial counterparts in major pediatric trauma registries.
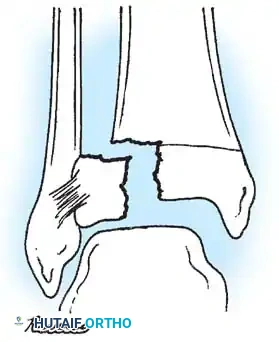
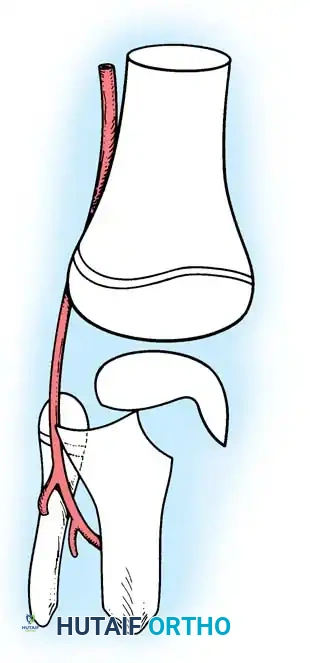
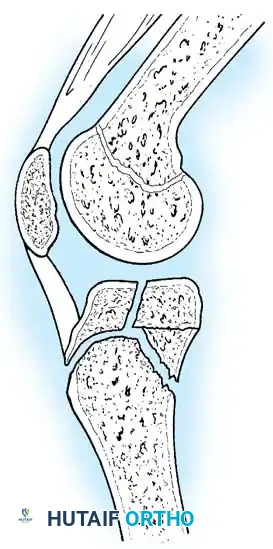
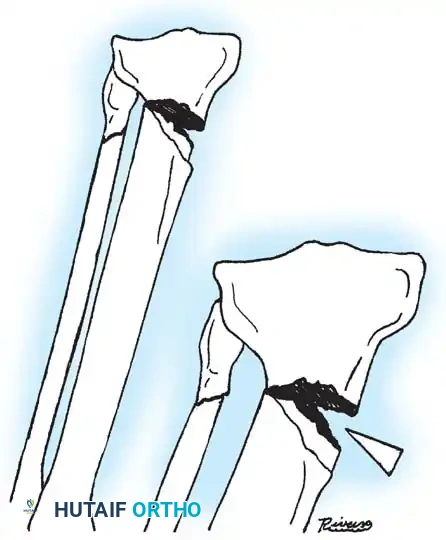
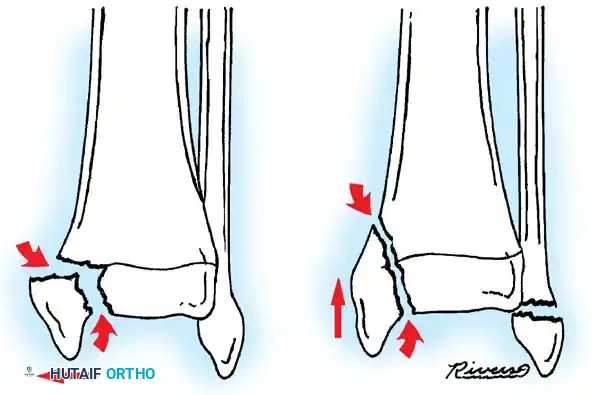
Vascular anatomy is arguably the most critical consideration in the acute management of these injuries. The popliteal artery descends through the popliteal fossa and is firmly tethered proximally by the adductor hiatus and distally by the fibrous arch of the soleus muscle (the soleal sling). Furthermore, the anterior tibial artery branches off the popliteal trifurcation and immediately passes anteriorly through the interosseous membrane. This rigid anatomical tethering renders the popliteal and anterior tibial arteries highly susceptible to traction, intimal tearing, thrombosis, or outright transection when the proximal tibial metaphysis is displaced posteriorly. In Salter-Harris Type I and II fractures with posterior displacement, the sharp metaphyseal ridge acts as a fulcrum over which the neurovascular bundle is stretched. Wozasek et al. documented that up to 13% of patients with proximal tibial physeal injuries exhibit signs of peripheral ischemia upon initial presentation, mandating immediate and aggressive vascular assessment.

Biomechanically, the pediatric periosteum plays a dual role in both the injury pattern and the subsequent surgical management. The periosteum in children is remarkably thick, osteogenic, and highly vascularized. During a displacement injury, the periosteum typically tears on the tension side of the fracture but remains intact on the compression side, acting as a robust hinge. While this intact periosteal hinge can aid in closed reduction maneuvers, the torn edges of the periosteum (along with the perichondrial ring of LaCroix) frequently become entrapped within the fracture site. This soft tissue interposition acts as a mechanical block to anatomic reduction, rendering the fracture irreducible by closed means and necessitating open surgical extraction. The surgeon must meticulously preserve the viable periosteal attachments during any open approach to maintain the vascular supply to the physeal and metaphyseal fragments, thereby mitigating the risk of avascular necrosis and subsequent growth arrest.
Exhaustive Indications and Contraindications
The decision-making process regarding operative versus non-operative management of pediatric knee dislocations and proximal tibial fractures requires a meticulous synthesis of fracture geometry, patient age, soft tissue integrity, and vascular status. The indications for surgical intervention are absolute in several clinical scenarios.
| Clinical Parameter | Indications for Surgical Intervention (ORIF/Ex-Fix) | Contraindications for Surgery (Favor Non-Operative) |
|---|---|---|
| Vascular Status | Absent pulses, ABI < 0.9, confirmed arterial injury on CTA. | Normal perfusion, palpable pulses, ABI > 0.9. |
| Fracture Displacement | Irreducible SH I/II, any displaced SH III/IV, >2mm articular step-off. | Non-displaced or minimally displaced SH I/II reducible via closed means. |
| Soft Tissue Envelope | Open fractures (Gustilo-Anderson I-III), compartment syndrome. | Intact skin, manageable swelling, absence of compartment tension. |
| Polytrauma Context | Floating knee injuries, severe head injury requiring rapid mobilization. | Isolated injury in a medically unstable patient unfit for anesthesia. |
| Joint Stability | Concomitant avulsion of cruciate/collateral ligaments causing gross instability. | Stable joint post-reduction in a long-leg cast. |
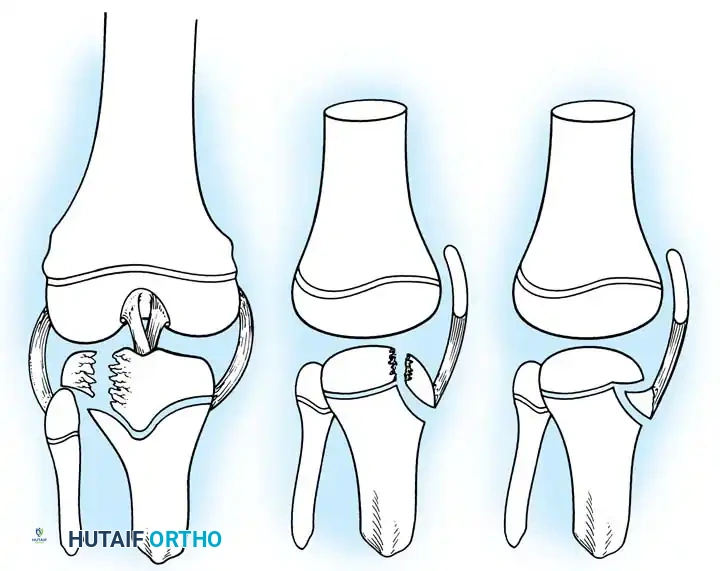
Operative intervention is strictly indicated when fractures are irreducible via closed means. As previously noted, this irreducibility is almost universally secondary to the interposition of the thick periosteal sleeve, the anterior horn of the medial or lateral meniscus, or the pes anserinus tendons into the physeal gap. Attempting forceful, repeated closed reductions in the face of soft tissue interposition is not only futile but highly deleterious, as it exacerbates damage to the delicate resting zone of the physis, exponentially increasing the risk of premature physeal closure. Furthermore, any Salter-Harris Type III or IV fracture with greater than 2 millimeters of articular step-off or physeal widening demands Open Reduction and Internal Fixation (ORIF). Anatomic restoration of the articular surface is mandatory to prevent early-onset post-traumatic osteoarthritis, while precise realignment of the physeal columns is required to minimize the risk of osseous bar formation.
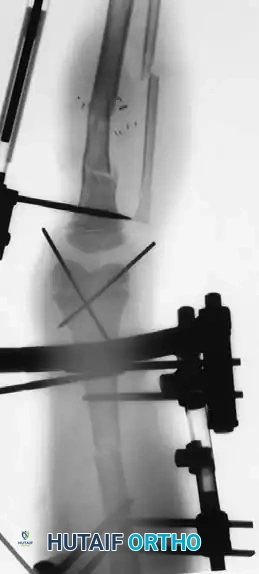
Absolute indications for emergent surgical exploration include any evidence of vascular compromise or impending compartment syndrome. A pulseless extremity that does not immediately respond to gentle realignment of the fracture requires urgent coordination with vascular surgery. If an arterial repair or bypass is necessary, the orthopedic surgeon must rapidly provide rigid skeletal stabilization—typically via a spanning external fixator or rigid internal fixation—prior to the vascular anastomosis to protect the repair. Similarly, the presence of tense, non-compressible compartments, severe pain out of proportion to the injury, or pain with passive stretch of the toes mandates emergent four-compartment fasciotomies of the lower leg. The threshold for fasciotomy should be exceedingly low in the setting of displaced proximal tibial fractures, given the high energy of the injury and the constrained nature of the fascial compartments.
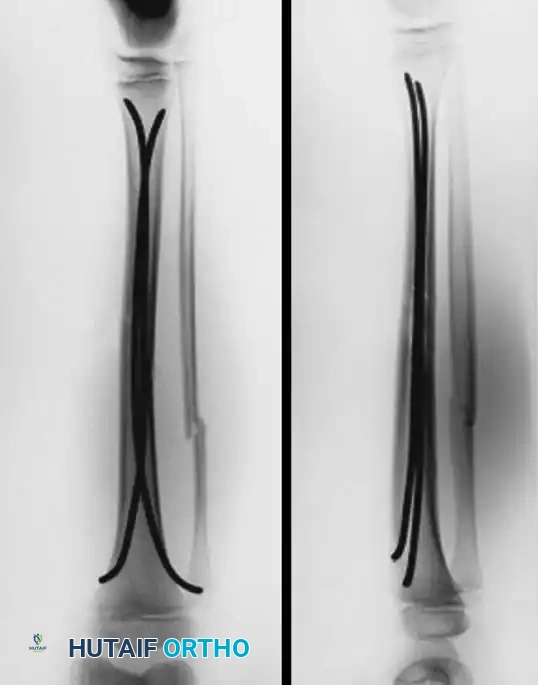
Conversely, contraindications to surgical intervention are primarily limited to non-displaced or minimally displaced Salter-Harris Type I and II fractures that can be concentrically reduced and stably maintained in a well-molded, long-leg cast. Additionally, surgical intervention may be temporarily contraindicated in the hemodynamically unstable polytrauma patient who cannot tolerate a prolonged anesthetic. In such damage-control orthopedics (DCO) scenarios, rapid application of a spanning knee external fixator is the treatment of choice, deferring definitive ORIF until the patient's physiological parameters have normalized. It is also critical to recognize that over-zealous surgical dissection in an attempt to achieve perfect radiographic alignment in a highly comminuted metaphyseal fracture can devascularize bone fragments and lead to nonunion; in these cases, biological fixation principles utilizing submuscular plating or elastic stable intramedullary nailing (ESIN) are preferred over extensive open approaches.
Pre-Operative Planning, Templating, and Patient Positioning
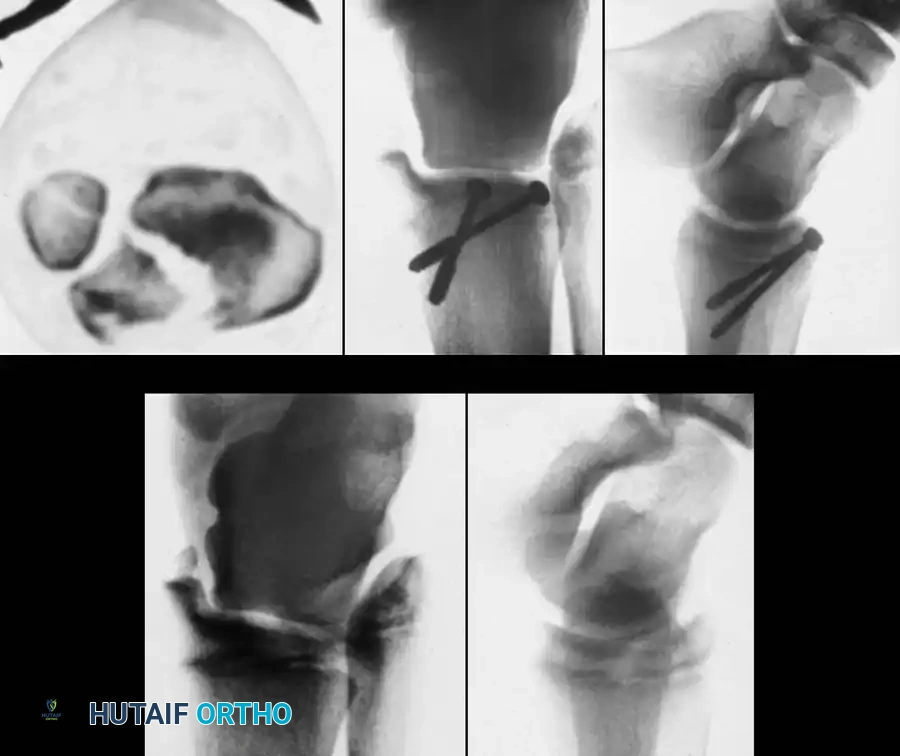
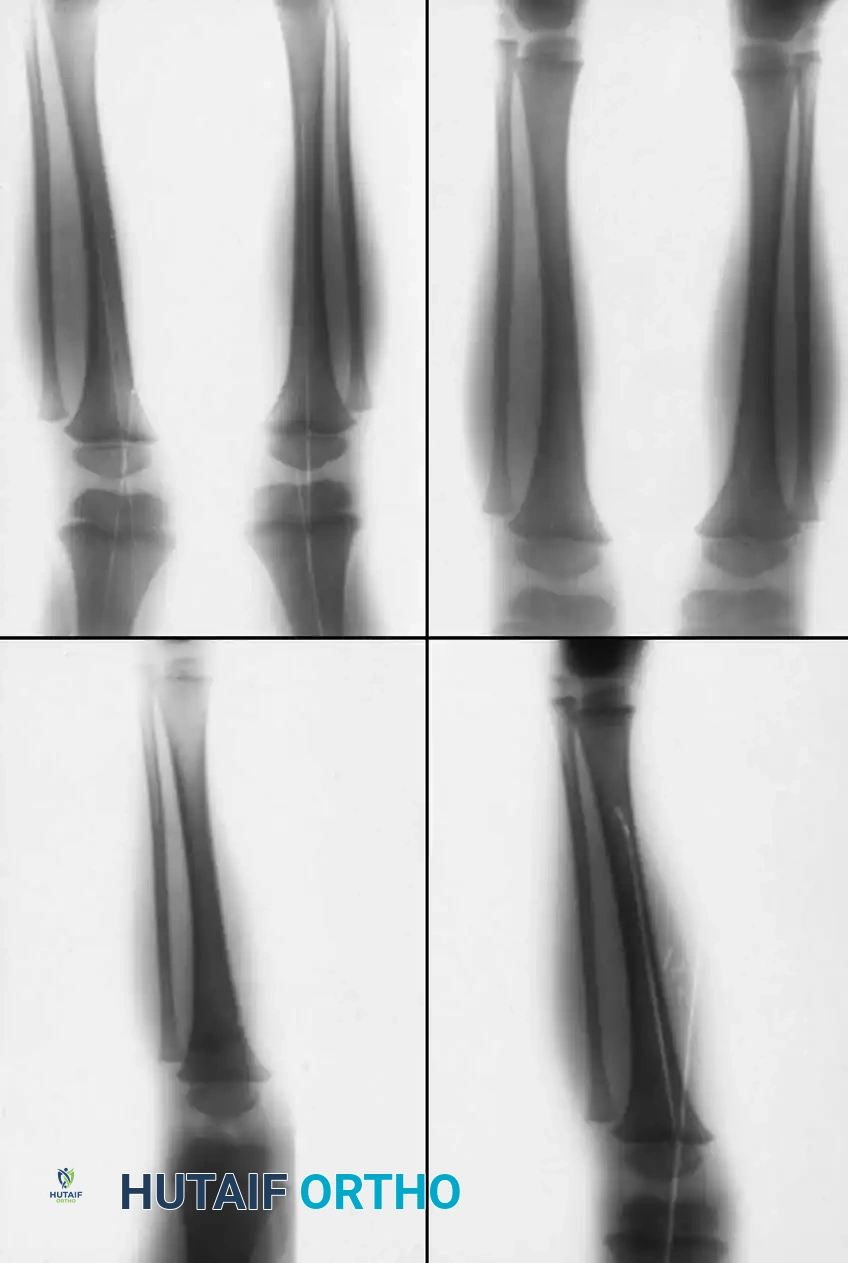
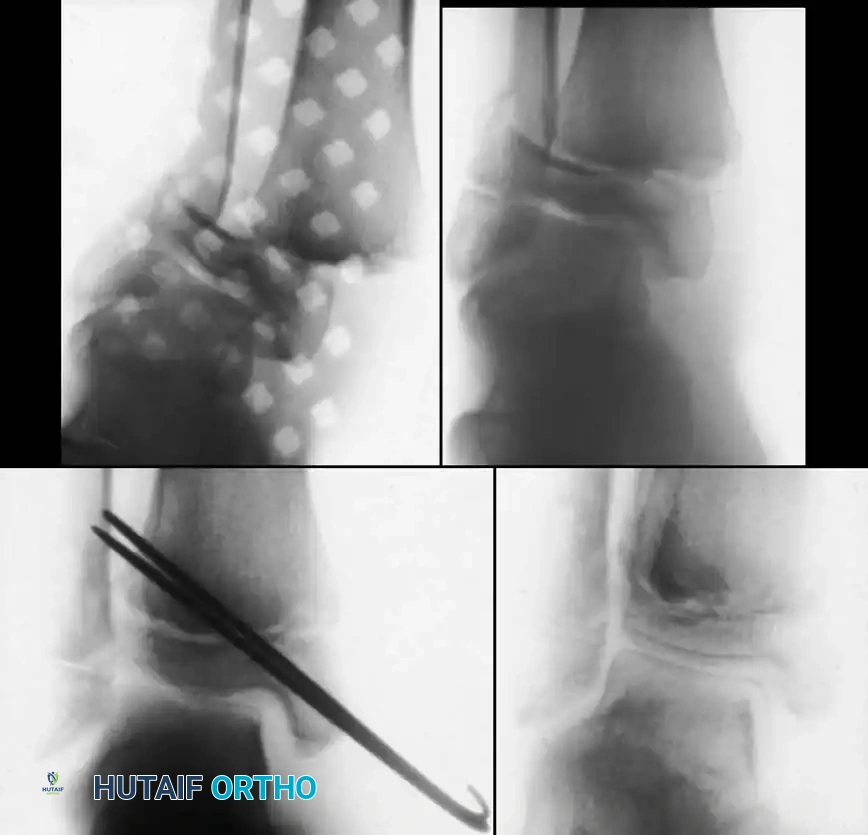
Thorough pre-operative planning is the bedrock of successful surgical execution in complex pediatric periarticular trauma. Plain radiographs, including true anteroposterior, lateral, and bilateral oblique views, are the initial standard; however, they frequently underestimate the true severity of physeal displacement and articular comminution. For any suspected Salter-Harris Type III, Type IV, or transitional triplane fracture of the proximal tibia, advanced cross-sectional imaging is mandatory. A fine-cut Computed Tomography (CT) scan with sagittal, coronal, and 3D surface-rendered reconstructions allows the surgeon to map the exact fracture geometry, identify the location of the metaphyseal spike, and quantify the degree of articular step-off. This imaging is crucial for determining the optimal surgical trajectory for screw placement, ensuring that fixation vectors remain parallel to the physis in younger children to prevent iatrogenic growth arrest.
In the setting of high-energy trauma with significant posterior displacement of the tibial shaft, pre-operative vascular templating is as critical as osseous templating. If the Ankle-Brachial Index (ABI) is less than 0.9, or if there are asymmetric pulses, a CT Angiogram (CTA) should be obtained immediately, provided it does not delay limb-saving intervention. The CTA will delineate the exact level of arterial injury—whether it is a traction-induced intimal flap, an in-situ thrombosis, or a complete transection at the level of the soleal sling. The surgical team must be prepared for a combined orthopedic and vascular procedure, ensuring that appropriate vascular instruments, shunts, and vein harvest sites are prepped and available in the operating theater.
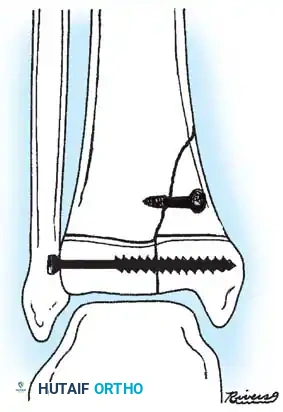
Pre-operative templating of hardware must account for the child's remaining growth potential. In the skeletally immature patient with open physes, the surgeon must plan for fixation that avoids crossing the physis whenever possible. If transphyseal fixation is unavoidable for stability, smooth, unthreaded Kirschner wires (K-wires) of the smallest effective diameter should be selected, and they should cross the center of the physis at an angle as close to 90 degrees as possible to minimize the cross-sectional area of physeal damage. In older adolescents nearing skeletal maturity (e.g., girls >14 years, boys >16 years), the risk of clinically significant growth arrest is negligible. In these patients, the surgeon should template for rigid interfragmentary compression utilizing 4.0mm or 4.5mm partially threaded cannulated cancellous screws to achieve absolute stability and facilitate early range of motion.
Patient positioning in the operating room must facilitate unhindered fluoroscopic access and the ability to manipulate the limb through a full range of motion. The patient is positioned supine on a fully radiolucent Jackson or OSI flat table. A bump is placed under the ipsilateral hip to correct natural external rotation, ensuring that the patella points directly toward the ceiling. A high thigh tourniquet is applied over copious padding. The entire lower extremity, from the tourniquet to the toes, is prepped and draped free. A sterile tourniquet may be utilized if proximal extension of the incision is anticipated. The C-arm fluoroscopy unit should be brought in from the contralateral side, allowing the surgeon unimpeded access to the medial and lateral aspects of the knee. Prior to incision, the surgeon must confirm that perfect AP and lateral fluoroscopic images can be obtained without interference from the table or the contralateral leg.
Step-by-Step Surgical Approach and Fixation Technique
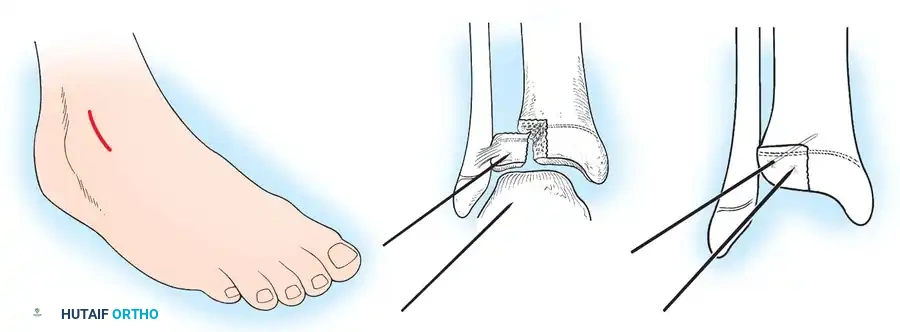
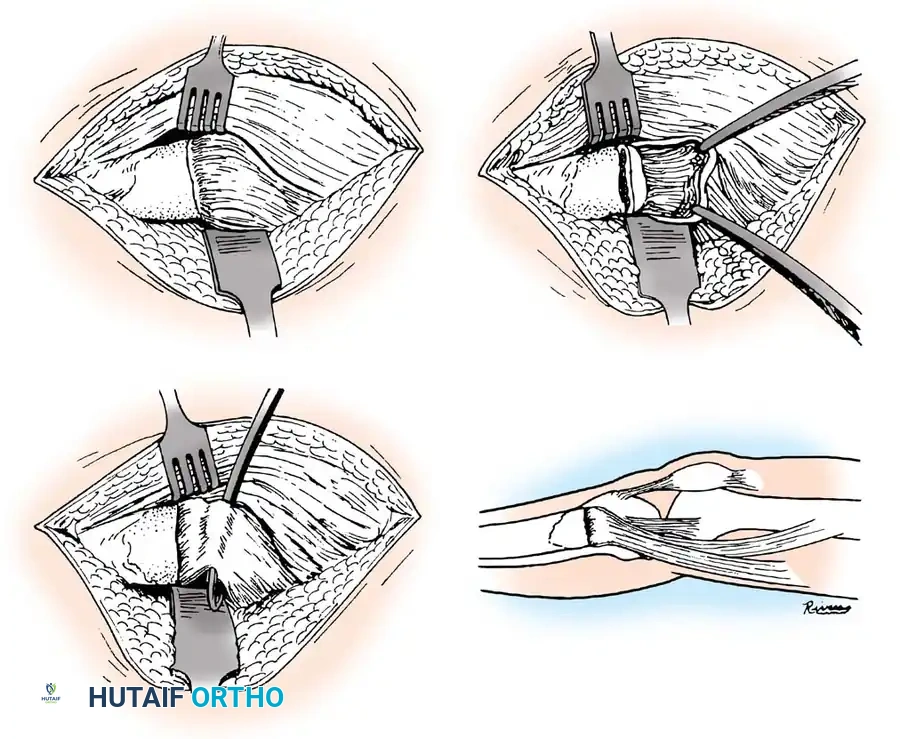
When displacement dictates surgical intervention, meticulous handling of the soft tissues and anatomic restoration of the articular surface are paramount. The surgical approach is dictated by the primary location of the fracture line and the anticipated trajectory of fixation. For most Salter-Harris III and IV injuries, including the massive tongue-type fractures of the tibial tuberosity, a longitudinal medial or lateral parapatellar approach is utilized. The incision is carried through the skin and subcutaneous tissues, maintaining full-thickness flaps to preserve the tenuous vascularity of the anterior skin envelope. The anterior tibial recurrent artery and the anterior compartment musculature are in close proximity to the lateral aspect of the tuberosity; excessive lateral dissection must be strictly avoided to prevent devascularization of the fragment or iatrogenic compartment syndrome.
Once the fracture site is exposed, the first critical step is the evacuation of the fracture hematoma and the meticulous debridement of interposed soft tissues. In tongue-type Salter-Harris III injuries, the entire tibial tuberosity and anterior proximal physis are elevated and hinged posteriorly. The surgeon must gently dissect medially and laterally into the joint capsule until the intra-articular physeal fracture line is directly visualized. Copious irrigation is employed to remove osteochondral debris. The surgeon will frequently encounter the torn periosteal sleeve folded deep into the physeal gap. This periosteum must be carefully extracted using a Freer elevator or small right-angle forceps. If the anterior horn of the meniscus is entrapped, it must be anatomically reduced; meniscectomy is strictly contraindicated in the pediatric population due to the catastrophic long-term biomechanical consequences.
Reduction of the fracture must be anatomic and should be achieved with minimal force. The reduction maneuver typically mimics closing a book or a hinge, bringing the anterior tuberosity fragment down to its anatomical bed. The knee is then extended; if the reduction springs open or feels "elastic," soft tissue entrapment is still present and must be re-addressed. Direct visual confirmation of joint congruity is combined with multi-planar fluoroscopy. A pointed reduction forceps (Weber clamp) can be applied to hold the reduction provisionally, taking care not to crush the fragile metaphyseal bone or the articular cartilage. The tines of the clamp should be placed precisely to provide compression perpendicular to the primary fracture plane.
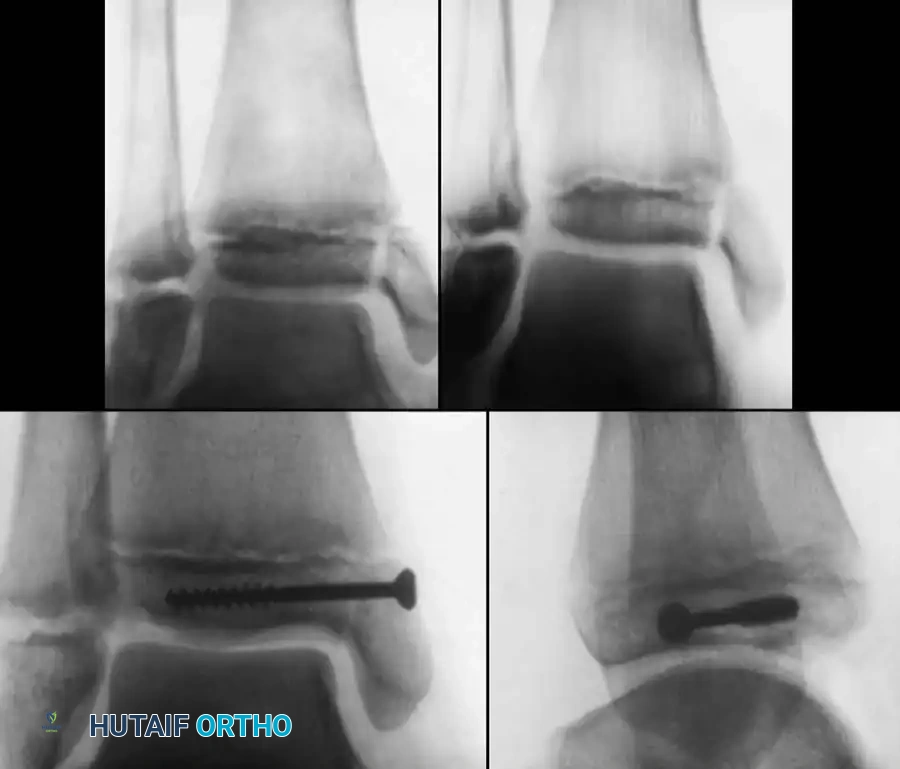
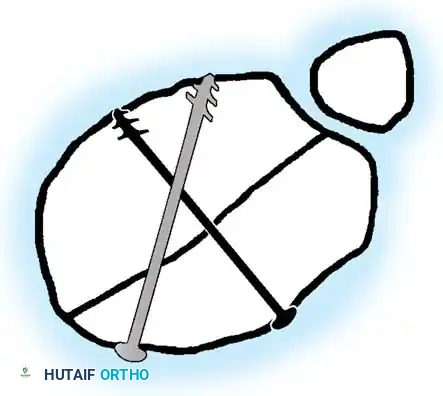
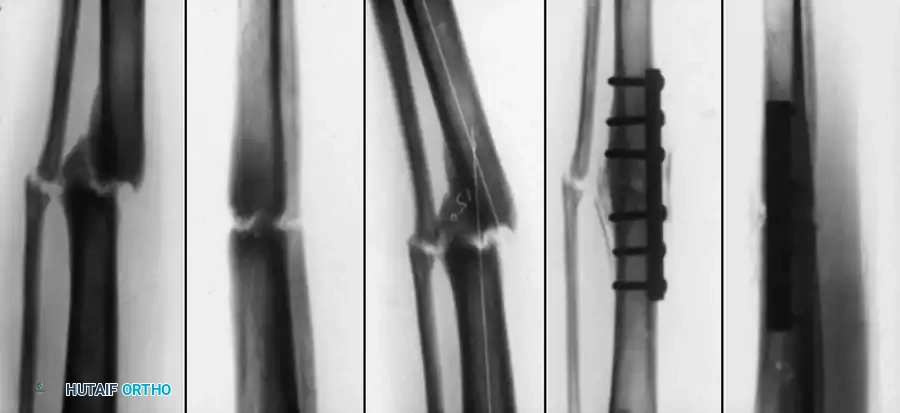
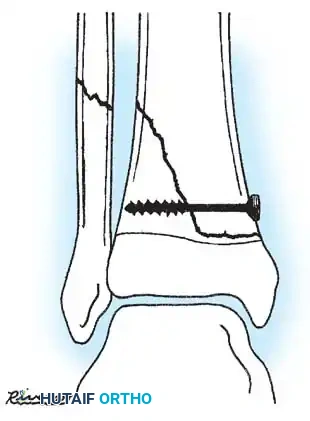
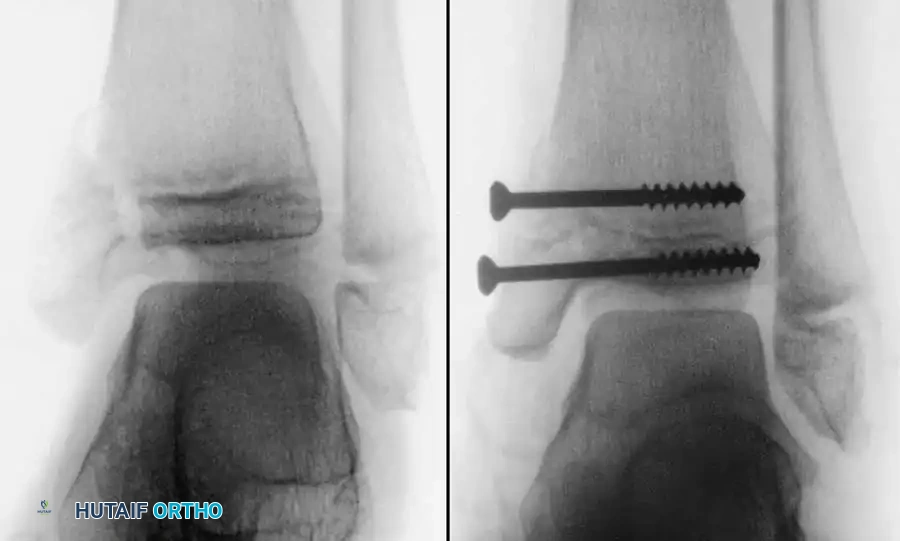
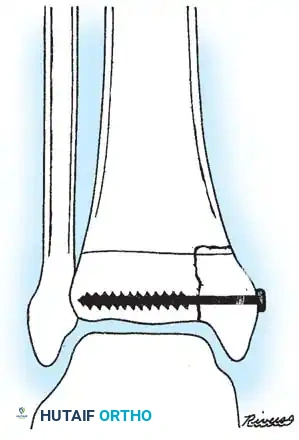
Definitive fixation is tailored to the patient's skeletal maturity. In younger children with significant remaining growth potential, the fracture is stabilized utilizing smooth K-wires placed transversely through the epiphysis, avoiding the physis entirely if possible. If transphyseal fixation is required for the metaphyseal component, the wires are placed centrally and removed at 3 to 4 weeks post-operatively. In adolescents nearing skeletal maturity, rigid internal fixation is achieved using 4.0mm or 4.5mm partially threaded cannulated cancellous screws. Guide pins are placed parallel to the articular surface, and their position is confirmed fluoroscopically. The lateral cortex is overdrilled to achieve a lag effect, and the screws are advanced carefully. Washers may be utilized if the metaphyseal bone is osteopenic, though they can cause hardware prominence beneath the thin anterior skin. Following final fixation, the tourniquet is deflated, meticulous hemostasis is achieved, and the retinaculum and surgical wounds are closed in layers over a closed suction drain if necessary.

Complications, Incidence Rates, and Salvage Management
The management of pediatric knee dislocations and proximal tibial fractures is fraught with potential complications, ranging from immediate limb-threatening vascular injuries to insidious, long-term angular deformities. The incidence of these complications is directly correlated with the energy of the initial trauma and the precision of the surgical intervention.
| Complication | Estimated Incidence | Pathophysiology / Risk Factors | Salvage Management / Intervention |
|---|---|---|---|
| Popliteal Artery Injury | 5 - 13% | Posterior displacement of metaphysis tethering artery at soleal arch. | Emergent vascular repair/bypass, spanning external fixation, fasciotomies. |
| Compartment Syndrome | 10 - 20% | High-energy crush, reperfusion injury post-vascular repair. | Emergent 4-compartment fasciotomy, delayed primary closure/skin grafting. |
| Premature Physeal Closure | 15 - 25% | Crush injury to resting zone (SH V), transphyseal threaded hardware. | Physeal bar resection (Langenskiöld), fat interposition, guided growth (8-plates). |
| Cozen's Phenomenon | 30 - 50% (Metaph.) | Asymmetric hyperemic overgrowth of medial proximal tibia post-fracture. | Observation (typically remodels in 12-24 mos), corrective osteotomy if persistent >2 yrs. |
| Genu Recurvatum | 5 - 10% | Anterior physeal arrest (tuberosity) with continued posterior growth. | Proximal tibial opening wedge osteotomy, distraction osteogenesis. |
Vascular injury and compartment syndrome represent the most acute and devastating complications. Failure to diagnose a popliteal artery intimal tear can lead to delayed thrombosis, profound ischemia, and eventual amputation. Even when vascular continuity is restored, the subsequent reperfusion injury significantly elevates intra-compartmental pressures. The rigid fascial boundaries of the lower leg cannot accommodate the massive third-spacing of fluids, leading to microvascular collapse and muscle necrosis. The orthopedic surgeon must maintain a high index of suspicion; if intra-compartmental pressures exceed 30 mmHg or are within 30 mmHg of the diastolic blood pressure (Delta P < 30), emergent four-compartment fasciotomies via dual medial and lateral incisions are absolutely mandated. Delaying fasciotomy beyond 6 hours of ischemia results in irreversible neuromuscular damage.

Growth arrest is the most common long-term complication following proximal tibial physeal fractures. The
Clinical & Radiographic Imaging Archive