Pediatric Hip Fractures: What Every Clinician Must Know

Key Takeaway
Discover the latest medical recommendations for Pediatric Hip Fractures: What Every Clinician Must Know. Pediatric hip fractures are rare injuries in children, occurring less than 1% as often as in adults. They typically result from severe direct trauma, such as motor vehicle accidents, accounting for 75-80% of cases. Mechanisms include axial loading, torsion, hyperabduction, or a direct blow, potentially impacting the developing proximal femur and its critical blood supply.
Introduction and Epidemiology
Pediatric hip fractures represent a rare yet critically significant injury in musculoskeletal trauma, demanding a nuanced understanding distinct from their adult counterparts. While hip fractures are exceptionally rare in children, occurring less than 1% as often as in adults, their potential for devastating long-term complications, particularly avascular necrosis (AVN) of the femoral head, necessitates prompt diagnosis and meticulous management. These injuries often present unique challenges due to the presence of open physes, high remodeling potential, and a delicate vascular supply to the femoral head.
The epidemiology of pediatric hip fractures exhibits a bimodal distribution. In very young children (toddlers and preschoolers), these fractures are uncommon and often associated with high-energy trauma, though a significant percentage warrant investigation for non-accidental trauma, especially if the injury mechanism is inconsistent with the child's developmental stage. In older children and adolescents, the etiology shifts predominantly towards high-energy mechanisms such as motor vehicle collisions, falls from significant heights, or sports-related trauma. Pathologic fractures, secondary to underlying bone pathology such as cysts, tumors, or metabolic bone diseases, also constitute a smaller but important subgroup across all age ranges. The incidence is reported to be between 0.3 and 1.5 per 100,000 children per year, underscoring their infrequency but highlighting the need for specialized expertise when encountered.
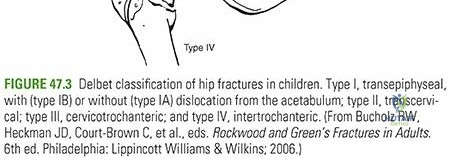
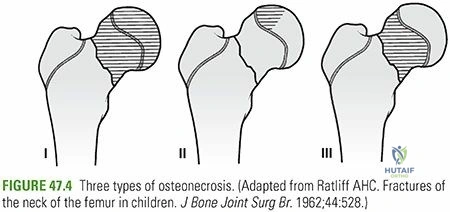
The classification system most widely used for pediatric hip fractures is the Delbet classification, which categorizes fractures based on their anatomical location relative to the proximal femoral physis:
* Type I: Transphyseal fractures (with or without epiphyseal dislocation). These are often Salter-Harris type I or II injuries through the physis, frequently associated with high-energy trauma or occurring in conditions like slipped capital femoral epiphysis (SCFE).
* Type II: Transcervical fractures. These involve the femoral neck and are highly prone to vascular disruption.
* Type III: Basicervical fractures. These occur at the junction of the femoral neck and intertrochanteric region.
* Type IV: Intertrochanteric fractures. These are extracapsular fractures involving the greater and lesser trochanters.
Each Delbet type carries a distinct prognosis and management strategy, primarily driven by the risk of AVN. Understanding the specific epidemiological patterns and classification is foundational for effective clinical assessment and treatment planning.
Surgical Anatomy and Biomechanics
A profound understanding of the developing proximal femoral anatomy, its ossification patterns, and delicate vascularity is paramount for any clinician managing pediatric hip fractures. The unique structural and biological characteristics of the pediatric hip dictate fracture patterns, influence treatment decisions, and largely determine the potential for devastating complications.
Proximal Femoral Ossification and Physis
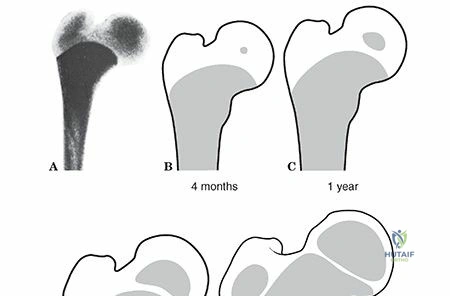
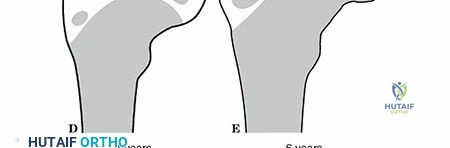
The development of the proximal femur is characterized by a series of distinct ossification centers.
* The proximal femur itself begins ossifying at approximately week 7 in utero.
* The proximal femoral epiphysis, which forms the femoral head, typically appears between ages 4 to 8 months. This cartilaginous anlage is critical for spherical development of the femoral head.
* The trochanteric apophysis, forming the greater trochanter, usually appears around 4 years of age.
* The lesser trochanteric apophysis appears later, typically between 9 and 12 years.
These growth centers remain open and active throughout childhood and adolescence. The proximal femoral epiphysis fuses with the femoral neck by approximately age 18 years, marking skeletal maturity. The trochanteric apophysis fuses later, typically between ages 16 to 18 years. The presence of these physes significantly alters the biomechanical response to trauma and poses challenges for internal fixation, as hardware crossing these physes can lead to growth arrest or deformity.
Physeal Contribution to Growth
The proximal femoral physis contributes significantly to the metaphyseal growth of the femoral neck and, to a lesser extent, to the primary appositional growth of the femoral head. Disruptions in this region, particularly Type I (transphyseal) and Type II (transcervical) fractures, can lead to severe architectural changes that may affect the overall anatomic development of the proximal femur. These include coxa vara or valga, leg length discrepancy, and even femoral head deformity secondary to physeal bar formation or growth arrest.
The trochanteric apophysis primarily contributes to the appositional growth of the greater trochanter and less to the metaphyseal growth of the femoral shaft. Injuries to this apophysis are less commonly associated with significant limb length discrepancy but can affect hip abductor function due to altered lever arm mechanics.
Vascular Anatomy and Avascular Necrosis Risk
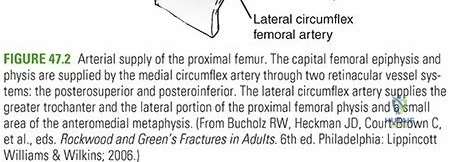
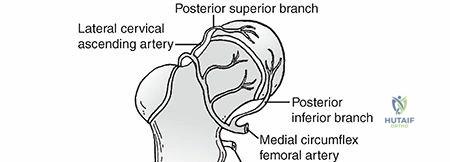
The blood supply to the pediatric femoral head is notoriously tenuous and is the primary determinant of the high AVN rate following hip fractures. This supply is predominantly derived from the medial femoral circumflex artery (MFCA) and, to a lesser extent, the lateral femoral circumflex artery (LFCA).
- The MFCA is the dominant vessel. It typically courses posteriorly and superiorly to the femoral neck, giving rise to several retinacular branches. These branches form an extracapsular ring, often referred to as the circulus arteriosus cervicalis, at the anterosuperior portion of the intertrochanteric groove.
- From this extracapsular ring, ascending retinacular vessels penetrate the joint capsule and ascend along the femoral neck to supply the epiphysis. The superior retinacular vessels, derived primarily from the MFCA, are particularly vulnerable to injury in displaced femoral neck fractures.
- The LFCA provides additional supply, particularly anteriorly and inferiorly, but its contribution to the epiphyseal head is less significant than the MFCA.
- The artery of the ligamentum teres (foveal artery), a branch of the obturator artery, also supplies the femoral head. Its contribution is generally more substantial in younger children, becoming less significant with age as the retinacular vessels mature. In cases of retinacular vessel injury, a patent foveal artery can partially mitigate AVN risk, especially in children under 4-5 years of age.
Any fracture that disrupts the integrity of the retinacular vessels, particularly displaced transcervical fractures (Delbet Type II) and transphyseal fractures (Delbet Type I), carries a high risk of AVN. The intracapsular hematoma associated with displaced fractures can also increase intra-articular pressure, further compromising blood flow to the femoral head. The integrity of these vessels is paramount, making urgent, gentle reduction and stable fixation critical for preserving vascularity.

Biomechanics
The pediatric proximal femur, particularly the femoral neck, is more elastic and less brittle than in adults. This elasticity can contribute to specific fracture patterns, such as greenstick or torus fractures, although high-energy forces are typically required to cause complete displacement. The developing bone also has a robust periosteal sleeve, which can provide some inherent stability and contribute to remodeling capacity, especially in non-displaced or minimally displaced fractures. However, this remodeling potential is limited in the highly constrained environment of the hip joint and for severely displaced fractures. The angle of inclination and anteversion of the femoral neck change significantly with growth, affecting the biomechanical forces across the hip and influencing fracture patterns and fixation strategies. Understanding these biomechanical principles is essential for achieving stable reduction and optimizing hardware placement to allow for continued growth and remodeling.

Indications and Contraindications
The management of pediatric hip fractures requires careful consideration of fracture stability, displacement, associated injuries, and the child's age and overall health. The primary goals are to achieve an anatomical or near-anatomical reduction, provide stable fixation, preserve the delicate vascular supply to the femoral head, and minimize complications such as AVN, growth arrest, and malunion.
Operative Indications
The vast majority of pediatric hip fractures, particularly those involving the femoral neck, require surgical intervention.
* Displaced fractures: Any significant displacement in Delbet Types I, II, and III fractures demands surgical reduction and fixation. Displacement greater than 2 mm is generally considered an indication for operative intervention due to the high risk of AVN and malunion.
* Unstable fractures: Fractures that cannot be maintained in an acceptable reduction with conservative measures.
* Delbet Type I (Transphyseal) fractures: These are Salter-Harris type I or II injuries through the capital femoral physis. Due to the high risk of AVN (up to 90% if completely displaced) and growth arrest, urgent reduction and stable fixation, often with smooth pins or cannulated screws carefully placed to avoid physeal damage, are critical.
* Delbet Type II (Transcervical) fractures: These are the most common type of pediatric hip fracture and carry the highest risk of AVN (30-70%). Nearly all displaced transcervical fractures require urgent open or closed reduction and stable internal fixation to restore anatomy and preserve vascularity.
* Delbet Type III (Basicervical) fractures: While having a slightly lower AVN rate than Type II, these are still intracapsular and displaced fractures require operative management.
* Delbet Type IV (Intertrochanteric) fractures: These are extracapsular and generally have a lower risk of AVN. However, displaced or unstable intertrochanteric fractures, particularly in older children, benefit from operative fixation to allow for early mobilization and prevent malunion. In younger children, closed reduction and spica cast immobilization may be considered for stable, minimally displaced fractures, but unstable patterns often require fixation.
* Fractures with associated injuries: Such as hip dislocations (fracture-dislocations), warrant prompt surgical intervention to address both components.
* Pathologic fractures: While the underlying pathology needs to be addressed, the fracture itself often requires stabilization, which may involve internal fixation, often augmented with bone grafting.
Non-Operative Indications
Non-operative management is reserved for a very select group of pediatric hip fractures and is typically only considered under specific circumstances.
* Minimally displaced or undisplaced Delbet Type IV (Intertrochanteric) fractures: In younger children with excellent remodeling potential, a stable, non-displaced intertrochanteric fracture may be managed with spica cast immobilization. Close radiographic follow-up is essential to monitor for displacement.
* Stable, minimally displaced impacted fractures: Extremely rare for femoral neck fractures, but if encountered and demonstrably stable, may be considered for cast immobilization, particularly in very young children where surgical risks are higher. This decision is made with extreme caution due to the high inherent risk of displacement and AVN.
* Children with severe comorbidities: In rare instances, if a child's overall medical status precludes general anesthesia or surgical intervention, non-operative management might be considered as a last resort, even for displaced fractures, accepting the high risk of complications.
Contraindications
Absolute contraindications to operative intervention for pediatric hip fractures are rare, especially given the significant morbidity associated with non-operative management of displaced fractures.
* Unstable medical condition: A child who is medically unstable and cannot tolerate anesthesia or surgery (e.g., severe head injury, hemodynamic instability) should be stabilized before orthopedic intervention, though prompt, often life-saving, fracture stabilization may be part of initial resuscitation in polytrauma.
* Non-displaced, stable fractures amenable to conservative treatment: As noted above, these are a very small subset, primarily certain intertrochanteric fractures.
* Severe local infection: Active infection in the surgical field would contraindicate immediate internal fixation, requiring initial infection control.
The decision to operate is almost always made in favor of stabilization to mitigate the severe long-term sequelae inherent to these injuries.
Operative vs Non-Operative Indications Table
| Indication Type | Specific Condition | Operative Approach | Non-Operative Approach |
|---|---|---|---|
| Delbet Type I | Transphyseal (Salter-Harris I or II), with or without epiphyseal displacement | Required: Urgent closed or open reduction and internal fixation (CRIF/ORIF) with smooth K-wires or cannulated screws (1-2) strategically placed to avoid violating physis. Goal is anatomic reduction within 6 hours to minimize AVN risk. | Rare/Contraindicated: Only for truly undisplaced, stable injuries (extremely rare, often diagnosed retrospectively). High risk of AVN, growth arrest, and chondrolysis makes conservative management exceptionally risky. If medically unstable and surgery is not possible, hip spica cast may be applied with high risk awareness. |
| Delbet Type II | Transcervical (most common) | Required: Urgent CRIF/ORIF with multiple cannulated screws (2-3) or an adolescent hip screw. Anatomic reduction is crucial. Open reduction is common due to high displacement and capsular interposition. Immediate stabilization to prevent AVN. | Contraindicated: High risk (30-70%) of AVN, nonunion, and malunion due to disruption of retinacular blood supply. Undisplaced fractures are exceedingly rare and prone to secondary displacement. |
| Delbet Type III | Basicervical | Required: CRIF/ORIF with multiple cannulated screws (2-3) or adolescent hip screw. Slightly lower AVN risk than Type II, but still significant. Open reduction may be necessary for irreducible fragments. | Contraindicated: Despite lower AVN risk, displaced basicervical fractures are intracapsular and subject to similar risks of nonunion and AVN if not anatomically reduced and stably fixed. |
| Delbet Type IV | Intertrochanteric (extracapsular) | Usually Required (for displaced/unstable): CRIF/ORIF with cannulated screws, tension band wiring, pediatric locking plate, or flexible intramedullary nail (depending on age, size, and fracture pattern). Offers stable fixation, early mobilization. | Potentially indicated (for non-displaced/stable in young children): Closed reduction and hip spica cast immobilization (for 6-10 weeks) may be considered for truly non-displaced or minimally displaced, stable intertrochanteric fractures in very young children (typically <6-8 years) with excellent remodeling potential. Requires rigorous radiographic follow-up for stability. Any significant displacement or instability necessitates surgical management. |
| Associated Injuries | Fracture-dislocation, polytrauma | Required: Urgent surgical stabilization of hip fracture, often as part of broader trauma management. | Contraindicated: Hip instability or significant associated injuries necessitate surgical correction to prevent further damage and optimize overall patient outcome. |
| Pathologic Fractures | Due to underlying bone lesions | Required: Internal fixation to stabilize the fracture, often combined with biopsy, curettage, and bone grafting depending on the underlying pathology. | Contraindicated for displaced: Non-operative management is typically reserved for non-displaced pathological fractures where the underlying condition does not require surgical intervention and the fracture is stable. High risk of further displacement due to bone fragility. |
| Medically Unstable Child | Severe comorbidities precluding surgery (rare) | Delayed or Staged: Priority is medical stabilization. If hip fracture stabilization is deemed life-saving or critical to overall trauma management, immediate surgery may proceed after resuscitation. | Considered as last resort: If general anesthesia and surgery are absolutely contraindicated due to life-threatening comorbidities, non-operative management (e.g., traction followed by spica cast) may be pursued, acknowledging the high risk of suboptimal outcome and complications. This is a rare, complex decision made by a multidisciplinary team. |
Pre Operative Planning and Patient Positioning
Thorough pre-operative planning is critical for optimizing outcomes in pediatric hip fractures, given their complexity and the high risk of complications.
Diagnostic Imaging and Assessment
- Standard Radiographs: Anteroposterior (AP) and frog-leg lateral views of the pelvis and injured hip are the initial imaging modalities. These provide basic information on fracture pattern, displacement, and epiphyseal integrity. Careful assessment of the physis and the capital femoral epiphysis is essential.
- Computed Tomography (CT) Scan: A CT scan with 3D reconstructions is highly recommended for displaced fractures, especially transcervical and basicervical types. It provides invaluable information regarding fracture morphology, displacement, comminution, and potential physeal involvement. This aids in surgical approach planning, reduction maneuver prediction, and hardware selection. CT angiography can occasionally be utilized if vascular compromise is suspected, though this is rare.
- Magnetic Resonance Imaging (MRI): MRI is not typically used for acute fracture diagnosis but is invaluable for assessing vascular integrity (early signs of AVN), physeal injury (e.g., physeal bar formation), and occult fractures or underlying pathology. It may be considered pre-operatively if there is a strong suspicion of pre-existing pathology or if delayed presentation raises concerns for early AVN.
- Skeletal Survey: In children under 2 years of age, or if the mechanism of injury is inconsistent with the fracture pattern, a skeletal survey to rule out non-accidental trauma is imperative.
Pre-operative Considerations
- Timing of Surgery: For displaced intracapsular hip fractures (Delbet Types I, II, III), urgent reduction and fixation within 6-12 hours of injury is widely advocated to minimize the risk of AVN. This is a surgical emergency.
- Associated Injuries: A comprehensive evaluation for associated injuries (e.g., head trauma, abdominal injury, other skeletal fractures) is crucial, especially in high-energy trauma. Multidisciplinary consultation with trauma surgeons, neurosurgeons, and intensivists may be necessary.
- Medical Optimization: The child's overall medical status must be optimized before surgery. This includes fluid resuscitation, pain control, and addressing any coagulopathies.
- Antibiotic Prophylaxis: Standard pre-operative intravenous antibiotics (e.g., cefazolin) should be administered according to institutional protocols.
- Blood Products: Type and cross-match blood should be readily available, especially for open reductions or complex cases.
Patient Positioning
- Supine on a Radiotranslucent Table: The patient is positioned supine on a radiolucent operating table, allowing unrestricted fluoroscopic access in AP, lateral, and oblique planes.
- Traction Capability: The table should ideally have traction capabilities, such as a fracture table, to facilitate reduction maneuvers, especially for closed reduction. Alternatively, manual traction can be applied.
- Leg Draping: The entire affected lower extremity, from the iliac crest to the foot, should be meticulously prepped and draped to allow for full range of motion of the hip and knee during reduction and fixation. This often involves a sterile stockinette and impervious draping, isolating the foot to allow for manipulation.
- C-arm Placement: The C-arm must be positioned to allow unobstructed views of the proximal femur, acetabulum, and the proposed entry points for hardware. The contralateral limb should be placed in an abducted, flexed position to facilitate true lateral views of the femoral neck.
- Surgeon and Assistant Positioning: The primary surgeon typically stands on the ipsilateral side of the fracture, with assistants positioned appropriately for exposure and instrument handling.

Detailed Surgical Approach and Technique
The specific surgical approach and fixation technique are highly dependent on the Delbet fracture type, the degree of displacement, the child's age, and the surgeon's preference. The overarching principles include anatomical reduction, stable fixation, protection of the femoral head vascularity, and preservation of the physes.
General Principles
- Urgency: Displaced intracapsular fractures require urgent reduction (ideally within 6 hours) to minimize AVN risk.
- Gentle Tissue Handling: Minimize soft tissue stripping, particularly around the femoral neck and capsule, to preserve remaining vascular supply.
- Anatomic Reduction: Achieve as anatomical a reduction as possible. Malreduction significantly increases the risk of AVN, nonunion, and malunion.
- Physeal Protection: Hardware should ideally avoid crossing open physes, especially the capital femoral physis. If unavoidable (e.g., in Type I fractures), smooth, small-diameter Kirschner wires are preferred over threaded screws. For transcervical fractures in older children nearing skeletal maturity, threaded cannulated screws may be used, carefully directed.
- Stable Fixation: The construct must be stable enough to withstand early rehabilitation and prevent loss of reduction.
Reduction Techniques
Closed Reduction
- Indication: Primarily for Delbet Type I, II, or III fractures that are amenable to reduction with traction and manipulation, and Type IV fractures.
- Technique: Performed under fluoroscopic guidance with the patient on a fracture table or with manual traction.
- Traction: Initial longitudinal traction is applied to disimpact the fracture and restore length.
- Manipulation: Specific maneuvers are employed based on fracture displacement. For anterior displacement, hip flexion and internal rotation are often used. For posterior displacement, gentle extension and external rotation.
- Confirmation: Reduction is confirmed with AP and true lateral fluoroscopic views. Adequacy of reduction is assessed (e.g., Shenton's line, cortical alignment).
Open Reduction
- Indication: When closed reduction fails, especially due to capsular interposition, severe comminution, or irreducible fragments. More common in Delbet Type II and III fractures.
- Approaches:
- Anterolateral Approach (Watson-Jones): This approach utilizes the interval between the tensor fascia lata and gluteus medius/minimus. It provides excellent visualization of the anterior and superior aspects of the femoral head and neck.
- Incision: Longitudinal incision centered over the greater trochanter, extending proximally towards the ASIS and distally along the femur.
- Dissection: Incise fascia lata, then identify and separate the tensor fascia lata (innervated by superior gluteal nerve) anteriorly from the gluteus medius/minimus (also superior gluteal nerve) posteriorly. The internervous plane is crucial.
- Capsulotomy: Perform a careful anterior or anterosuperior capsulotomy. The hip capsule is often distended with hematoma; evacuation of this can decompress the joint and improve blood flow.
- Reduction: Direct visualization allows for precise reduction of fracture fragments using ball-spikes, periosteal elevators, or dental picks. Traction and manipulation are still used.
- Anterior Approach (Smith-Petersen): Provides direct access to the anterior hip joint.
- Incision: Longitudinal incision from the ASIS directed towards the greater trochanter.
- Dissection: Identify the interval between the sartorius (femoral nerve) and the tensor fascia lata (superior gluteal nerve). Retract the sartorius and rectus femoris medially, and the TFL laterally. Ligate ascending branches of the LFCA if necessary, though efforts should be made to preserve them.
- Capsulotomy: Anterior capsulotomy.
- Reduction: Direct visualization and manipulation.
- Anterolateral Approach (Watson-Jones): This approach utilizes the interval between the tensor fascia lata and gluteus medius/minimus. It provides excellent visualization of the anterior and superior aspects of the femoral head and neck.
Fixation Techniques
Percutaneous Pinning (Cannulated Screws/K-wires)
- Indication: Most common technique for Delbet Types I, II, and III fractures after successful closed or open reduction.
- Technique:
- Guide Wire Insertion: Once reduction is achieved and confirmed fluoroscopically, 2-3 cannulated guide wires (typically 1.6-2.0 mm K-wires) are inserted.
- For Delbet Types II and III (transcervical and basicervical), wires are typically started laterally on the femoral shaft, aiming for the femoral head. A "triangle of stability" configuration is often used, with screws in the superior, inferior, and posterior aspects of the femoral neck. Crucially, the wires should be placed to avoid the capital femoral physis, especially in younger children. This often means placing them parallel to the physis or distally to it.
- For Delbet Type I (transphyseal), small-diameter smooth K-wires (often 2) are inserted across the physis into the epiphysis to provide stable fixation without compressing the growth plate, minimizing physeal arrest. These are generally placed parallel.
- Screw Selection: Depending on age and bone quality, fully threaded cannulated screws (typically 4.0 mm or 4.5 mm) are usually preferred over partially threaded screws for better purchase in osteopenic pediatric bone. Screw length is crucial – ensure adequate purchase in the femoral head without breaching the articular cartilage.
- Screw Insertion: After measuring, drilling (if necessary), screws are inserted over the guide wires.
- Confirmation: Final AP and lateral fluoroscopic images confirm reduction, hardware position, and screw length. Avoid hardware protrusion into the joint.
- Guide Wire Insertion: Once reduction is achieved and confirmed fluoroscopically, 2-3 cannulated guide wires (typically 1.6-2.0 mm K-wires) are inserted.


Plates and Screws (Pediatric Hip Screw or Locking Plates)
- Indication: Primarily for Delbet Type IV (intertrochanteric) fractures, unstable Delbet Type III fractures in larger adolescents, or severely comminuted fractures.
- Technique:
- Approach: Typically a lateral approach is used.
- Reduction: Reduce the fracture fragments.
- Plate Application: A pediatric dynamic hip screw (DHS) system, a locking pediatric proximal femur plate, or a reconstruction plate may be used. The lag screw or blade of a DHS is inserted into the femoral head, and the plate is secured to the femoral shaft with screws. For locking plates, locking screws provide angular stability.
- Considerations: Ensure the plate and screw construct provide sufficient stability without compromising the femoral blood supply or future growth. For younger children, care must be taken to choose implants that allow for remodeling and avoid creating stress risers.
Intramedullary Nailing
- Indication: Less common for proximal femoral fractures, but flexible intramedullary nails or a short cephalomedullary nail may be considered for stable Delbet Type IV (intertrochanteric) fractures in older children or adolescents.
- Technique: Entry point typically at the greater trochanter or piriformis fossa (carefully avoiding vascular damage). Nails are advanced across the fracture site and into the femoral head.
Post-Fixation Evaluation
- Fluoroscopy: Multiple views to confirm reduction and hardware placement.
- Wound Closure: Standard layered closure. A drain may be considered for large hematomas or open reduction.
Complications and Management
Pediatric hip fractures, despite optimal management, are associated with a high rate of severe complications, primarily due to the vulnerability of the femoral head's blood supply and the presence of open growth plates. Long-term follow-up is essential to detect and manage these sequelae.
Common Complications and Management Table
| Complication | Incidence | Etiology/Risk Factors | Management / Salvage Strategy |
| Delbet Type I | 2-5% of all pediatric hip fractures. 90% AVN if displaced. | High-energy trauma, SCFE. Complete disruption of epiphyseal blood supply. | Salvage: For AVN, non-weight bearing, observation initially. For severe deformity or collapse, reconstructive osteotomies (e.g., valgus osteotomy), vascularized fibular graft, or hip arthrodesis in severe cases. Total hip arthroplasty (THA) is typically deferred until skeletal maturity. | Delbet Type II (transcervical) | 30-70% AVN, 10-30% nonunion. Highest risk. Factors: delay to reduction, poor reduction, increased number of fixation attempts, severe displacement. | AVN Salvage: Non-weight bearing, protected activity. For head collapse/deformity: valgus osteotomy (to improve coverage and correct coxa vara), femoral head resurfacing, vascularized fibular graft (controversial in children). Ultimately, total hip arthroplasty (THA) or hip arthrodesis for painful, end-stage AVN, usually deferred until skeletal maturity.
Nonunion Salvage: Revision internal fixation with bone grafting (autograft or allograft), potentially with added stability (e.g., plate and screw construct). Corrective osteotomy to optimize biomechanics.
Malunion Salvage: Corrective osteotomy (e.g., varus derotation osteotomy for valgus malunion, valgus osteotomy for coxa vara) to restore femoral neck-shaft angle and improve joint mechanics. |
| Primary Complication: | | | |
| |
| |
| |
| |
| |
| |
| ** |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
| |
|
Clinical & Radiographic Imaging