Pediatric Tibia and Fibula Fractures: Essential Clinical Insights
Key Takeaway
We review everything you need to understand about Pediatric Tibia and Fibula Fractures: Essential Clinical Insights. Pediatric tibia and fibula fractures are common, representing 15% of all pediatric fractures, typically occurring around age 8. These lower leg bone breaks often result from motor vehicle trauma (50% for ipsilateral fractures) or indirect rotational forces. The tibia is also the second most fractured bone in abused children, making comprehensive evaluation crucial.
Introduction and Epidemiology
Pediatric tibia and fibula fractures represent a significant portion of orthopedic trauma, requiring a nuanced understanding of skeletal immaturity, growth potential, and injury mechanisms. The tibia is the third most common pediatric long bone fracture, following femur and forearm fractures, and accounts for approximately 15% of all pediatric fractures. The average age of occurrence is 8 years, though the distribution is bimodal, peaking in early childhood (toddler years) and again during early adolescence due to increased participation in high-impact sports and motor vehicle exposure.
The ratio of incidence in boys compared to girls is 2:1. Of all pediatric tibial fractures, approximately 30% are associated with ipsilateral fibular fractures. The presence or absence of an intact fibula significantly alters the biomechanics of the injury, the fracture pattern, and the propensity for specific angular deformities during healing.
Crucially, the tibia is the second most commonly fractured bone in abused children. Non-accidental trauma must remain a high index of suspicion in non-ambulatory infants or children presenting with inconsistent histories. Statistics indicate that 26% of abused children presenting with fractures have a tibia fracture. Thorough evaluation, including a complete skeletal survey in children under two years of age and consultation with child protection teams, is mandatory when non-accidental trauma is suspected.
Proximal tibial metaphyseal fractures warrant specific epidemiological consideration. These are relatively uncommon, representing less than 5% of all pediatric fractures and approximately 11% of pediatric tibia fractures. They exhibit a peak incidence between the ages of 3 and 6 years and are notorious for a specific post-traumatic complication known as Cozen’s phenomenon, which involves progressive valgus overgrowth.
Surgical Anatomy and Biomechanics
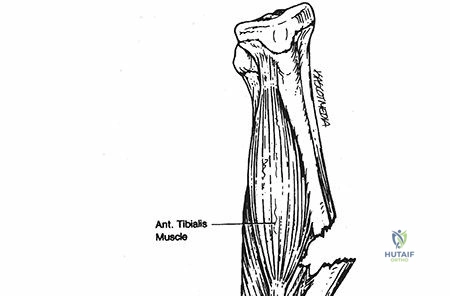
A profound understanding of the osseous and soft tissue anatomy of the pediatric lower leg is essential for accurate diagnosis and surgical planning. The anteromedial aspect of the tibia is entirely subcutaneous, possessing no overlying musculature for protection. This anatomical reality makes the tibia highly susceptible to open fractures and severe soft tissue compromise following high-energy trauma.
The tibia develops from three consistent primary and secondary ossification centers:
* Diaphyseal Center: Primary ossification occurs at 7 weeks of gestation.
* Proximal Epiphysis: This secondary ossification center appears just after birth and typically closes at 16 years of age.
* Distal Epiphysis: This secondary ossification center appears in the second year of life, with closure occurring around age 15.
Surgeons must be acutely aware that the medial malleolus and tibial tubercle may present as separate, accessory ossification centers. These normal developmental variants must not be confused with avulsion fractures or intra-articular pathology.
Fibular development mimics the tibia with three primary ossification centers:
* Diaphyseal Center: Ossification occurs at 8 weeks of gestation.
* Distal Epiphysis: Appears at age 2 years, with closure at age 16 years.
* Proximal Epiphysis: Appears at age 4 years, with closure delayed until age 16 to 18 years.
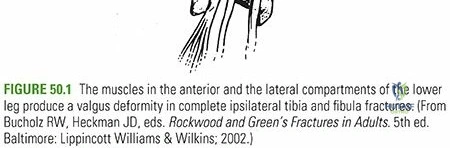
Biomechanically, the proximal tibial physis is generally structurally weaker than the adjacent metaphyseal region. However, due to the robust nature of the proximal periosteal sleeve and the specific mechanisms of injury, fractures in the tibial metaphysis still occur and present unique challenges. The presence of an intact fibula acts as a biological strut. While an intact fibula prevents significant fracture shortening, it acts as a tether that can drive the tibia into a varus deformity during the consolidation phase. Conversely, in proximal metaphyseal fractures, the mechanism often involves a valgus force applied to the extended knee, causing the medial cortex of the metaphysis to fail in tension, frequently resulting in a nondisplaced or greenstick fracture of the medial cortex while the lateral cortex undergoes plastic deformation.
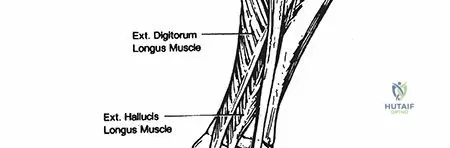
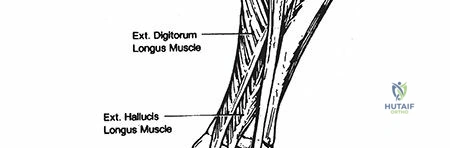
The lower leg is divided into four rigid fascial compartments: anterior, lateral, superficial posterior, and deep posterior. The anterior tibial artery passes from the posterior compartment to the anterior compartment through a proximal defect in the interosseous membrane, making it highly vulnerable to tethering and injury in proximal third tibial fractures.
Indications and Contraindications
The decision-making process for managing pediatric tibia and fibula fractures hinges on patient age, fracture pattern, soft tissue envelope integrity, and the degree of displacement. Because children possess immense remodeling potential—particularly in the plane of joint motion (sagittal plane)—non-operative management is the mainstay for the vast majority of these injuries. However, strict radiographic parameters must be respected to prevent long-term functional deficits.
Acceptable alignment parameters vary by age. For children under 8 years of age, up to 10 degrees of varus or valgus, 10 degrees of pro- or recurvatum, and 10 millimeters of shortening are generally acceptable. For children over 8 years, the remodeling potential decreases, and acceptable parameters tighten to less than 5 degrees of coronal or sagittal angulation and less than 5 millimeters of shortening.
| Clinical Scenario | Operative Management | Non Operative Management |
|---|---|---|
| Open Fractures | Absolute Indication (I&D, stabilization) | Contraindicated |
| Compartment Syndrome | Absolute Indication (Fasciotomy) | Contraindicated |
| Floating Knee | Relative Indication (Facilitates mobilization) | Rarely indicated |
| Polytrauma | Relative Indication (Damage control) | Dependent on overall stability |
| Unacceptable Alignment | Indicated if closed reduction fails | Indicated if reduction is stable |
| Toddlers Fracture | Contraindicated | Absolute Indication (Immobilization) |
| Proximal Metaphyseal | Rarely indicated (High risk of Cozen's) | Primary Indication (Cast in varus) |
| Intact Fibula with Varus | Indicated if varus is progressive | Indicated with close radiographic follow-up |
Contraindications to surgical intervention include undisplaced or minimally displaced fractures that fall well within acceptable alignment parameters, isolated fibula fractures with an intact tibia, and classic toddler's fractures. Active infection at the planned surgical site represents a strict contraindication to internal fixation.
Pre Operative Planning and Patient Positioning
Thorough clinical and radiographic evaluation must precede any surgical intervention. Because more than 60% of pediatric tibial fractures are associated with motor vehicle or pedestrian-motor vehicle trauma, a full pediatric Advanced Trauma Life Support (ATLS) protocol must be strictly observed. Life-threatening injuries must be addressed prior to orthopedic management.
Patients typically present with an inability to bear weight, gross deformity, and painful range of motion of the adjacent knee or ankle. A meticulous neurovascular evaluation is essential, requiring documented assessment of both the dorsalis pedis and posterior tibial artery pulses, as well as the sensory and motor function of the peroneal and tibial nerves. Palpation of the anterior, lateral, superficial posterior, and deep posterior muscle compartments is critical. If compartment syndrome is suspected clinically (pain out of proportion, pain with passive stretch), compartment pressure measurement should be undertaken immediately.
Field dressings and splints must be removed to expose the entire leg, allowing the surgeon to assess soft tissue compromise, identify abrasions or fracture blisters, and rule out open fractures.
Radiographic evaluation requires orthogonal anteroposterior and lateral views of the entire tibia, including the knee joint. Furthermore, anteroposterior, lateral, and mortise views of the ankle must be obtained to rule out concomitant syndesmotic or physeal ankle injuries. Comparison radiographs of the uninjured contralateral extremity are rarely necessary but can be utilized in complex periarticular trauma. In the setting of a suspected toddler's fracture with negative initial radiographs, a technetium bone scan or magnetic resonance imaging may be obtained, though empirical casting and repeat radiographs at 10 to 14 days is often the most pragmatic approach.
For operative intervention, the patient is positioned supine on a radiolucent operating table. A bump is placed under the ipsilateral hip to correct natural external rotation, ensuring the patella points directly toward the ceiling. This facilitates true anteroposterior and lateral fluoroscopic imaging. A sterile tourniquet is placed on the proximal thigh but is rarely inflated unless severe hemorrhage is encountered or open reduction and internal fixation is required. The entire lower extremity is prepped and draped free to allow for dynamic manipulation and intraoperative assessment of alignment.
Detailed Surgical Approach and Technique
When non-operative management fails or is contraindicated, several surgical modalities are available. The choice of fixation depends on the fracture location, pattern, and the child's skeletal maturity.
Flexible Intramedullary Nailing Technique
Titanium elastic nails are the workhorse for diaphyseal pediatric tibia fractures requiring surgical stabilization. This technique relies on the principle of three-point fixation and symmetric construct elasticity.
- Incision and Entry Point: Two small longitudinal incisions are made approximately 1.5 to 2 centimeters distal to the proximal tibial physis, on the medial and lateral metaphysis. Care is taken to avoid the physis proximally and the tibial tubercle apophysis anteriorly.
- Cortical Window: An awl or drill is used to create a cortical window angled distally to facilitate nail insertion. The medial entry point is anterior to the medial collateral ligament, and the lateral entry point is slightly anterior to the fibular head to avoid the common peroneal nerve.
- Nail Selection and Contouring: Two titanium nails of identical diameter are selected. The combined diameter of the nails should equal approximately 80% of the narrowest diameter of the tibial isthmus. The nails are pre-contoured into a gentle "C" shape, with the apex of the curve corresponding to the fracture site.
- Insertion and Reduction: The nails are advanced sequentially down the medullary canal to the level of the fracture. Closed reduction is performed using manual traction and manipulation. The nails are then driven across the fracture site into the distal metaphysis.
- Final Positioning: The nails are advanced until their tips diverge in the distal metaphysis, stopping short of the distal tibial physis. The proximal ends are cut, leaving 1 to 2 centimeters protruding from the cortex to facilitate future removal, but seated deep to the subcutaneous tissue to prevent skin irritation.
Submuscular Plating Technique
For proximal or distal metaphyseal fractures where flexible nails provide inadequate stability, or for highly comminuted diaphyseal fractures, submuscular bridge plating is an excellent alternative.
- Incision: Small incisions are made proximal and distal to the fracture zone, respecting the physeal lines.
- Tunnel Creation: An extraperiosteal, submuscular tunnel is created along the medial or anterolateral aspect of the tibia using an elevator.
- Plate Insertion: A contoured locking compression plate is slid through the tunnel across the fracture site.
- Fixation: Following indirect reduction using manual traction or percutaneous clamps, the plate is secured with locking screws proximally and distally. The fracture hematoma is left undisturbed to promote secondary bone healing via callus formation.
External Fixation Technique
External fixation is primarily reserved for severe open fractures with extensive soft tissue loss, highly comminuted fractures in polytrauma patients, or as a damage-control orthopedic measure.
- Pin Placement: Half-pins are inserted percutaneously into the proximal and distal tibial fragments, staying well clear of the physes and the zone of injury.
- Construct Assembly: A rigid bar or circular frame is attached to the pins.
- Reduction: The fracture is reduced under fluoroscopic guidance, and the clamps are definitively tightened. External fixators can be used as definitive management or converted to internal fixation once the soft tissue envelope has recovered.
Compartment Syndrome and Fasciotomy
If compartment pressures exceed 30 mmHg of the patient's diastolic blood pressure (Delta P < 30), emergent fasciotomy is mandatory. The standard approach is a dual-incision technique.
- Lateral Incision: Placed halfway between the fibular shaft and the tibial crest. This accesses the anterior and lateral compartments. The fascial septum between the compartments is identified, and both fascial envelopes are released longitudinally.
- Medial Incision: Placed 2 centimeters posterior to the posteromedial border of the tibia. This accesses the superficial and deep posterior compartments. The saphenous vein and nerve must be protected. The soleus bridge is released to ensure complete decompression of the deep posterior compartment.
- Closure: Wounds are left open, managed with negative pressure wound therapy, and closed in a delayed fashion or covered with split-thickness skin grafts once swelling subsides.
Complications and Management
The management of pediatric tibial fractures is fraught with potential complications, ranging from benign radiographic anomalies to limb-threatening emergencies. Anticipation and early recognition are paramount.

One of the most unique complications in pediatric orthopedics is Cozen’s phenomenon, which occurs following proximal tibial metaphyseal fractures. The mechanism of injury usually involves a force applied to the lateral aspect of the extended knee, causing the medial cortex to fail in tension. Following healing, patients predictably develop a progressive valgus deformity of the proximal tibia. This is theorized to be caused by asymmetric hypervascularity stimulating the medial aspect of the proximal tibial physis, or due to a tethering effect of the intact fibula. The deformity typically peaks at 12 to 18 months post-injury. Management requires extensive parental counseling, as the vast majority of these deformities will spontaneously remodel and correct over 24 to 36 months. Early surgical intervention (osteotomy) is contraindicated due to the high rate of recurrence.
| Complication | Estimated Incidence | Pathophysiology and Salvage Strategy |
|---|---|---|
| Compartment Syndrome | 3% to 10% | Increased intracompartmental pressure. Requires emergent dual-incision fasciotomy. Delay leads to ischemic contracture. |
| Cozen's Phenomenon | Up to 50% in proximal metaphyseal fx | Asymmetric physeal stimulation causing valgus overgrowth. Observation is key; spontaneous resolution occurs in 2-3 years. |
| Leg Length Discrepancy | 10% to 20% | Hyperemia leads to overgrowth (typically 1 cm). Rarely clinically significant. Managed with shoe lifts if >2 cm. |
| Delayed Union / Nonunion | < 2% | Rare due to robust periosteum. Associated with open fractures or rigid fixation. Managed with dynamization, bone grafting, or revision fixation. |
| Angular Deformity | 5% to 15% | Intact fibula drives varus; premature weight-bearing causes apex anterior bowing. May require corrective osteotomy if remodeling potential is exhausted. |
| Hardware Irritation | 10% to 30% (with TENs) | Prominent nail tips irritate subcutaneous tissue. Managed with local wound care and routine hardware removal after fracture consolidation. |
Leg length discrepancy is another frequent complication. The hyperemic response to fracture healing stimulates the adjacent physes, often resulting in an overgrowth of the fractured tibia by approximately 1 centimeter. This is usually well tolerated and rarely requires intervention. Conversely, severe trauma can cause premature physeal arrest, leading to shortening or angular deformity, necessitating epiphysiodesis or lengthening procedures in the future.
Post Operative Rehabilitation Protocols
Rehabilitation following pediatric tibia and fibula fractures is highly dependent on the stability of the fixation construct, the age of the patient, and the presence of concomitant injuries. A phased approach ensures optimal biological healing while preventing joint stiffness and muscle atrophy.
Phase 1: Acute Healing (0 to 4 Weeks)
Regardless of operative or non-operative management, the initial phase prioritizes soft tissue rest and fracture consolidation. Patients treated with flexible intramedullary nails or plates are typically placed in a well-padded short-leg or long-leg posterior splint or bivalved cast to accommodate swelling. Weight-bearing is strictly prohibited (Non-Weight Bearing - NWB). Elevation of the limb above the level of the heart is critical to mitigate edema and reduce the risk of delayed compartment syndrome. Radiographs are obtained at 1 and 3 weeks post-operatively to ensure maintenance of reduction and assess early callus formation.
Phase 2: Callus Formation and Early Mobilization (4 to 8 Weeks)
Once bridging callus is visible on orthogonal radiographs, the patient is transitioned to a short-leg walking cast or a controlled ankle motion (CAM) boot. Weight-bearing is advanced to Weight Bearing As Tolerated (WBAT). Physical therapy may be initiated to focus on active and active-assisted range of motion of the knee and ankle joints. Strengthening exercises for the quadriceps and hamstrings begin, utilizing isometric contractions.
Phase 3: Remodeling and Return to Function (8 to 12+ Weeks)
By 8 weeks, most pediatric tibial fractures demonstrate robust clinical and radiographic union. Immobilization is discontinued. Rehabilitation focuses on restoring normal gait mechanics, proprioception, and full muscle strength. Return to high-impact sports or contact activities is generally delayed until 12 to 16 weeks, contingent upon complete radiographic obliteration of the fracture line and symmetric lower extremity strength.
Hardware removal is a routine consideration in pediatric orthopedics. Titanium elastic nails are typically removed in an outpatient surgical setting between 6 and 12 months post-operatively, once the fracture is fully consolidated and the medullary canal has reconstituted. Submuscular plates may be left in situ unless they cause symptomatic prominence or are perceived to tether longitudinal growth.
Summary of Key Literature and Guidelines
The management of pediatric tibial fractures is guided by a robust body of literature emphasizing the efficacy of conservative management and the precise indications for surgical intervention.
Current consensus guidelines dictate that closed reduction and cast immobilization remains the gold standard for closed, isolated tibial shaft fractures with acceptable alignment. Studies have consistently demonstrated that the robust pediatric periosteum and immense remodeling potential yield excellent long-term functional outcomes without the risks associated with surgery.
However, literature over the past two decades has shown a paradigm shift toward flexible intramedullary nailing for unstable, displaced, or length-unstable fractures, particularly in older children and adolescents. Comparative studies between casting and flexible nailing for unstable fractures indicate that operative intervention significantly decreases the length of hospital stay, reduces the time to independent ambulation, and minimizes the risk of malunion requiring late corrective osteotomy.
Regarding proximal metaphyseal fractures, seminal papers on Cozen’s phenomenon universally advocate for non-operative management of the initial fracture, utilizing an asymmetric long-leg cast molded into varus to counteract the deforming forces. The literature strongly cautions against early corrective osteotomy for the subsequent valgus deformity, as the hyperemic response of surgery frequently exacerbates the overgrowth, leading to recurrent and often more severe deformity. Observation remains the most evidence-based approach for this specific complication.
Clinical & Radiographic Imaging
